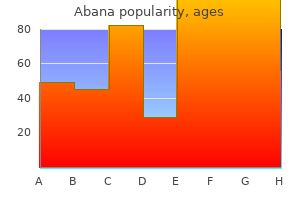
Abana
Abana dosages: 60 pills
Abana packs: 1 bottle, 2 bottle, 3 bottle, 4 bottle, 5 bottle, 6 bottle, 7 bottle, 8 bottle, 9 bottle, 10 bottle
Discount abana 60 pills visa
Supplemental Testing Gonioscopy and visual subject testing cholesterol test locations abana 60 pills buy discount on line, in addition to some technique for documenting the physical appearance of the optic nervehead � all are essential to set up each current status as properly as a baseline for future comparability cholesterol blood test name proven abana 60 pills. Careful questioning directed specifically at the issue of prior refractive surgical procedure ought to assist keep away from this downside. Some of those shall be volunteered in the center of routine questioning concerning ocular health. A sudden, profound, and lasting visible lower after central retinal vein occlusion, a preceding occasion for neovascular glaucoma, will usually be noted and reported by the affected person. Hazing of imaginative and prescient with vigorous train could additionally be a symptom of pigmentary glaucoma (from sudden release of pigment into the aqueous humor). Because imaginative and prescient clears to normal ranges inside hours, patients may not point out this spontaneously however will respond if requested specifically. The pain and blurred vision attribute of angle-closure glaucoma are sometimes distinctive factors in an ocular history. However, some patients with angle closure are so impressed by their headache during an assault that this becomes their predominant reminiscence. Further careful, directed questions, on this case triggered by finding a narrow angle on clinical examination, could develop a extra complete description of the symptoms. The evaluation course of must be continued on this recursive trend, from historical past to examination, back to historical past, and so on, until the best possible settlement between historical past and examination is developed. First of all, constructive household history is a vital risk factor for major open-angle glaucoma. The danger for primary open angle glaucoma is larger for first-degree family members of glaucoma sufferers than for the overall inhabitants. It is also useful to note whether or not the member of the family uses or used drugs only or whether surgical procedure was required. Frequently, affected person schooling will assist within the early detection of glaucoma in other at-risk family members, thus permitting glaucoma to be recognized earlier than the incidence of intensive damage to the eye. In addition, several of the childhood glaucomas have welldescribed hereditary patterns. Intense private expertise like this will have a optimistic impact by encouraging cautious adherence to treatment. Myopia is extra common in these sufferers than within the basic population (whereas hyperopia is decidedly extra common in main angle-closure glaucoma). Also, since glaucoma tends to develop within the older age teams, presbyopia is incessantly current. To rule out other mechanisms for glaucoma, one should inquire specifically concerning prior trauma (including surgery), inflammation (including potential steroid use), or an infection. These historic questions are sometimes triggered, or reemphasized, in the course of the examination. For example, a patient may deny any recollection of great trauma, yet the examination reveals a recessed chamber angle. In latest years, refractive surgical procedures have become extremely refined and effective, and increasing numbers of sufferers are choosing this technique of refractive correction. This could be unlucky, for the reason that corneal thinning produced by these procedures can cause marked underestimates of intraocular stress. The affected person is allowed to discuss what he or she perceives as important in the prevalence of the attention downside. Listening is an excellent route for establishing belief and dedication between affected person and physician. Thus, a foundation for a long-term relationship between the patient and the physician shall be created. However, in different circumstances, the periocular buildings may present clues, apparent or subtle, suggesting a coexisting glaucoma. A less apparent vascular abnormality, dilatation of the episcleral veins, could signal glaucoma brought on by an arteriovenous malformation elevating the episcleral venous strain. In addition to noting such specific glaucoma-related findings, the external examination should embody a seek for indicators of previous trauma, proptosis, restriction of motion, photophobia and tearing, and hyperemia. The pupillary responses are usually normal in primary openangle glaucoma, but there could also be an afferent defect within the event of severe nerve damage. Therefore, in addition to direct and consensual responsiveness, the pupils ought to be evaluated for size, quantity, form, and equality (preferably in each mild and dark). In addition, by way of the use of auxiliary optical devices, the slit-lamp biomicroscope turns into one of the most succesful means for analyzing the anterior chamber angle and the optic nerve head. The conjunctiva normally seems regular in major openangle glaucoma, as properly as in plenty of other types of glaucoma. Mention has already been made of dilated episcleral veins, which is a particular association with glaucoma. More generalized hyperemia is a nonspecific sign of inflammation or irritation and may be associated with several types of secondary glaucoma. Although initially normal, the conjunctiva may be altered later in the midst of glaucoma by an allergic or inflammatory reaction to drug treatment or via formation of drug deposits (adrenochrome) after long-term epinephrine instillation. The conjunctiva is, after all, an essential tissue within the context of filtering surgical procedure. Biomicroscopic examination of the cornea should include an overall assessment of readability, size, and vascularity, as properly as consideration to every tissue layer. There are particular findings in the cornea which are useful in the diagnosis of several of the secondary glaucomas. Not surprisingly, the cornea is generally normal for age in major open-angle glaucoma, until the intraocular pressure is high sufficient to trigger corneal edema. However, corneal edema is uncommon on the usually reasonable pressure levels of major openangle glaucoma. Corneal stromal scars are helpful markers of prior trauma or infection-inflammation. An more and more frequent explanation for stromal scarring is refractive surgery; an necessary discovering since it may sign inaccurate tonomety readings. Careful inspection of the stroma for signs of old interstitial keratitis � midstromal scarring and ghost vessels � is effective because these in any other case quiet eyes might purchase glaucoma as a late complication. A visible estimate of corneal thickness can be used to gauge the distance between the anterior floor of the peripheral iris and the posterior floor of the peripheral cornea in the periphery of the anterior chamber. In childish glaucoma, sudden stretching of the globe by stress could cause ruptures in this membrane. Several forms of glaucoma are related to characteristic alterations in or on the endothelial surface of the cornea. The regular anterior chamber is four to five corneal thicknesses deep centrally with its posterior extent defined by the lens and a comparatively flat iris plane, its anterior extent determined by the endothelial floor of the cornea. Moderate forward bowing could additionally be related to an elevated relative pupillary block or lens enlargement, or both. Backward bowing � a peripheral concavity of the iris � is a attribute finding in pigmentary glaucoma.
Abana 60 pills mastercard
Commonly presents between 3�9 months of age (less typically presenting at delivery or as much as ideal cholesterol to hdl ratio 60 pills abana discount fast delivery ~3 years of age) ldl cholesterol levels new zealand purchase 60 pills abana amex, and inflicting buphthalmos and blindness if not handled. Associated indicators of excessive stress within the toddler eye (in addition to the corneal stretching and opacity) embody deep anterior chamber, buphthalmos, myopia, and optic nerve cupping. Additional surgical procedures for refractory cases include trabeculectomy (sometimes combined with trabeculotomy by some surgeons), glaucoma implant surgical procedure, and cycloablation, along with medication use. Visual loss may result from corneal scarring and optic nerve harm, however often additionally happens due to amblyopia in unilateral or asymmetrical instances. Vision within the better seeing eye is a minimum of 20/50 typically the place glaucoma is stabilized after initial angle surgical procedure. Aggressive early management of glaucoma and attention to refractive errors and amblyopia, in addition to life-long follow-up of glaucoma, maximize visual outcome and high quality of life in affected children. Causes of Visual Loss in Primary Infantile Glaucoma Corneal scarring Cataracts Optic nerve injury Anisometropic amblyopia Strabismic amblyopia Retinal pigmentary adjustments, detachment (possible complication after filtration, seton, or cycloablative surgery) � � � � � � � � primary congenital glaucoma in 1938,four the visible outlook for affected youngsters was bleak. Although major infantile glaucoma is the most typical childhood glaucoma, this illness should be distinguished from other primary and secondary glaucomas in youngsters. The presence of associated ocular and systemic abnormalities, both congenital (in different primary glaucomas) or acquired (in secondary glaucomas), helps rule out major childish glaucoma. Juvenile open-angle glaucoma, a distinct inherited illness with onset in middle childhood to early maturity, must also be individually thought-about (see Chapter 199). A detailed classification system for the childhood glaucomas is introduced in Chapter 305. More than 80% of all sufferers have an onset of illness within the first yr of life, with ~25% diagnosed as newborns and greater than 60% presenting by 6 months of age. These authors suggest that the identification of these founder mutations in ethnically various populations suggests the next provider frequency for these older mutations in the studies populations, such that genetic testing for the founder mutations could lead to productive genetic counseling for congenital glaucoma. Primary infantile glaucoma and grownup open-angle glaucoma appear to be unrelated ailments. The probability of a second baby having the illness is no extra than 3% however may be as high as 25% if two youngsters have the disease (assuming autosomal recessive inheritance). Process of exposing the trabecular meshwork to the anterior chamber during improvement. Kupfer and Kaiser-Kupfer proposed the importance of neural crest cells within the normal growth of the anterior chamber angle. Faulty migration or differentiation of these cells was postulated to explain the defects noted in numerous forms of congenital glaucoma. These could include compression of the trabecular meshwork beams by a high iris and ciliary body insertion in addition to abnormal improvement of the trabecular meshwork itself. In children in whom glaucoma has its onset after 1 year of age, fewer overt signs and signs may occur due to the decreased expansibility of the attention. Even indoors, the toddler could present an obvious reluctance to face upward and could additionally be mistakenly thought-about shy. Blepharospasm or excessive blinking could also be yet another manifestation of photophobia, typically accompanying epiphora but without the mucoid discharge so usually seen in congenital nasolacrimal duct obstruction. This infant with main infantile glaucoma first introduced with tearing, photophobia, and corneal enlargement. This child showed an enlarged but clear proper cornea in early infancy, which was not acknowledged as major infantile glaucoma till he was three years old. Extensive optic nerve cupping was current, with myopic anisometropia and hand-motion vision. Associated cataracts, keratitis, and systemic findings (deafness, psychological retardation, cardiac anomalies) help distinguish this disorder, which is now turning into uncommon in trendy societies; a tribute to rubella immunization programs that prevent later maternal an infection. In oculocerebrorenal (Lowe) syndrome, an X-linked recessive situation, accompanying cataracts, microphthalmia, and systemic findings (aminoaciduria amongst others) assist distinguish this disease from major infantile glaucoma. For example, glaucoma might complicate uveitis and has been reported in the setting of storage disease, corneal dystrophy, congenital anomalies similar to Peters anomaly, and megalocornea. Glaucoma may even happen coincidentally with congenital nasolacrimal duct obstruction. At different instances, with a number of of these features absent, other diagnoses should be thought-about and excluded before a definitive diagnosis of main infantile glaucoma may be reached (Table 198. When epiphora, photophobia, or blepharospasm, or a mixture, accompanies a purple eye, ocular irritation (uveitis) and corneal harm or keratitis. Megalocornea is a uncommon, X-linked recessive disorder; households have been described during which some people have megalocornea alone, whereas others current with major infantile glaucoma. Asymmetry in diameter between the 2 corneas, or a corneal diameter of thirteen mm or more at any age, strongly suggests an abnormality. Corneal Diameter in Children: Normal and Glaucomatous Eyes Corneal Diameter (horizontal, in mm) Age Term (newborn) 1 year 2 years Older child Normal 9. Enlarged but clear corneas (14 mm diameter) persist on this baby after management of main infantile glaucoma. This symmetric optic nerve cupping has been attributed to stretching of the optic canal and backward bowing of the lamina cribrosa. Diagnostic Examination Every toddler and baby suspected of attainable major infantile glaucoma (or another sort of glaucoma) ought to have a full ophthalmic office analysis. The goals of this examination include (1) confirming or excluding the prognosis of glaucoma, (2) figuring out whether the glaucoma (if present) is primary childish glaucoma or a unique sort, and (3) acquiring extra medical information wanted to plan for subsequent anesthesia (for additional examination and surgery, if needed). This initial workplace examination could conclude the diagnostic course of if glaucoma may be confidently excluded. Additionally, relevant household history may be useful, as can any details about systemic abnormalities, attainable ocular trauma, or drug or treatment publicity. The office examination may be optimized by together with the use of a transportable slit lamp, millimeter ruler, TonoPen or Perkins tonometer (or both), and Koeppe diagnostic gonioscopic lenses. One can estimate corneal diameter by holding a millimeter ruler just in entrance of each cornea. Anterior Segment Examination the portable slit lamp provides details concerning the anterior section after tonometry has been carried out (or attempted). The typical corneal findings and abnormalities related to main infantile glaucoma have been described above. An unusually deep anterior chamber is commonly present in eyes with major infantile glaucoma. Iris or lens abnormalities might present clues to different diagnoses (such as aniridia or Axenfeld�Rieger syndrome). Gonioscopy, which can typically be performed within the office utilizing a Koeppe contact lens and a transportable slit lamp, helps determine the glaucoma sort and severity, quite than its presence or absence. Gonioscopy could be extra easily performed with the patient underneath anesthesia (unless glaucoma could be excluded by the workplace examination and findings). Imaging Techniques: Fundus pictures, Optical Coherence Tomography Fundus images of the optic disks has long been a mainstay within the analysis of adults with glaucoma over time, and is helpful in cooperative youngsters with clear visible axes and without substantial nystagmus. Unless the workplace examination adequately excludes the diagnosis of main infantile (or other) glaucoma, an examination with the patient beneath anesthesia (or sedation; see further ahead) is often warranted for additional analysis and doubtless for surgical intervention (see section on Treatment).
Trusted abana 60 pills
Regillo and associates reported such a case during which a successful vitrectomy was performed cholesterol ratio levels order abana 60 pills. In one family cholesterol ratio in canada 60 pills abana buy with mastercard, three boys who have been affected with congenital retinoschisis all developed retinal detachment. Fundus drawing of congenital retinoschisis with breaks within the internal (large black arrows) and the outer layers (small black arrow), causing a full-thickness retinal detachment. The third kind is a traction retinal detachment, which is similar to that of proliferative diabetic retinopathy in its fundus appearance and doubtless also in its mechanism of detachment; i. The retinal detachment thus created resembled a tabletop detachment, with the best retinal elevation at its point of adhesion to the fibrovascular membrane. The full-thickness retinal detachment caused by an outer layer break alone and not using a break within the inside layer seen in acquired retinoschisis has not been noticed in congenital retinoschisis. The aim of remedy in retinal detachment is to close all outer layer and full-thickness breaks. Regillo and associates reported surgical ends in six circumstances that developed complications: three with rhegmatogenous retinal detachment, one with exudative retinal detachment, and two with vitreous hemorrhage. A scleral buckle was used to treat the retinal detachments, and vitrectomies have been carried out to deal with vitreous hemorrhage and proliferative vitreoretinopathy that developed when the retina redetached. Fundus drawing of a traction retinal detachment in congenital retinoschisis with fibrovascular tissues from the disc. Blood within the vitreous (small arrows) and the dendritic figures attribute of congenital retinoschisis are seen on the 6:00 and 8:30 clock hour meridians (asterisks). Schema of the crosssection through the vertical line (white arrows) is also proven. Vitreous membranes Usually absent Vitreous hemorrhage Rare Retinal detachment Associated with different anomalies Rhegmatogenous None instances included those with overhanging inner layer retinoschises with blood within the schisis cavity blocking the macula without retinal detachment, and those with a traction detachment in the macula. However, the indications for removing the inner layer remain to be determined, significantly in instances of ballooning retinoschisis masking the macula with out the presence of a retinal detachment. In such instances, additional statement is an alternative as a outcome of blood-containing bullous retinoschises can collapse spontaneously. Congenital retinoschisis confined to the macula has never been a sign for remedy. However, Azzolini and colleagues reported a case during which the surgery resulted in decision of the macular schisis with good restoration of imaginative and prescient. Because Goldmann�Favre disease apparently impacts the retinal pigment epithelium in its early stage, along with the presence of the congenital retinoschisis, the medical findings of this disease are complex and generally misleading. The absence of typical peripheral retinoschisis makes diagnosing Goldmann�Favre illness more difficult as a result of the seen abnormality within the fundus is restricted to the macula, which may not present any attribute findings of retinoschisis. Besides the decrease of the a-wave amplitude, its implicit time is prolonged in all cases, as is that of the b-wave. A fundus appearance described as "a new clinical entity" and called enhanced S cone syndrome resembles that of Goldmann�Favre illness. No treatment is known to be efficient in Goldmann�Favre illness, but Garweg and associates handled two patients utilizing cyclosporine and bromocriptine. They hypothesized that this illness is a manifestation of a humoral and mobile immune response. As a results of cyclosporine treatment, the authors reported regression of the macular edema and flattening of the retinoschisis with subsequent improvement of imaginative and prescient. For instance, one often sees the peripheral retina elevated in young adults with regressed retinopathy of prematurity. Pigmentation is often seen within the connected retina or slightly indifferent at the edge and on both sides of the retinal elevation, typically associated with subretinal exudate. Secondary retinoschisis in proliferative diabetic retinopathy is relatively common. Lincoff and coworkers diagnosed eighty five cases of retinoschises and one hundred fifteen cases of traction retinal detachment among 200 cases of proliferative diabetic retinopathy with traction elevation of the retina. The inner layers are transparent, and circumscribed detachment of the outer layers is seen via the inside layers. The elevation of the inner layers is oval and far more in depth, speaking with the optic nerve pit. A uncommon case of hemorrhage within the macular retinoschisis cavity with an optic nerve pit was reported. Such treatment, nevertheless, is usually unsuccessful for retinoschisis associated with an optic pit. The fundus reveals blood-filled retinal cysts which would possibly be often massive and a quantity of and concentrated within the posterior pole. Subsequently, the blood migrates from the retina into the vitreous, leaving a retinal scar and markedly slender retinal arteries. Autopsy findings demonstrated a number of hemorrhages within the inner retina and within the preretinal, intrachoroidal, and intrascleral spaces in the area of the circle of Zinn�Haller. Prevalence and long-term natural course of retinoschisis among aged individuals: the Copenhagen City Eye Study. Yassur Y, Nissenkorn I, Ben-Sira I, et al: Autosomal dominant inheritance of retinoschisis. Optical coherence tomography of a peripheral retinal schisis with an outer retinal layer break. Clements S, Busse H, Gerding H, Hoffman P: Treatment pointers in various phases of senile retinoschisis. Schwarze U, Laqua H: Retinoschisis mit zentral gelegenem Aussenschichtriesenress und Begleitamotio. Huopaniemi L, Rantala A, Tahvanainen E, et al: Linkage disequilibrium and bodily mapping of X-linked juvenile retinoschisis. Pearson R, Jagger J: Sex linked retinoschisis with optic disc and peripheral retinal neovascularisation. Hirose T, Wolfe E, Hara A: Electrophysiological and psychophysical research in congenital retinoschisis of X-linked recessive inheritance. Granit R: Sensory mechanisms of the retina with an appendix on electroretinography. Miyake Y, Shiroyama N, Ota I, Horiguchi M: Focal macular electroretinogram in X-linked congenital retinoschisis. Alitalo T, Forsius H, Karna J, et al: Linkage relationships and gene order around the locus for X linked retinoschisis. Gellert G, Petersen J, Krawczak M, et al: Linkage relationship between retinoschisis and four marker loci. Ruether K, van de Pol D, Jaissle G, et al: Retinoschisis-like alterations within the mouse eye attributable to gene focusing on of the Norrie disease gene. Kageyama M, Nakatsuka K, Miyake Y: A case of congenital retinoschisis with surprising look and spontaneous regression. Turut P, Francois P, Castier P, et al: Analysis of ends in treatment of peripheral retinoschisis in sex-linked congenital retinoschisis. Ricci A: Clinique et transmission g�n�tique des diff�rentes formes de d�g�n�rescences vitr�o-r�tiniennes. Fran�ois J, Van Oye R: D�g�n�rescence hyalo�d�o-tap�to-r�tinienne de GoldmannFavre.
60 pills abana buy mastercard
Resistance was related to prior intravenous cidofovir use or prior oral ganciclovir use cholesterol medication safe during pregnancy order abana 60 pills. The pellet is coated with polyvinyl alcohol (which is permeable to ganciclovir) and ethylene vinyl acetate (which is impermeable) cholesterol in eyes 60 pills abana with visa. The launch fee of about 2 mg/h is decided by the thicknesses of the coatings of the 2 polymers, offering launch of drug for about 7�8 months. A stable intraocular focus of ganciclovir is obtained within 24�48 h and is roughly fourfold greater than that obtained with intravenous therapy. Because of these potential complications, the implant is prevented if immune reconstitution is anticipated except zone 1 is concerned. However, its tedious intravenous administration schedule coupled with its facet impact profile, especially nephrotoxicity, has made it a much less desirable first-line therapy. Systemic therapy may take several weeks or extra to control retinitis and subsequently will not be adequate in the initial treatment of lesions near the fovea or optic nerve. In these cases, immediate intravitreous injections of ganciclovir or foscarnet, followed by placement of a ganciclovir implant, may be more practical. Unfortunately, the sensitivity and optimistic predictive worth for these markers were low, limiting their international clinical utility. The retinitis can start within the macula or in the periphery with patchy, multifocal outer retinal lesions coalescing quickly all through the retina within the absence of vascular or vitreous inflammation. Severe visible loss from the diffuse retinal necrosis, optic atrophy, and retinal detachment occurs in as much as 70% of sufferers. Some sufferers have extreme imaginative and prescient loss regardless of minimal or absent retinitis on account of early optic nerve involvement; in these sufferers, the onset of ache with vision loss could also be a key discovering. A regimen of intravitreal foscarnet and ganciclovir as well intravenous administration of each medicine was related to 45% of sufferers having a vision of 20/80 or better. This same research advised that laser demarcation could end in better outcomes as properly due to a decrease threat of retinal detachment. Reactivation is documented with the reappearance of opacification of the border of the lesion and advancement of the lesion borders or the event of latest lesions. Reinduction remedy with a higher dose of drug or by switching from one drug to one other, combined remedy with intravenous ganciclovir and foscarnet has been shown to be twice as effective as both drug alone in delaying additional progression72; however, the added toxicity of the second drug makes combination therapy troublesome to administer and reduces quality of life. In circumstances by which drug resistance is the purpose for development, a change from ganciclovir to foscarnet or cidofovir could also be needed. Some of the unwanted effects embody headache, dysgeusia, diarrhea, and nausea which are dose related. The choroiditis takes from 6 weeks to 4 months to resolve after treatment with double strength trimethoprim-sulfmethoxazole. In immunocompromised patients, ocular involvement is far much less frequent than central nervous system toxoplasmosis. The various shows vary from acute anterior uveitis to panophthalmitis with a secondary orbititis. For patients allergic to sulfa drugs, azithromycin, atovaquone, and clindamycin with pyrimethamine/leucovorin may be efficient. Varicella zoster virus and herpes simplex virus have each been related to this illness. The retinitis is marked by deep retinal whitening, restricted hemorrhage hemorrhage, and a speedy development over days to weeks. Dense vitritis produces fibrotic bands that exert traction on necrotic retina resulting in advanced retinal detachments in 75% of patients and blindness in 64% of patients inside 2�3 months. Proliferative vitreoretinopathy often accompanies the retinal atrophy in the end-stages of the illness. Therapy consists of intravenous acyclovir followed by indefinite oral remedy with acyclovir, valacyclovir, or famciclovir. Laser demarcation along the posterior border of the retinitis is indicated to cut back the danger of retinal detachment. Chorioretinitis and endophthalmitis are each thought to outcome from direct invasion of the organism usually via neural tissue. The chorioretinitis that outcomes is characterized by perivascular retinal lesions with minimal irritation. Prophylactic treatment with aerosolized pentamidine alone is associated with an increased danger of Pneumocystis carinii choroidopathy, characterised by pale, multifocal, cream- to orange-colored plaques ranging in dimension from 300�3000 mm deep in the mid-peripheral and posterior choroid. The illness characteristically begins within the oropharynx and disseminates to lymphoid tissue. In immuno compromised patients, it can end result from reactivation of a 2102 Retinal Manifestations of the Acquired Immunodeficiency Syndrome: Diagnosis and Treatment quiescent lesion since cell-mediated immunity keeps the infection dormant. This fulminant infection can cause a complete retinal detachment with marked vitritis and iridocyclitis and in one case resulted in enucleation. Because intravenous amphotericin has poor intravitreal penetration, vitrectomy and intravitreal amphotericin B are recommended adjunct therapy for sightthreatening endophthalmitis. At the time of a pars plana vitrectomy, the vitreous washings in the cassettes can be plated for cultures and cytology to further tailor therapy. In the operating room, a complete peritomy is carried out with isolation of the four recti muscles. A half-thickness scleral trapdoor dissection is performed with preplaced sutures, allowing fast closure of the wound, and is surrounded by cautery. Some advocate performing a pars plana vitrectomy previous to choroidal sampling to assist in the upkeep of intraocular pressure. Endoretinal biopsy may be carried out on the time of repair of rhegmatogenous retinal detachment in patients with viral retinitis. Hematogenous dissemination of Mycobacterium tuberculosis to the choroid leads to single or a quantity of round, yellow-white elevated lesions with indefinite borders starting from zero. Tuberculous choroiditis responds properly to systemic remedy with rifampin, ethambutol, isoniazid, and pyrazinamide. These brokers are associated with a hypersensitivity response that affects the whole class of agents. Protease inhibitors are often associated with gastrointestinal intolerance and metabolic abnormalities. It inhibits fusion of the viral envelope glycoprotein (gp41) with the host cell membrane. These medication cause inhibition of the nitrous oxide pathway and have been linked to anterior ischemic optic neuropathy. The agents should be phosphorylated by host cell enzymes in the cytoplasm to become active. Hence, quarterly oblique ophthalmoscopy ought to be performed in children on this medication.
Order abana 60 pills on line
If main childish glaucoma has been beforehand cholesterol in eggs and heart disease order abana 60 pills without prescription, or by this time cholesterol jfk ratio abana 60 pills mastercard, confirmed, one could proceed directly to appropriate surgical intervention (see section on Treatment). The whole examination beneath anesthesia can usually be achieved using a mask only, reserving endotracheal intubation until the need for surgical intervention has been confirmed within the working room. Examination Under General Anesthesia: Suggested Sequence Tonometry (as early as potential after induction and before intubation) External examination (brief) Anterior phase examination Corneal diameter measurement Koeppe gonioscopy Fundus examination (optic disc) Ultrasound pachymetry to measure central corneal thickness (omit if edema present) Ultrasound (axial length measurement and/or B-scan if indicated) Optic nerve pictures, refraction (if pupil massive or dilated) Surgical intervention constitutes the definitive remedy modality for major childish glaucoma, although medications play an adjunctive role. Angle surgical procedure (goniotomy or trabeculotomy) ought to be attempted as the initial process typically (see further ahead). The youngster with glaucoma usually adheres to his/her prescribed ocular drugs quite well in the early years, especially when strong family support is present. Most of the commercially available glaucoma medication within the United States at present have been approved with none information on their security in children. When administered orally with meals or milk three or four instances day by day (total dose 10�20 mg kg�1 day�1), acetazolamide is often well tolerated. The metabolic acidosis that has been reported in infants could additionally be ameliorated with oral sodium citrate (Bicitra) (1 mEq kg�1 day�1). In a small cross-over trial, eleven kids whose glaucoma was controlled on topical b-blockers and oral acetazolamide switched from the oral acetazolamide to topical dorzolamide tid within the examine eye. Using Topical Glaucoma Medications in Congenital Glaucoma Medication (Class, Name) Beta-Blockers Nonselective (timolol, and so forth. Miotics Miotic drugs have a restricted function in treating sufferers with major childish glaucoma, perhaps in part because of the abnormally excessive insertion of the ciliary muscle into the trabecular meshwork. Older (phakic) kids typically undergo substantial visible blur attributable to miotic-induced ciliary spasm and resultant myopia. Several studies have examined the role of timolol in treating uncontrolled childhood glaucomas, but none has addressed solely main infantile glaucoma sufferers. Although unusual, systemic unwanted facet effects can occur in youngsters treated with topical b-blockers. The most extreme of those have included acute bronchial asthma assaults, bradycardia,113,a hundred and fifteen and apneic spells (the latter in neonates). Topical b-blockers should be used with excessive caution in neonates, who may be especially prone to apnea. As a comparatively b1-selective drug, betaxolol (Betoptic) may be much less probably than the nonselective b-blockers to precipitate acute bronchial asthma assaults in kids (which may present as coughing). The remaining nonselective b-blockers could be anticipated to display dangers and efficacy much like that of timolol. Its use must be prevented altogether in infants and in small and underweight children, because of its propensity to cause severe systemic side effects. Topical brimonidine administration has caused bradycardia, hypotension, hypothermia, hypotonia and apnea in infants, and severe somnolence in toddlers. Angle Surgery the introduction of angle surgery (first goniotomy after which trabeculotomy ab externo) has drastically improved the previously dismal prognosis for youngsters with major infantile glaucoma. Both goniotomy and trabeculotomy ab externo have their staunch advocates, however neither procedure has been definitively proved better than the other for treating main infantile glaucoma. Reported success has been equally excessive (from ~80 to >90%) with both procedures in favorable circumstances of glaucoma. Goniotomy Goniotomy, a process supposed to incise the uveal trabecular meshwork beneath direct visualization, was introduced as an operation for major congenital (infantile) glaucoma by Barkan in 1938. The goniotomy process remains basically as Barkan described it ~60 years ago, underscoring its importance and widespread use because the preliminary procedure for major infantile glaucoma. Gonioscopy performed with the affected person underneath anesthesia before surgery confirms whether the angle visualization is enough for goniotomy. Several drops of sodium chloride 5% can help in decreasing corneal haze from edema, to maximize the gonioscopic angle view. A Barkan goniotomy lens modified with an added handle, and placed onto a mound of healon on the central cornea works well. The nontapered Swan knife (or needle-knife) enters the anterior chamber simply and cuts in both direction. The needle is single-use, readily available, and at all times sharp; further its uniform shaft diameter maintains the deep anterior chamber because the instrument is withdrawn after incision. Postoperative care of the infant eye typically challenges the parents and surgeon alike. The goniotomy knife or needle then enters via peripheral clear cornea 1 mm from the limbus, opposite the midpoint of the supposed goniotomy. A cleft of whitish tissue may be noted in the wake of the incision, with a widening of the angle. After careful removing of the knife or needle, blood often egresses from the angle incision, normally stopping when the chamber is refilled. Postoperative treatment features a topical antibiotic and steroid, as properly as pilocarpine drops. Bilateral goniotomies could also be performed throughout one anesthesia supplied all instruments are replaced or sterilized; all drapes, gowns, and gloves replaced; and the man eye reprepared and draped in sterile style after the first procedure. Burian and Smith independently described this procedure in 1960 as a substitute for goniotomy. Trabeculotomy, carried out with either a limbus- or a fornixbased flap, uses a partial-thickness triangular or rectangular scleral flap (as created for traditional trabeculectomy), ideally positioned temporally (to spare superior conjunctiva). The anterior chamber often shallows slightly, with egress of blood from the torn trabecular meshwork, because the trabeculotome is faraway from the attention. The scleral flap is then secured with 10�0 nylon or Vicryl, whereas the Tenon and conjunctival layers may be closed with a working suture of 8�0 or 10�0 absorbable suture, as for normal trabeculectomy. Trabeculotomy, beneath a limbus-based conjunctival and partial-thickness scleral flap. If mitomycin C has been utilized, the use of an oblong partial-thickness scleral flap and a subsequent separate working closure of both the Tenon and the conjunctival layers with 10�0 absorbable suture is favored. Postoperative care must be as for pediatric trabeculectomy in this case (see section on Trabeculectomy). Although angle surgical procedure alone is taken into account commonplace initial surgical management for main congenital glaucoma by many surgeons, some do advocate combined trabeculotomy and trabeculectomy as an alternative, with excellent surgical success (66% at 5 years). Additional challenges to success embrace difficulties in the postoperative care of youngsters, as well as visual loss from amblyopia even if glaucoma has been managed. Although most glaucoma filtration surgical procedure in kids was standardly carried out utilizing a limbus-based conjunctival incision, many surgeons performing trabeculectomy in both adults and kids now advocate fornix-based incisions. Intraoperative beta irradiation, used in Britain, elevated success of trabeculectomy from ~40% to greater than 65%. Postoperative care and issues of this process in kids are just like those in adults, except that periodic examinations underneath anesthesia are usually required in young youngsters. The presence of thin-walled avascular filtering blebs in pediatric sufferers after mitomycin C-augmented trabeculectomy raises critical concern about the lifetime risk of the development of endophthalmitis, bleb leaks, and wound rupture with minor trauma in these eyes (all of which have already occurred). Most common among the many latter in plenty of sequence were contact between the tube and the corneal endothelium (tube�cornea touch), erosion of the tube externally through the conjunctiva, migration of the tube, and cataract formation or development.
Abana 60 pills purchase with amex
Other treatment methods have been investigated total cholesterol hdl ratio diabetes 60 pills abana generic otc, together with a randomized trial comparing a total dose of 1000 rad versus 2000 rad/orbit with percent of cholesterol in shrimp abana 60 pills buy low price, no remedy difference detected between the two doses. Orbital radiation could cause detrimental effects to the eye and surrounding tissues (Table 230. Shielding the anterior eye usually protects towards harm to the lacrimal gland and lens. The threat is highest for sufferers with a predisposing vascular situation, such as diabetes, however microvascular modifications have been reported even in patients without known retinopathy threat factors. The randomized scientific trials of radiation therapy have excluded sufferers with optic neuropathy, as a result of moral concerns about treating these sufferers with sham therapy. The greatest proof supporting radiation for optic neuropathy therefore comes from nonrandomized trial knowledge. The most appropriate treatment strategy is set by severity of the optic neuropathy, affected person age and medical status. Surgical decompression creates more space for the swollen tissues by increasing the partitions of the orbit (bony decompression) or by eradicating excess orbital fats (fat decompression). The primary indications for orbital decompression are compressive optic neuropathy and extreme proptosis. Excessive proptosis can manifest as globe subluxation, corneal ulceration, and beauty disfigurement. Orbital decompression surgery additionally has a role in sufferers with reasonable proptosis who require strabismus surgical procedure. In these sufferers, launch of tight rectus muscular tissues could permit ahead movement of the globe, thereby worsening the preexisting proptosis. Other indications for orbital decompression surgery embody improved cosmesis, steroid dependence, and intractable ache. The many approaches to orbital bony decompression can be categorized based on the surgical strategy to the orbit (transantral, lateral, transfrontal/coronal, transconjunctival, transcaruncular, endoscopic transnasal), or on the number of bony partitions removed (one, two, three, or four wall). Experimental and clinical studies show that the quantity of proptosis discount increases with the variety of orbital partitions decompressed. A one-wall decompression usually yields 0�4 mm proptosis discount, a two-wall decompression 3�7 mm, a threewall decompression 6�10 mm, and a four-wall decompression 10�17 mm. The selection of specific surgical technique is dependent upon the indication for surgery. With this information, the surgeon can more accurately counsel the patient on the expected quantity of decompression and the chance of postoperative complications corresponding to diplopia and hypesthesia. When decompression is carried out for optic neuropathy, a medial wall decompression usually permits essentially the most direct entry to the orbital apex. Potential approaches to the medial wall embody transcaruncular, transnasal endoscopic, transantral, and transcutaneous. Successful decompression for optic neuropathy is achievable via any of those routes. A medial decompression could be mixed fairly readily with a decompression of the orbital ground to increase the amount of decompression. With any method to decompress the medial wall and orbital floor, the risk of postoperative diplopia and hypoglobus may be minimized by retaining the bony strut within the inferomedial orbit. Advantages to leaving the rim intact embody decreased surgical time to take away and exchange the bone flap, lack of imaging artifact postoperatively, preservation of the lateral canthal tendon attachments, and talent to measure postoperative proptosis using an exophthalmometer in opposition to the lateral orbital rim. The anterior aspect of the lateral wall may be decompressed into the temporalis fossa. For this technique, a drill and bone curette are used to remove bone to the extent of the inner table, where bleeding is encountered. Potential complications of the strategy embrace scarring of the scalp, and neuralgia of the supraorbital nerve. In a sequence of more than 400 orbital decompressions, only 10 patients required decompression of the roof. The orbit may additionally be decompressed by orbital fats removal, both at the side of bony decompression or as a standalone procedure. In these cases, fats decompression has been reported to reverse optic neuropathy in patients who had failed prior steroids and/or orbital radiation. On the right facet, a limited lateral decompression was mixed with a medial decompression. On the extra proptotic left side, an aggressive deep lateral decompression was mixed with medial decompression. The lateral partitions had been each removed with high-speed drills and the orbital rims had been left intact. The enlarged medial rectus muscle has prolapsed medially, with aid of optic nerve compression. The left decrease eyelid retraction has worsened, as is frequent following inferior rectus recession. Prior decompression can also lead to challenging strabismus patterns, together with large-angle esotropia and torsional diplopia. The optimum timing of surgical procedure is controversial, with some surgeons advocating ready for stable measurements a minimal of 6 months aside and others favoring earlier surgical procedure. The aim of strabismus treatment is to achieve single binocular imaginative and prescient in main and downgaze positions. Others, however, feel that the alignment within the instant postoperative period differs substantially from the longer-term result and therefore advocate using fixed suture strategies. Conservative maximal quantities of muscle recession should be used to keep away from finding muscular tissues too near the globe equator, thus altering the mechanical fulcrum of muscle motion and decreasing its range of motion. As with any strabismus surgery, the surgeon ought to limit the number of operated rectus muscles to no extra than three per eye to keep away from anterior section ischemia. If diplopia persists longer than 6 weeks after surgery, extra surgery could be carried out. The pathophysiology of lower eyelid retraction is similar, although the decrease lid retractors are less properly outlined than are those of the upper lid. Soft tissue infiltration or orbital congestion could cause diffuse fullness of the upper and decrease eyelids in addition to extra focal expansion of the eyelid and orbital fats. Additionally, surgical debulking of excess skin and fats can restore a more normal appearance to the eyelids. Eyelid surgery ought to be undertaken after orbital decompression and extraocular muscle surgery, because both procedures can have an result on eyelid position. The most typical eyelid abnormality following transantral decompression is lower eyelid entropion. Eyelid surgery is usually carried out a minimal of 6 weeks after orbital decompression or the ultimate strabismus process, though eyelid surgical procedure may be undertaken in conjunction with decompression or strabismus surgical procedure. Advantages of the anterior method include a more familiar display of the eyelid anatomy, access to the anterior eyelid tissues if pores and skin or fats removal is necessary, and the flexibility to extra aggressively deal with eyelid retraction.
Buy abana 60 pills free shipping
Most sufferers were from nonendemic areas and had vitritis and decreased electroretinogram alerts cholesterol levels definition 60 pills abana safe. Of sixteen sufferers who underwent skin testing cholesterol levels of meats abana 60 pills without a prescription, only 5 examined optimistic for histoplasmosis. This syndrome is very troublesome to differentiate from birdshot choroidopathy and diffuse unilateral subacute neuroretinopathy. Deutsch and Tessler64 reported comparable findings, nevertheless 43% of their patients have been black. Gass56 believes the punched-out lesions fluoresce but that this is due to scleral reflection and not precise leakage of dye. The electroretinogram is depressed, and fluorescein angiography reveals disc leakage and cystoid macular edema. Systemic signs such as tinnitus, deafness, poliosis, vitiligo, and headache happen. At 36 months, the outcomes had been 45% for the group receiving no treatment and 10% for the treated group. Aphthous oral ulcers and genital lesions often accompany the attacks of uveitis. Many years ago, Schlaegel and colleagues45 thought-about systemic steroids to be acceptable for acute flare-ups and possibly for long-term use to prevent visual loss. Schlaegel65,66 believed that steroids, if used, ought to be given in excessive doses (prednisone 60�100 mg/day) and tapered very slowly over 1�2 yr. Makley and co-workers67 found some profit if steroids were used early in the center of macular lesions. There are a number of benefits of krypton purple laser, together with less lens scatter, much less absorption by xanthophyll, and fewer internal retina injury. Complications of Laser Treatment Recurrence of choroidal neovascular membrane Retinal pigment epithelial rips Acute choroidal hemorrhage Nerve fiber layer field defects Premacular fibroplasia cooperative sufferers. The fluorescein angiogram getting used to guide treatment must be less than 72 h old, particularly with juxtafoveal lesions. Because of eccentric fixation or distortion of the fovea, one could also be fooled into treating the fovea if the aiming beam is used to determine fixation. The patient ought to be introduced to the sound of the laser before treatment really begins. One ought to use a computer monitor (for digital angiograms), a table-top viewer (for film angiograms) adjoining to the laser slit lamp. If bleeding happens during the laser remedy, intraocular strain must be increased with the contact lens after which laser therapy utilized over the bleeding website, ideally with argon green. Gass83 recommends covering any pigment ring and choroidal neovascularization as proven by an early body of the fluorescein angiogram. Several danger components have been statistically related to recurrences, including hypertension, cigarette smoking, proximity to fovea, younger age, and female gender. Seventy-one percent of the eyes with perfused subfoveal choriocapillaris had visual enchancment postoperatively versus only 14% of these not perfused. A profitable end result was defined as a 24 month visual acuity higher or no a couple of line (seven letters) worse than at baseline. Forty-six % of the eyes in the observation arm and 55% within the surgery arm had a profitable consequence (success ratio 1. Median visual acuity on the 24 month examination was 20/250 for eyes within the statement arm and 20/160 for eyes within the surgical procedure arm. In a subgroup of eyes with preliminary visual acuity worse than 20/100, surgical procedure was extra profitable; 76% of forty one eyes within the surgery arm versus 50% of forty eyes within the noticed arm at the 24 month examination had a successful outcome (success ratio 1. Four percent of eyes within the surgery arm skilled rhegmatogenous retinal detachment. Twenty-four % of eyes developed postvitrectomy cataract, all in patient over the age of fifty years. However, they did recommend submacular surgical procedure for the subgroup of eyes with visible acuity worse than 20/100. Vision-targeted high quality of life improved more after submacular surgery than with statement, supporting a possible small general good factor about surgery. Natural historical past studies recommend that solely 14�16% of these patients recover visual acuity of 20/40 spontaneously without remedy. These authors reported improvement of preoperative median visible acuity of 20/200 to 20/40 at 7 months follow-up. Ten patients (45%) gained 7 or extra letters of visual acuity while 4 (18%) patients misplaced eight or more letters, including two sufferers (9%) who misplaced at least 15 letters. There was no leakage on the fluorescein angiogram in 85% of the evaluable lesions. The outcomes of the above prospective study corroborated an earlier retrospective evaluation printed by Busquets et al in June 2003. Visual acuity improved or stayed the same in 69% of eyes, improved by at least two strains in 44%, and improved by greater than four lines in 22%. This retrospective sequence had variable follow-up and included some eyes (38%) that had undergone prior submacular surgical procedure. The authors of this chapter have anecdotal expertise with pegaptanib and bevacizumab, and believe that this type of remedy (along with ranibizumab) will probably show helpful for this disease. A 23-year-old white male introduced with blurred vision and distortion of 1 week period within the left eye. In truth, one yr in the past, he offered with similar symptoms and was felt to have choroiditis of a juxtafoveal macular histo spot. He refused thermal laser and subsequently underwent photodynamic therapy with verteporfin. Because of worsening signs and increased fluorecsein angiographic leakage, an intravitreal injection of pegaptanib was given. Thirty p.c of eyes gained a minimal of 5 letters, 20% lost 5�14 letters, and 50% maintained stable visual acuity. Interestingly, reported side effects included transient intraocular pressure elevation and gentle cataract development, well known complications of intravitreal corticosteroids. This grid can be used at residence by sufferers at risk for the event of new vessel membranes. Patients with macular chorioretinal scars are in danger for the development of choroidal neovascularization that can threaten central imaginative and prescient. I: Histoplasmin pores and skin check sensitivity in cases recognized during a community survey. Macular Photocoagulation Study Group: Five-year follow-up of fellow eyes of people with ocular histoplasmosis and unilateral extrafoveal or juxtafoveal choroidal neovascularization. Kranias G: Vitreous hemorrhage secondary to presumed ocular histoplasmosis syndrome. Macular Photocoagulation Study Group: Argon laser photocoagulation for neovascular maculopathy-Three-year outcomes. Macular Photocoagulation Study Group: Krypton laser photocoagulation for neovascular lesions of ocular histoplasmosis.
Buy cheap abana 60 pills on line
The disk could seem regular initially cholesterol in large shrimp abana 60 pills cheap line, however an afferent pupillary defect could also be present cholesterol lowering food products abana 60 pills cheap amex, and later optic disk edema adopted by atrophy may develop. Fluorescein angiography could present leakage of dye in the area of the white retinal patches, retinal and disk edema, venous staining, and areas of capillary nonperfusion. The retinal hemorrhages and white patches resolve over several months, though the affected person could also be left with some loss of imaginative and prescient secondary to pigmentary macular modifications and optic atrophy. The blood normally clears spontaneously; however, in instances of nonclearing vitreous hemorrhage, vitrectomy could additionally be beneficial. There may be associated vitreous hemorrhage or dissection of blood beneath the retina. The presumed mechanism of retinal hemorrhage is rupture of superficial retinal capillaries owing to a sudden improve in retinal venous strain after the speedy increase in intrathoracic or intraabdominal pressure related to a Valsalva maneuver, corresponding to coughing or vomiting. This 22-year-old man famous decreased vision and a central scotoma instantly after a coughing episode three weeks earlier than presentation. Note the bilobed look of the preretinal hemorrhage, now yellow because of hemolysis. Along the inferior margin of the hemorrhage, blood can be seen breaking through the inner limiting membrane and extending into the vitreous cavity inferiorly. One month later, the hemorrhage had nearly fully resolved, and imaginative and prescient improved to 20/20. Harissi-Dagher M, Sebag M, Gauthier d, Marcil G, et al: Photodynamic therapy in younger patients with choroidal neovascularization following traumatic choroidal rupture. Garcia-Arumi J, Corcostegui B, Cavero L, et al: the role of vitreoretinal surgery in the treatment of posttraumatic macular gap. Harcourt B, Hopkins D: Permanent chorioretinal lesions in childhood of suspected origin. Boulton Spectral dependence of phototoxicity or absorption Light may cause photomechanical, photothermal, or photochemical retinal damage. Photic retinopathy is produced experimentally by extended intense gentle exposures ranging from seconds to hours at illuminances exceeding normal environmental levels that may in all probability be properly tolerated if experienced solely briefly. Photochemical retinal harm has additionally provided useful perception into the molecular biology of retinal degeneration. The absorption spectra of rhodopsin in rod photoreceptors and melanopsin in light-sensitive ganglion cells are comparable in type but peak at ~500 nm249 (blue-green) and 480 nm (blue),67�69 respectively. Violet (400�440 nm) and blue (440�500 nm) gentle comprise the shorter wavelength portion of the seen spectrum. Thermal and photochemical retinal injury happen when photons are absorbed by chromophores, the light absorbing parts of biomolecules. Melanin, hemoglobin, and macular xanthophyll are the simplest retinal mild absorbers. Other retinal gentle absorbers embrace lipofuscin, rhodopsin, cone photopigments, melanopsin, porphyrins, and cytochrome c oxidase. Absorption spectra describe how effectively tissue chromophores seize photons at totally different wavelengths. Absorption spectra for molecules corresponding to hemoglobin or rhodopsin have peaks at specific wavelengths, with decrease absorption at adjacent wavelengths. When photon absorption induces damaging reactive oxygen species, spectra that describe the effectiveness of photon seize at totally different wavelengths are often known as action spectra. Action spectra characterize how successfully completely different optical radiation wavelengths produce photochemical results. Energy could be transformed into increased average molecular vibrational movement, raising retinal temperature and inflicting photocoagulation when tissue temperature elevation is sufficiently excessive. Alternatively, if photon power is coupled effectively to chemical bonds in goal molecules, extra molecular electronic vitality from photon absorption can break those bonds, producing photochemically induced structural changes within the molecules. Reactive oxygen species are highly reactive oxygen radicals with the capacity to modify and harm cell membranes, proteins, carbohydrates, and nucleic acids. In addition, there are oxygen species during which electron pairing is regular but the molecule is in an excited state. Singlet oxygen is the lowest excited state of the di-oxygen molecule, its lifetime in resolution is within the microsecond vary, and it reacts readily with membrane lipids. Reactive oxygen species can react either directly with goal tissues (type-1 photochemical or free radical reactions) or with molecular oxygen to produce singlet oxygen or superoxide which then reacts with target tissues (type-2 photochemical or photodynamic reactions). Apoptosis removes unneeded, injured, or diseased cells, spanning a broad complex of interrelated mechanisms for signaling and producing cell dying. Blue-green retinal phototoxicity in rodents was discovered by Werner Noell in 1966. A photoreceptor photopigment consists of an 11-cis retinal chromophore molecule sure to a transmembrane opsin protein in a photoreceptor outer segment disk. Most experimental research of photopigment-mediated retinal phototoxicity use rodent models and protocols that differ in retinal irradiance, publicity period, supply wavelength, animal species, antioxidant status, and circadian timing. A vital discovering is that native rhodopsin focus throughout a rodent retina is inversely proportional to local illuminance. Experimental studies have shown that cones have lower photo- toxicity susceptibility than rods in rodents87 and greater susceptibility in pigeons and primates. Lipofuscin could impair antioxidant activity, produce phototoxic harm or mechanically compromise mobile perform. A2E is a retinoid cycle byproduct, formed from phosphatidylethanolamine and two molecules of all-transretinaldehyde. An acute solar injury produces a yellowish-white foveola lesion, as seen on this 15-year-old female with 20/70 visible acuity. Welding arc accidents usually produce yellowish-white foveolar lesions just like these seen in photo voltaic maculopathy, as illustrated on this 17-year-old male 3 days after a welding arc publicity. Solar remark with a dilated 7 mm pupil or telescope-assisted photo voltaic inspection could cause considerably greater retinal temperature increases and photocoagulation injuries. Months later, there could additionally be foveal distortion, lamellar defects, pigment mottling, a macular gap or no obvious damage. The worst injuries occur with extended statement and good fixation, as when the solar disk is foveated through a defective optical filter. Operating microscope maculopathy charges have declined with improved, faster cataract surgery strategies, but injuries can nonetheless happen briefly procedures. The size, location, and severity of working microscope lesions determine their visible results. The endoilluminator lesion within the temporal macula of this 68-year-old male is accompanied by cystoid macular edema after epiretinal membrane surgery. The term foveomacular retinitis was originally used to describe foveal abnormalities resembling photo voltaic retinopathy. These situations include whiplash and blunt ocular injuries,129�131 although similar findings have been reported in folks with no prior historical past of photic or mechanical trauma. Increased chorioretinal pigmentation increases chorioretinal temperature elevations from photo voltaic remark, perhaps increasing the risk or extent of photic injury.