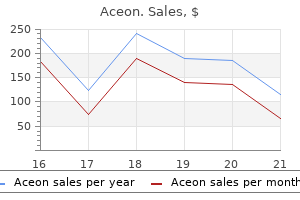
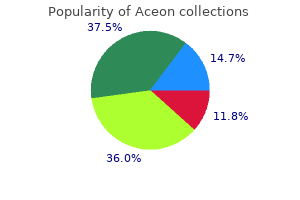
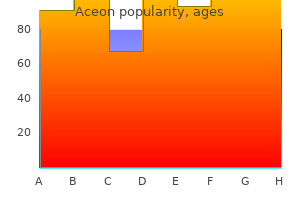
Aceon
Aceon dosages: 8 mg, 4 mg, 2 mg
Aceon packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Aceon 2 mg purchase fast delivery
An inferior meatal antrostomy for access to the sinus may be useful relying on the form of the sinus heart attack discount aceon 2 mg online. This antrostomy should be kept small 2258 and resection of the top of the inferior turbinate should be minimized heart attack pain in arm aceon 4 mg purchase free shipping. In these sufferers, instrumentation of the ground of the sinus will frequently determine areas of loculated secretions. This "mega-antrostomy" is also a approach to handle recirculation between middle and inferior meatal antrostomies. The revision ethmoid cavity is often tough to navigate because of altered landmarks, and image steerage is important. Exploration of this scar revealed debris trapped in the scar bed (bottom proper image). Therefore, one of the central goals of revision ethmoid surgical procedure, as in major surgery, is to prevent the development of osteitis. Meticulous mucosal preservation with elimination of partitions with slicing instruments will minimize this drawback. The aim is a single ethmoid cavity lined with normal mucosa so all partitions should be removed flush to the lamina papyracea and skull base if attainable. It is frequent to find small loculations of mucopus trapped behind these partitions. Preservation of the residual center turbinate is important to maintain 2260 landmarks and prevent lateralization and iatrogenic frontal recess illness. The retained uncinate resulted in persistent obstruction of the natural ostium of the maxillary sinus and continued persistent maxillary sinusitis. To maximize middle-meatal visualization and decrease ethmoid inflammation, any residual concha bullosa must be addressed. Pneumatization could not contain the pinnacle of the turbinate and will involve only the vertical lamella. Image steering is also useful, as a concha bullosa that was missed on the initial procedure can be challenging to find. One potential consequence of revision ethmoid surgical procedure is a destabilized center turbinate. The destabilized turbinate could make intraoperative middle meatus entry troublesome and it could possibly scar laterally making postoperative access a problem. The floor of the maxillary sinus is clearly seen and simply instrumented if necessary. The destabilized turbinate may make intraoperative middle meatus entry troublesome, and it might possibly scar laterally making postoperative access a problem. In revision ethmoid surgery, the skull base must be recognized early, and the lateral cavity must be examined for undissected cells. These lateral cells are sometimes the outcome of a retained uncinate that pushed preliminary dissection medially. The microdebrider has revolutionized sinus surgical procedure in this regard but should be used with caution as it can additionally strip mucosa and can violate each the lamina papyracea and the cranium base. As in main sinus surgical procedure, dissection should proceed from a posterior to anterior path after identification of the skull base. Care should be taken to not twist partitions as they might be extra sturdy than the cranium base. In the revision case, the center turbinate may be absent, and medial skull base dissection must proceed carefully to prevent inadvertent harm to the lateral lamella of the cribriform. When the limits of the 0� endoscope and/or the boundaries of 45� chopping instruments have been exhausted, an angled endoscope ought to then be used. Anterior ethmoid dissection ought to then proceed and shall be mentioned in the part on frontal sinus surgery. The surgical causes for sphenoidotomy failure can broadly be categorized into 2 teams. In the primary, the sphenoid was not entered (intentionally or unintentionally); whereas in the second, it was entered, but it was closed by secondary scarring. In other instances, mucosal inflammatory illness and polyp can recur in a correctly opened sinus with a patent sphenoidotomy. The revision sphenoidotomy, as is all revision sinus surgery, is usually sophisticated by altered anatomy. The pure ostium of the sphenoid sinus all the time lies medial to the superior turbinate and is reliably recognized in this place in primary sphenoidotomy. Additionally, the natural ostium could additionally be scarred and osteitic and will not be simply penetrable. In truth, the face of the sphenoid may be thicker than the again wall of the sphenoid, making vigorous penetration of the sphenoid face inadvisable. Magnetic resonance imaging in these circumstances will help identify the contents of the sphenoid and will decide the placement of the carotid artery, pituitary, optic nerve, and dura. The 2 principal endoscopic approaches to the sphenoid are transnasal (medial to the center turbinate) and transethmoid. Additionally, in the setting of a failed transnasal sphenoidotomy, the transethmoid approach ought to be tried. In the transnasal approach, the middle turbinate is gently lateralized and the superior turbinate is identified. The pure ostium of the sphenoid sinus is 2263 recognized medial to the superior turbinate and is enlarged with a J-curette, sphenoid mushroom punch, and/at Kerrison rongeur. The inferior side of the superior turbinate is usually trimmed to allow for added lateral enlargement. In this approach, lateral dissection is limited by the middle turbinate which may end in a smaller than sufficient sphenoidotomy. Additionally, if work ought to be carried out on the ethmoid or maxillary sinuses, the middle turbinate is at risk for changing into flail as work is finished both medial and lateral to the turbinate. As said previously, the flail turbinate can scar laterally, prevent postoperative entry to the center meatus and create iatrogenic frontal recess disease. Furthermore, the postoperative care of the transnasal sphenoidotomy is tough due to discomfort from instrumentation medial to the center turbinate, adjacent to the nasal septum. One of the biggest reasons for failure of main transethmoid sphenoid surgery is difficultly identifying the sphenoid or misidentifying an Onodi cell as the sphenoid sinus. This is much more difficult in revision circumstances, when the anterior edge of the superior turbinate could also be difficult to determine. In these cases, critical review of the radiographic relationships among the superior turbinate remnant, Onodi cell, if current, and the placement of the particular sphenoid sinus is paramount. Assuming the superior turbinate remains to be present, it may be preserved or the inferior facet of it can be resected. This could be accomplished with a straight probe or a J-curette and may be enlarged with a round punch or Kerrison-type forceps.
Aceon 4 mg generic mastercard
These nonactivated cells with IgM sure to their floor are known as virgin B-cells prehypertension causes aceon 4 mg cheap on-line. The IgM and the IgD receptors on anyone individual virgin B-cell confer the identical antigen specificity blood pressure 700 8 mg aceon order visa. Once a virgin B-cell binds antigen in its Fab region, it both becomes activated or turns into a memory B-cell. If the cell becomes activated, it secretes IgM molecules with the same receptor specificity as the unique membrane-bound IgM receptor. The binding of antigen by pentameric, secreted IgM causes the Fc area to bind and activate complement proteins, which in flip can unleash a cytotoxic biochemical attack on the surface of an invading microorganism. While the precise function of IgD is obscure, latest studies recommend that IgD enhances mucosal immunity by "arming" basophils as well as binding to the virulent components of bacteria and viruses in the upper respiratory tract. IgG antibodies are the first antibodies produced in the course of the secondary immune response. IgG antibodies are the one class of antibody that may traverse the placenta; additionally, IgG molecules are secreted in breast milk and absorbed within the neonatal gastrointestinal tract. This macromolecule binds to a particular Fcreceptor on the basal floor of epithelial cells. The entire IgA dimer/Fc-receptor advanced is engulfed right into a vesicle and transported across the cell cytoplam. The binding of antigen to this complicated triggers the mast cell or 1781 basophil to launch quite so much of preformed, biologically active amines. The most necessary of those amines is histamine, which causes vasodilation, increased vascular permeability, and bronchoconstriction. In addition, mast cells can activate a specialized sort of white blood cells known as eosinophils. Eosinophils are important for the immunologic protection towards parasites together with IgE antibodies. Antibody Diversity How does the body generate a seemingly limitless variety of totally different antibodies Scrutiny of amino acid sequences of various antibodies has led to the discovery that antibody diversity is achieved by way of multiple mechanisms involving the hypervariable areas within every mild and heavy chain. Heavy chains, and have one variable and three constant domains; whereas, and heavy chains have one variable and 4 fixed domains. The variable section of the sunshine chain and the variable section of the heavy chain collectively form the antigen-binding website or Fab area of the antibody molecule. The human physique makes roughly 1015 completely different antibody molecules with out previous immune stimulation, this is called preimmune antibody 1782 repertoire. The human genome incorporates less than 105 genes, but capable of synthesizing greater than 1015 antibodies. This paradox lends itself to the question: how can the human body make extra antibodies than the genes it has Each type of antibody chains, particularly, mild chain, mild chain and heavy chain, has its own pool of gene segments. While the constant area of both mild and heavy chains is encoded by a single gene phase, the variable areas differ. Two separate gene segments, variable (V) and becoming a member of (J) encode for the variable region of the light chain, whereas, the heavy chain variable area is encoded by a mixture of variable (V), range (D) and joining (J) gene segments. For instance, 200 (40 � 5) different V regions of light chain can be formed by combining any of the 40 V-gene segments with any of the 5 J-gene segments. Likewise, over 8200 (51 � 27 � 6) V regions of heavy chain may be resulted from 51 V-gene segments, 27 Dgene segments and six J-gene segments. If any gentle chain can mix with any heavy chain, more than 106 completely different antibody combos can then be produced. The complement system enhances the antibody response and protects the body towards bacterial infections. Individuals with deficiencies within the production of complement proteins have increased susceptibility to bacterial infections, as do individuals with antibody deficiencies. Activation of complement by varied immune mediators begins when an antigen is encountered through the main immune response. Once complement proteins are activated, they in turn activate other proteins downstream, which finally work in concert to kill the invading microorganism. The classical pathway is activated by IgG or IgM antibodies certain to the floor of an invading microorganism. Once the primary enzyme within the sequence is activated, it generates a serine protease that cleaves and activates the next component in the pathway. The cascade also amplifies the response such that activation of some early complement proteins triggers a larger subsequent response. Furthermore, cleavage of the complement proenzyme reveals an lively enzyme and a small membrane binding website. This causes the activated complement proteins to adhere to the membrane of the invading microorganism, quite than diffusing into the bloodstream. The classical, various and lectin pathways all converge at the cleavage of C3 into C3a and C3b. While C3b and C5b serve as major players of the complement cascade, C3a and C5a act as diffusible, proinflammatory anaphylatoxins that recruit white blood cells (such as neutrophils and monocytes). The potential harmful properties of complement proteins require subtle mechanisms to stop destruction of normal tissues. First of all, complement proteins are secreted in inactive forms and are solely activated within the presence of an antigen. Thirdly, specific inhibitors exist in the blood to deactivate quickly complement proteins to forestall widespread destruction of regular tissue. These methods act together to control the efficiency and motion of the complement system. T-cells form the opposite main class of lymphocytes and are liable for the mobile responses. While B-cells can secrete antibodies that act at nice distances away from the unique B-cell, T-cells are depending on the interaction with the goal cells within a short range. They work together with the target cells in considered one of two fashions: both by killing the target cell or utilizing the goal cell in a signaling cascade to recruit other cells and enhance the immune response. Furthermore, these peptide sequences must be offered to the T-cell by particular molecules on the surface of the target cell. The T-cell receptor recognizes the peptide sequence certain to the special molecule advanced and subsequently initiates downstream responses. These mechanisms permit T cells to respond successfully in opposition to intracellular microorganisms, corresponding to viruses, and towards phagocytic cells which have engulfed overseas extracellular peptides. Other subtypes of helper T-cells have been named after their production of 1 main cytokine, these embrace, Th5, Th6, Th7, Th9, Th17 and Th22 cells.
Cheap aceon 2 mg mastercard
It is important for many patients to know the true diploma of olfactory loss arteriosclerotic cardiovascular disease aceon 2 mg cheap without a prescription, provided that prognosis relates to heart attack jaw pain 2 mg aceon visa the magnitude of the loss. Mechanical obstruction secondary to distorted intranasal architecture or intranasal tumors can typically be addressed surgically. However, inflammatory causes of sinonasal disease usually tend to be treated medically or in combination with surgery. Quantitative olfactory testing is advised before and after remedy to guarantee an accurate assessment of the intervention and to assess long-term outcomes. Examples of therapies which have restored olfactory perform in some sufferers embrace allergy administration, topical and systemic corticosteroid therapies, antibiotic remedy, and functional endoscopic sinus surgical procedure. A temporary course of systemic corticosteroid remedy can be helpful in distinguishing between conductive and sensorineural olfactory loss, as sufferers with the previous will usually reply positively to the treatment. Topical nasal corticosteroids could additionally be ineffectual in altering odor dysfunction because the corticosteroid fails to penetrate the upper recesses of the nostril. Administering nasal drops or sprays in the head-down Moffett position can typically improve efficacy. When spontaneous recovery happens in head trauma patients whose loss reflects damage to the olfactory receptor cell axons, it usually does so inside three or 4 months of the injury. Patients who stop smoking tobacco usually have 1734 dose-related enchancment in olfactory perform and taste sensation over time,a hundred and ten although tobacco smoking by itself hardly ever causes complete loss of the sense of smell. Some central olfactory neural impairments, for instance, tumors throughout the medial temporal lobe or tumors that impinge upon the olfactory bulbs or tracts, can, in some people, be resected in a fashion that enables for no much less than some restoration of olfactory perform. Some sufferers with extraordinarily debilitating continual dysosmia (usually of a quantity of years duration and infrequently unilateral), in whom weight reduction is marked or daily functioning is markedly impaired, are amenable to surgical intervention, for example, ablation of regions of the olfactory neuroepithelium or olfactory bulb elimination. Of the surgical approaches, intranasal ablation or stripping of tissue from the olfactory neuroepithelium on the effected facet is more conservative and less invasive than elimination of the olfactory bulb and/or tract through a craniotomy. When olfactory disturbances are attributed to a particular medication, discontinuance, dose changes, or substitution of other modes of therapy can be effective, although fast reversal of the issue hardly ever occurs. Although it has been instructed that alpha-lipoic acid,113�114 as nicely as working towards smelling odorants,a hundred and fifteen may assist in bettering odor operate, lack of masking (blinding) and acceptable controls limits the value of such research. To date, no double masked research has been carried out to demonstrate the efficacy of such therapies. Because of this truth, complete lack of style function is uncommon from peripheral insults or trauma (since all nerves would have to be involved), and is extra likely due to systemic or central causes. The sensation of "chocolate," however, is dependent upon retronasal stimulation of the olfactory receptors. The goblet-shaped style buds are distributed over the dorsal floor of the tongue, the lateral margin of the tongue, the base of the tongue, the soft palate, pharynx, larynx, epiglottis, uvula and the primary third of the esophagus. Of the four kinds of papillae � fungiform, foliate, circumvallate, and filiform � solely the primary three harbor style buds. Taste buds are regularly bathed in secretions from the salivary glands and nearby interlingual glands. The saliva accommodates not only such proteins as amylase (which initiates starch breakdown of foodstuffs), but development elements important for wound therapeutic and the maintenance of taste buds. Indeed, removal of the submandibular and sublingual salivary glands results in taste bud loss that could be prevented by supplying epidermal development issue in the ingesting water. The opening to the bud is termed the style pore, and the excavation below the pore is termed the style pit. Several types of cells are found inside the taste bud, together with cells that project microvilli into the style pit and basal cells from which other cell varieties come up. Apically, these cells end with various sorts of microvilli within the style pit and will attain the taste pore. Nerve fibers throughout the short dermal papilla are barely myelinated, and within the style bud they kind an umyelinated plexus. Note the basal lamina between dermis (which incorporates a capillary) 1737 and the epithelium. After coming into the taste pore, the tastant initiates the transduction process through considered one of two mechanisms: A) activating receptors coupled to G-proteins that, in turn, activate second messenger systems (a process that in all probability happens with sweet and bitter tasting stimuli); and B) directly gating apical ion channels on the microvillae inside the style bud pit (a process that most likely happens with bitter and salty tasting stimuli). Although more than 2,000 genes have been associated with primate style buds,121 candidate taste receptor genes number less than 50. Sweet tastes seem to depend mainly upon the T1R3 receptor, when paired with the T1R2 receptor, though T1R3 knockout mice nonetheless have the power to detect some sugars. Many bitter tasting substances, including caffeine and quinine, bind to numerous completely different receptors. Salty tastes are largely mediated by Type I cells, which � like neuroglia � serve secretory and phagocytotic capabilities, including transmitter redistribution and ion clearance. For example, miraculin, a gylcoprotein from the berry of the African shrub Syncepalum dilcificum, quickly modifications most sour-like sensations to 1738 sweet sensations. Gymnemic acid, an extract from the leaves of the Indian plant Gymnema sylvestre, can mitigate the perception of candy sensation (and the corresponding electro-physiologic activity) with out significantly altering the perception of the opposite taste qualities. An understanding of this truth can be become necessary when scientific syndromes that involve style dysfunction are thought-about. The taste buds within the region of the nasopharynx are provided by the pharyngeal department of this nerve. The nerve cell our bodies of these gustatory afferent fibers are found throughout the petrosal ganglion immediately outside the jugular foramen, where the fibers finally cross to enter the cranium. Afferent fibers from the superior laryngeal nerve project by way of their cell our bodies within the inferior nodose ganglion. Like the glossopharyngeal nerve, the vagus penetrates the cranium via the jugular foramen. These regions include multimodal neurons responsive to touch and temperature, in addition to taste. There is some evidence, nonetheless, that handedness could need to be managed in such studies. Total ageusia is uncommon and, when current, is usually produced by central, for example, ischemic, medication occasions, since regeneration of style buds can happen and peripheral injury must contain multiple pathways to induce taste loss. Thus, whereas 433 of 585 sufferers (74%) studied at the University of Pennsylvania Smell and Taste Center who exhibited olfactory loss complained of each odor and style disturbance, less than 4% had verifiable whole-mouth gustatory dysfunction, and even that was restricted. For example, in a single study, sensitivity to three concentrations of NaCl was measured on the tongue tip and three cm posterior to the tongue tip in 12 younger (20 to 29 years of age) and 12 aged (70 to seventy nine years of age) topics. On average, the younger topics had been more delicate to NaCl on the tongue tip than on the extra posterior stimulation web site and exhibited, at both tongue loci, improve in detection performance as the stimulus concentration elevated. The elderly topics, who would be anticipated to exhibit, at worse, moderate deficits on 1742 whole-mouth testing, carried out at chance levels. In truth, most sufferers can sustain loss of taste sensation on half of the anterior a part of the tongue following unilateral sectioning of the chorda tympani nerve in middle-ear surgery with out noticing the problem. Such ignorance stems, in part, from the redundancy of the a quantity of taste nerves, in addition to compensatory mechanisms.
Discount 2 mg aceon with mastercard
The mylohyoid muscle and anterior stomach of digastric muscles is supplied by the mandibular division of the trigeminal nerve blood pressure watches 4 mg aceon buy mastercard. Motor innervation of stylohyoid muscles and posterior stomach of digastric muscular tissues is supplied by the facial nerve heart attack 86 years old order 2 mg aceon visa. The 2914 sternocleidomastoid and trapezius muscular tissues are innervated by the spinal accessory nerves. The laryngeal department consists of the superior laryngeal nerve and the recurrent laryngeal nerve. The superior laryngeal nerve has each an external and inner branch; the external department supplies motor operate to the cricothyroid muscle, and the interior branch offers sensation to the supraglottic region. The recurrent laryngeal nerve offers motor innervation to all different muscles of the larynx, in addition to sensation to the vocal folds and inferiorly into the subglottis. The pharyngeal branches of the vagus nerve present motor innervation to the muscular tissues of the pharynx and palate, besides the stylopharygeus muscle which receives its innervation from the glossopharyngeal nerve, and the tensor veli palatini muscle which is supplied by the mandibular branch of the trigeminal nerve. Cervical Vasculature and Lymphatics the arterial system of the top and neck is separated into contributions from the subclavian artery and the carotid artery. The thyrocervical trunk branches into the inferior thyroid artery, the transverse cervical artery, and the suprascapular artery. Its principal cervical branches include the superior thyroid artery, ascending pharyngeal artery, posterior auricular artery, occipital artery, lingual artery, facial artery, superficial temporal artery and inside maxillary artery. The venous drainage from the pinnacle and neck is primarily through the external and internal jugular veins. The posterior auricular vein, occipital vein, and posterior retromandibular vein turn into the external jugular vein, while the anterior retromandibular vein, facial vein, lingual vein, superior and middle thyroid veins drain into the inner jugular vein. The lymphatic drainage of the top and neck is primarily to the deep cervical lymph nodes from regional superficial lymph node basins. The regional basins 2915 are the occipital, retroauricular, parotid, submandibular and retropharyngeal nodes. These drain to the deep cervical lymph nodes, which in the end drain into the thoracic duct or the best lymphatic duct, each of which are positioned throughout the root of the neck the place the internal jugular and subclavian veins meet. The main baseline saliva contribution is from the submandibular glands by stimulation from the postganglionic parasympathetic fibers from the submandibular ganglion. The parotid gland is the primary contributor in stimulated salivary secretion via the postganglionic parasympathetic fibers of the auriculotemporal nerve from the otic ganglion. Salivary circulate could additionally be altered by age, hormones, systemic diseases, food regimen, hydration and drugs. The saliva of the parotid glands is more serous whereas the saliva of the submandibular glands is more mucinous. The chemical composition of the saliva is a variable mixture of amylase, statherin, histatins, mucins, lysozymes, lactoferrin, peroxidases, secretory IgA, proline rich proteins, thiocyanites, salts, gases, and other organic substances. The secretory IgA, lactoferrin, lysozyme, and peroxidases have antibacterial effects. Statherins help within the maintenance of dentition and shield tooth from detrimental effects of the human food regimen. Taste buds are additionally found in the epithelium of the soft palate, pharynx, larynx, epiglottis, and esophagus. The taste bud is concerned within the perception of chemical stimuli and in style transduction. The taste pore within the central opening on the epithelial floor of the taste bud is where food molecules are offered to the 2916 receptor cell. The two major lessons of receptors are the seven-transmembrane G-protein coupled receptor and ion channels. Bitter, sweet and umami is mediated by way of stimulation of G-protein coupled receptors. The fungiform, circumvallate and foliate papillae are referred to as gustatory papillae in that in addition they include sense organs which might be capable of understand style. The eight to 10 circumvallate papillae are in an inverted V-shape and separate the anterior two-thirds of tongue from the posterior one third. Further info on the sense of style is in Chapter 38 entitled Olfaction and Gustation. Speech and Swallowing Speech is necessary for communication and is the result of coordinated exercise of the respiratory tract as well as other associated constructions. The modification of voice and articulation occurs via the relaxation of the upper aerodigestive tract including the pharynx, palate, mandible, tongue, teeth and lips and the higher respiratory tract together with the nasopharynx, nostril and paranasal sinuses. Swallowing is conveniently described in four phases: the preparatory phase, the oral part, the pharyngeal section, and finally the esophageal part. In the oral part, the bolus of meals is moved from the oral cavity to the oropharynx. The pharyngeal section is composed of multiple simultaneous actions beginning with velopharyngeal closure, laryngeal elevation, contraction of the pharyngeal constrictors, and cricopharyngeal relaxationIncluded on this phase is the speedy superior and anterior motion of the hyoid bone with laryngeal elevation and closure. The esophageal part of swallowing starts as quickly as the bolus passes by way of the cricopharyngeus. Several pathologic conditions can lead to alterations in each speech and swallowing. Some of these, similar to ankyloglossia, velopharyngeal insufficiency and sialorrhea, are focal conditions which may be handled with surgery or speech remedy. Ankyloglossia, generally referred to as tongue tie, is because of a short lingual frenulum. The severity of ankyloglossia ranges from mild to full with the tongue being tethered to the ground of the mouth. This situation affects the mobility of the tongue and may impair feeding and sucking in infants in addition to create issues with articulation later in life. Mild ankyloglossia can often be managed with oral remedy whereas extra severe ankyloglossia is treated by frenulectomy. Velopharyngeal insufficiency is brought on by insufficient velopharyngeal closure which permits air or meals substances to escape via the nostril. Mild velopharyngeal insufficiency can likewise be treated nonsurgically with speech remedy and prosthetic devices. Surgical therapies corresponding to coronal and sphincter pharyngoplasty, pharyngeal flap, and posterior pharyngeal wall augmentation may show essential. Sialorrhea could replicate extreme manufacturing of saliva due to medications or an infection but extra generally reflects decreased saliva clearance secondary to open mouth respiratory or impaired swallowing. The management of sialorrhea contains treating an underlying an infection, avoiding predisposing medicines, or lowering saliva manufacturing by botox injections or surgery corresponding to ductal ligations and gland excisions. Systemic circumstances corresponding to neuromuscular issues also can impair speech and swallowing. Polymyositis affects muscles within the center of the body and may progress to contain swallowing. Amyotropic lateral sclerosis causes progressive muscle losing and eventual paralysis.

Aceon 4 mg buy overnight delivery
When the remedy setup has been finalized the therapy protocol is exported to Leksell Gamma Knife arrhythmia practice test generic 8 mg aceon with visa. In addition hypertension kidney group 08755 4 mg aceon purchase free shipping, a protecting design limits the transfer of a therapy plan to the Leksell Gamma Knife to one affected person at a time. However, with the mannequin B the remedy group enters the therapy room after every shot is delivered and manually adjusts the X, Y, and Z coordinates, as properly as the gamma angle, ie, the pitch of the top, if essential. While changing into of historic interest, for the model B and model C models, the group needed to change the collimator helmet manually 1643 when needed, as dictated by the therapy plan. In the Perfexion unit, all features of the treatment supply are automated with no need to change the collimator helmet. The cobalt sources transfer linearly to the suitable collimator sizes within each sector of the machine along and with automated motion of sofa. This allows faster therapy delivery in comparison with previous-generation Gamma Knife models. In this instance, 13 Gy delivered to the 50% isodose line was prescribed (dark blue line). The most dose (26 Gy) is delivered to the center of the tumor volume (asterisk). The outer most line (green line) represents the dose supply distribution of four Gy of radiation. A gradient color scale has been used to symbolize visually the relative quantity of radiation delivered with dark orange illustrating the utmost radiation delivered and blue illustrating the least radiation delivered. These knowledge enable an understanding of how much of every volume receives a specific dose of radiation. In this affected person, particular person isodose coordinates had been changed until the cochlear volume was measured to have one hundred pc receiving lower than 4 Gy to reduce radiation-induced listening to loss. Before repositioning, the sofa will move out a short distance to convey the patient out of treatment focus. Additional runs are performed after manually altering the collimator helmet for the model 4C. For the Perfexion the collimator helmet allows automated changes in measurement according to eight sectors, plus automated management of the coordinates and treatment times of every isodose delivered. The anterior fixation websites are dressed with antibiotic ointment and adhesive bandages. Often pressure must be held to management bleeding and occasionally a staple may have to be used on the posterior sites. Typically patients will expertise a transient headache after elimination of the frame and some develop nausea and emesis. Patients are observed for a number of hours posttreatment and discharged house with pain 1645 medication and follow-up appointments. Tumor control and facial nerve motor preservation occurs with virtually all vestibular schwannoma sufferers treated with present Gamma Knife protocols. Areas of continued focused investigation embody the results of radiosurgery on hearing and balance, and methods of improving outcomes. There are two well-recognized listening to classification systems for accessing outcomes after intervention in vestibular schwannoma management: the American Academy of Otolaryngology � Head and Neck Surgery hearing classification system29 Table 36-1); and the Gardner-Robertson classification system30 Table 36-2). Lunsford and colleagues summarized their expertise with 829 vestibular schwannomas handled between 1987 and 2002. They reported tumor control in 97% of patients at 10 years, and facial nerve (motor) dysfunction in < 1% of patients. Trigeminal nerve symptoms occurred in < 3% of patients and sometimes occurred with massive tumors reaching the level of the trigeminal nerve. The reporting of hearing preservation has limited representation in the entire 829 sufferers. Hearing-outcomes knowledge were presented in only 267 sufferers, and "five-year actuarial charges of hearing-level preservation and speech preservation" have been reported in 103 patients. They additionally acknowledged that "for sufferers with intracanalicular tumors, hearing preservation charges in these treated with 12. They additionally reported a "preservation of testable speech discrimination capability" in ninety one � 2. Based on our medical observations and people of other facilities, this image is way more complicated over time than is represented in these publications. Prasad and colleagues from the University of Virginia reported their series of 200 patients with vestibular schwannomas treated with Gamma Knife surgical procedure over a 10-year interval in 2000. They reported no listening to prior to Gamma Knife surgical procedure in one hundred and five patients, together with fifty three of 96 primary-treatment and fifty two of fifty seven secondary-treatment patients. Despite these limitations, they found that, apart from one affected person, no change in hearing was observed in the first two years after Gamma Knife surgical procedure. Their information additionally showed that the best change in Gardner-Robertson grade occurred between years two and 4 after Gamma Knife surgery; nevertheless, with out understanding the assessment intervals, the precise onsets of the listening to losses are unknown. Before Gamma Knife surgery, interim after Gamma Knife surgical procedure, and last after Gamma Knife knowledge were reported. Similar to our expertise, they discovered that in sixteen sufferers the 1648 listening to deteriorated > 20 dB three to six months after Gamma Knife surgical procedure and that this listening to loss continued for twenty-four months. The only prognostic factor for hearing deterioration that they identified was the maximum dose to the cochlear nucleus. Lasak and coworkers reported 33 patients with vestibular schwannoma who have been handled with Gamma Knife surgery and who had audiometric information pre- and post-treatment. The median audiometric follow-up was 24 months, with a variety of six to 51 months (mean = 24. Fifteen sufferers received lower than the median cochlear dose, and 18 received greater than or equal to the median cochlear dose. This early and vital drop in auditory perform is in maintaining with those observed by Paek et al. They found that there were three predictors of good listening to outcomes: 1) sufferers who had an initial symptom apart from listening to loss (91. Massager et al reported 82 sufferers with vestibular schwannomas handled with Gamma Knife surgery. All patients acquired a marginal dose of 12 Gy and a radiologic and audiologic 1649 follow-up of no less than one 12 months. The dosimetric knowledge of the quantity of the cochlea have been retrospectively analyzed and have been correlated with the auditory end result of sufferers. The cochlea received significantly larger radiation doses in patients with worsening of hearing after Gamma Knife surgical procedure. In addition, a highly vital association between the dose of radiation delivered to the cochlea and the inner auditory canal and the hearing loss was found.
Aceon 4 mg generic online
Symptomatic therapy should be individualized to present enough hypertension knee buy aceon 4 mg line, prompt reduction with minimal danger and unwanted effects blood pressure zones aceon 2 mg cheap without prescription. An method to utilizing stratified care has proven profitable where the energy of the prescription is reflective of the severity of the headache. Factors influencing choice of drugs ought to embody the frequency that drugs might be required, contraindications, route of administration (based on velocity of onset of head ache and length of the headache), prior medicine successes and failures, or the necessity for breakthrough headache therapy. Antiemetics such as metoclopramide must be given first to avoid worsening or triggering nausea; this class of medication facilitates the absorption of the antimigraine medication by reversing gastric stasis. Triptan remedy can be used early in the center of remedy for sufferers with substantial incapacity consistent with a stratified strategy to care. Table 51-4 Triggers for Migraine14 Ingested food or drink Aged cheese Alcohol Artificial sweeteners Caffeine Chocolate Fermented foods Nitrites Red wine Odor exposure Cigarette smoke Cleaning brokers Exhaust Paints Perfumes Hormonal variations Hormonal alternative therapy Menses Oral contraceptives Pregnancy Irregular schedule Exercise Meals Sleep Stress or anger Flashing lights Reproduced from reference 14, by permission of Blackwell Science, Inc. Finally, for difficult to treat sufferers, referral to a headache heart or neurologist is acceptable. For kids, Annequin and associates reviewed using various agents and found good effectiveness for each acetaminophen and ibuprofen. Prophylactic remedy is indicated when the frequency of episodes is larger than five days per thirty days. Dosages ought to be titrated within beneficial ranges utilizing the principle of beginning at a low dose and slowly titrating to a therapeutic dose to reduce side effects. Therapeutic trials of any agent ought to last a minimal of 4 to eight weeks on circumstance that therapeutic effects are sometimes delayed. This class of headaches is by far the most typical, afflicting approximately 80% of the grownup inhabitants. Tension-type headache is more more probably to occur in women, and normally a family historical past of headaches is current. The headaches are characteristically bilateral, with a tightening or band-like sensation within the frontotemporal region around the head, and spreading to the occipital area or trapezius muscles. The onset is gradual, whereas the standard is dull, non-throbbing, and constant, sometimes lasting for weeks. By definition, the 2187 headache lasts from 30 minutes to seven days and has two of the next characteristics: a tightening high quality, mild to average intensity, bilateral location, and never aggravated by routine bodily activity (exercise may typically enhance pain). The cephalalgia is triggered or exacerbated by stress or anxiousness in most sufferers. Some proof has discounted the concept persistent muscle contraction is the purpose for the ache. Some debate nonetheless exists as to whether all persistent day by day complications are tension-type. This could symbolize an evolution of the headache course of which is commonly related to overuse of rescue medicines. According to Silberstein and Lipton, persistent daily headache must be divided into each tension-type and migrainous sort, in addition to other entities. Any psychiatric comorbid conditions should be recognized and evaluated appropriately as a risk factor for remedy failure. Non-pharmacologic cures embrace: reassurance, muscle rest, simple muscle workouts, stress administration, biofeedback, and physical remedy with thermal modulation, ultrasonography, or electirical stimulation. They are unilateral, excruciating, and situated across the eyes/temples or in the maxilla. The cephalalgia is related to unilateral lacrimation, rhinorrhea/nasal stuffiness, and injected conjunctivae. A cluster interval is the phase of time during which assaults are probably to occur several times per day for several weeks. The cluster period ends with remission of attacks and begin of a headache-free period; therefore the assaults occur in "clusters. Rapid eye movement sleep as a trigger causes sleep deprivation which, in conjunction with the headache, may lead to despair. Circadian hormonal fluctuation suggests a hypothalamic dysfunction (and this area is metabolically energetic on positron emission scanning throughout a cluster attack), whereas excitation of a nerve plexus within the carotid sheath and adventitia might enhance trigeminal discharge charges resulting in facial ache. Chronic paroxysmal hemicrania 2190 (Sjaastad syndrome) is a variant with shorter, extra frequent assaults lasting two to forty five minutes), occurs more typically in girls, and is normally responsive to indomethacin. It may be precipitated by contact to the nose/periorbital area, with chewing, or ingestion of citrus fruits. Along with providing reassurance for the patient, episodes can be ended with inhalation of one hundred pc oxygen for 10 minutes, however there are obvious logistical challenges with utilizing oxygen. Sumatriptan is the best selfadministered medication for the symptomatic aid of the cluster assault. Other choices embrace intranasal imitrex 20 mg or zomitriptan, rizatriptan or eletriptan orally (several different triptans might take longer to work), though relief might take 30 or more minutes to occur with these oral preparations. At least three episodes of cephalalgia must be treated with anyone agent earlier than declaring it a failure and transferring to one other agent. Short-term or transitional prophylaxis can be utilized during a cluster period to suppress attacks, whereas maintenance prophylaxis is used earlier than and all through the period of the cluster period. In general, they want to be used early in the cluster period till the patient has been headache-free for no much less than two weeks after which adopted by a tapering interval. Maintenance prophylaxis could also be required when transitional prophylaxis and suppression therapy have been discontinued, turn out to be ineffective or in anticipation of onset of the cluster period. Newer approaches have used valproate, topiramate, pizotifen and phototherapy with brilliant gentle. Histamine desensitization could supply aid to patients with persistent cluster headaches refractory to therapy. Karst and colleagues in 201079 reported remissions in 4 chronic and one episodic cluster patients in an open, non-randomized case collection (patients had failed verapamil and various different prophylactic agents) with the usage of a modified type of lysergic acid (2-bromo-lysergic acid diethylamide) which has no hallucinogenic potential. Associated signs embrace altered degree of consciousness and sometimes nausea and vomiting, in addition to focal central nervous system changes. There is usually an antecedent history of head trauma, though the trauma may be temporally distant. Treatment usually involves a craniotomy for drainage, but spontaneous decision might occur over time. Head and/or neck trauma has been associated with the onset of acute or 2192 continual complications. It could be aggravated by routine bodily actions, and it may have related signs of a migraine headache, normally sensitivity to light and noise. The affected person also wants to be evaluated for psychiatric comorbidities or psychological modifications. All patients ought to endure repeat imaging, especially in instances of persistent headache or severe personality modifications.
Buy aceon 4 mg line
In addition hypertension signs and symptoms aceon 2 mg discount amex, any back-cut on the base of the flap to obtain lengthening or appropriate canine ears peripheral neuropathy purchase aceon 4 mg fast delivery, compromises the blood provide to the flap. To circumvent this problem, canine ears may be left in place and allowed to settle over time. Alternatively, cuts positioned on the base of the flap to improve rotation or to remove canine ears should be directed away from the pedicle and designed as a Z-plasty or Burow triangle, thus maintaining a wide pedicle base. Incisions are made by way of the anterior helical pores and skin and cartilage leaving the posterior auricular skin intact. A Burow triangle can be excised from the posterior auricular pores and skin to facilitate closure of the secondary defect. A circular defect is first transformed to a triangular defect by excising a Burow triangle. The defect was initially closed with a cut up thickness pores and skin graft and placement of two a hundred ml tissue expanders. After tissue enlargement, two broadly based rotation flaps had been designed to recruit tissue from either side of the defect. Transposition flaps are versatile in that they are often designed with borders which are removed from the defect thus allowing flexibility in placing incisions. Examples of transposition flaps generally utilized in head and neck reconstruction embrace the Limberg or rhombic flap, note flap, bilobed flap, interpolation flap, and hinge flap. The Limberg flap is an extremely versatile instance of a transposition flap used in closing rhombic-shaped defects. Four choices for putting the third limb of the flap can be chosen and drawn parallel to the edge of the defect. Thus for a given rhombic defect, four Limberg flaps can probably be raised depending on where the third limb is placed. The third limb is selected to recruit probably the most cellular skin that permits for one of the best camouflage without distortion of surrounding structures. The resulting secondary defect is then closed primarily by undermining and advancing the encompassing tissue. The direction of pressure should be located such that closure avoids distortion of defining buildings. Like the Limberg flap, the Dufourmentel flap is also a transposition flap designed to shut rhombic defects. The flap is designed by extending one line from the brief axis to a length equivalent to the facet lengths, similar to a traditional rhombic flap, and one other line is drawn by extending the aspect adjoining to the decrease angle to a similar length. It is, 2618 therefore, finest fitted to restore of defects of the lateral facial subunits: lateral cheek, mandible, and temple regions. As these areas are seen tangentially from direct facial presentation and are thus much less noticeable. The basic Z-plasty is basically two adjacent random triangular flaps that interchange place by being lifted into each others defect thereby lengthening and reorienting their frequent central limb. Z-plasties are used to lengthen tight, contracted scars or reorient tissue or scars right into a more fascinating location. In the basic Z-plasty, the adjacent triangles are equilateral triangles with 60� angles. A 30�, 45�, and 60� Z-plasty can theoretically lengthen a scar by 25%, 50%, and 75% respectively. The actual achieve in length relies on the elasticity of the encompassing tissues. Occasionally the best flap design requires that the two flap angles be of various sizes or angles. Other variants of the traditional Z-plasty are the double opposing Z-plasty used in cleft palate and epicanthal fold restore, and the a number of operating Z-plasty utilized in scar revisions. Another widespread transposition flap is the "notice flap," so referred to as because the design is reminiscent of a musical eighth note. To design the flap, a tangent is drawn from the edge of the circular defect parallel to a relaxed pores and skin rigidity line for a distance of 1. A second line equal in size to the first is drawn at 50� to 60� to the primary to create a triangular flap. The flap is then elevated with extensive undermining of the tissue surrounding the defect. Invariably a standing-cone deformity develops, the dimensions of which depends upon the arc of rotation. In its unique description, the two lobes of the bilobed flap have been at 90� angles so that the final transposition was over an 180� arc. Final arcs of transposition of 90� to 110� are extra optimal with less ensuing deformity. The bilobed flap is primarily utilized in closing defects of the decrease third of the nose but can be used in other regions of the face such as the infraorbital region. A drawback of the flap is that the resulting scar is 2619 unable to follow pores and skin tension strains in lots of situations. It can additionally be extra susceptible to pincushioning as a outcome of the curvilinear scars and the wide bed of scar that contract deep to the flap. Compared to the traditional Limberg design, the pedicle base is broader and the main angle is more obtuse. A needle is inserted at this pivot level and a suture is wrapped round a marking pen. Using this as a guide, the trail of rotation is drawn out starting from the edge of the defect. The first lobe of the flap equaling the scale of the defect can then be drawn adjoining to the defect. The second lobe is usually designed as a triangular flap to facilitate closure and may be made smaller than the secondary defect. The distal portion of the flap can be tailor-made to fill the depth of the primary defect, but the relaxation of the flap ought to be stored thick to optimize its vascularity. A Burow triangle centered on the pivot level is then excised at the base of the primary defect to facilitate transposition of the lobes. The interpolation flap is a random or axial flap designed and lifted into a close-by defect over or beneath an intervening bridge of normal skin. Common examples embody the melolabial flap, the paramedian-forehead flap, and Monk-eyelid flap. If the flap passes over an intervening tissue, a second-stage process is required for pedicle division. When the pedicle passes under a bridge of normal skin, a portion of the pedicle can be de-epithelialized to allow a one-stage process. The paramedian-forehead flap is the flap of selection for reconstructing extensive-nasal defects. It can be used for reconstructing complex-periorbital and medial-cheek defects. A detailed dialogue of the paramedian-forehead flap is provided in Chapter sixty three, "Nasal Reconstruction.

8 mg aceon best
The premorbid form and function of dental arteria princeps pollicis aceon 8 mg amex, skeletal 5 htp and hypertension order 8 mg aceon fast delivery, and delicate tissues should be reestablished as a lot as is feasible. Recent pictures and dental data, if obtainable, are most useful to establish the pre-traumatic appearance. If the initial injury involves pores and skin or mucosal lacerations, makes an attempt should be made to make the most of these lacerations when possible for the strategy to fracture repair. If no epithelial damage is present, approaches to fractures ought to attempt to maximize exposure, whereas minimizing scarring and danger to adjoining neural and vascular constructions. Often, these patients have suffered multiple injuries and could also be both unconscious or intubated. Information may be gleaned from pals or family members on the scene or the police or ambulance attendants. Physical examination features a careful inspection of dental occlusion, examination of the facial contour, and palpation of the facial bones. After fracture prognosis is completed, a systematic therapy plan is established. Surgical therapy of facial fractures includes enough publicity, meticulous discount, and secure fracture fixation. After exposing the facial fracture, meticulous discount must be performed and maintained until enough fixation of the fracture can be done. Fixation methods should permit for complete 2723 bone therapeutic with reconstitution in three dimensions: peak (superior-inferior), width (lateral-medial), and depth or projection (anterior-posterior). Repair of soft tissue injuries is usually as necessary as fracture therapy in the complete restoration of the patient with craniomaxillofacial injuries. This is very true within the periorbital region, where injuries similar to telecanthus, enophthalmos, and dysopsia often accompany the skeletal harm. Complete remedy of facial accidents requires consideration to these soft tissue accidents and the correct reattachment of sentimental tissue fascial layers after fracture restore. Table 65-1Principles of Diagnosis and Initial Treatment of Facial Fractures Establishment and securing airway Control of bleeding Detailed history Careful physical examination the basic principles of prognosis and initial remedy of patients with facial fractures are listed in Table 65-1. Understanding dental occlusion is a vital element within the management of facial fractures. Dental occlusion is the connection of the maxillary to the mandibular teeth with regard to their slicing and grinding surfaces. This relationship largely is dependent upon the relative place of the teeth and their angulation to one another. In the Angle system, the reference level is the connection of the primary maxillary molar tooth to the mandibular molar tooth beneath it. The cusps adjacent to the tongue are called lingual and those adjacent to the cheek, 2724 buccal. In this kind, the mesial buccal cusp of the first maxillary molar fits in the groove on the lateral or buccal floor of the primary mandibular molar tooth. The buccal cusps of the maxillary enamel overlap the buccal surfaces of the mandibular molars. The setback chin often prevents the upper lip from fully covering the upper incisor tooth. This lack of lip protection, called lip 2726 procumbency, can render the incisors more vulnerable to injury. The overbite leads to the higher incisors biting into the gingival lingual sulcus beneath. The malocclusion is often so extreme the patient has an extremely difficult time chewing stable meals. This open chew deformity produces a marked useful disturbance and is extremely unpleasant. In addition to aberrations within the anteroposterior relationship of the dentition are deformities involving malposition within the medial and lateral path, in addition to abnormalities involving a lateral tilt of the occlusal airplane. If each arches are symmetric, the maxillary molars of the opposing aspect shall be put right into a extra buccal relationship with the opposing mandibular enamel, thereby creating a buccal crossbite on this particular side. For instance, a narrow maxillary arch coupled with a reasonably regular mandibular arch, as seen in hemimandibular hypoplasia, typically produces a buccal crossbite on one aspect and normal occlusion on the opposite. The coronoid course of is the anterior- superior extension of the mandibular ramus projecting above the mandibular notch into the infratemporal fossa. The angle is a non-tooth-bearing portion of the mandible between the ramus and the physique. The parasymphyseal area consists of the anterior arch of the mandible and is bounded by the two psychological foramina. The alveolar ridge or course of consists of thin cortical bone (lamina dura) that encompasses the tooth and atrophies when the teeth are gone. While traversing this canal, it gives off sensory innervation to the dentition and gingival. The terminal portion of the inferior alveolar nerve is the mental nerve which exits the physique of the mandible on the labial floor just below the second premolar tooth. It is important to keep in thoughts that the nerve travels about 2 to three mm anteriorly past the foramen earlier than it doubles again and exits the bone. The muscle tissue of mastication inserting on the mandible include the temporalis, internal pterygoid, exterior pterygoid, and masseter. The capsule is densely innervated with proprioceptive and sensory fibers, which are extraordinarily delicate to refined changes in motion of one or each joints. A slight alteration in occlusion from muscle spasm or a displaced fracture might alter the central notion of joint place. Feedback loops in the central nervous system drive the contralateral muscle tissue of mastication to compensate. Understanding the assorted attachments of the aforementioned muscular tissues of mastication, as properly as the mylohyoid, geniohyoid, genioglossus, and digastric muscle tissue, is necessary in understanding the forces of displacement in a mandible fracture. The floor of the mouth and extrinsic tongue muscles tend to displace fractures posteriorly and inferiorly. The medial pterygoid and masseter muscle tissue act as a sling within the posterior a half of the body and angle space and tend to elevate a displaced fragment of the angle or posterior a part of the physique. Condylar fractures are displaced by the pull of the lateral pterygoid muscle, which rotates and dislocates the fracture medially. A fracture is considered simple when each the exterior pores and skin and oral mucosa are intact, or compound (open) when a laceration in the skin or intraoral mucosa is present. If the patient is dentulous and the fracture line passes into the tooth root, the fracture is theoretically compound as a outcome of the periodontal pocket of that tooth typically extends to the fracture website. The most frequent location of fractures of the mandible is the condylar-subcondylar area. Mandibular fractures can additionally be categorized as dentulous, edentulous, or pediatric. Vertical instability is lent by advantage of the pull of the temporalis, masseter, and pterygoid muscle tissue. On the other hand, if the inclination is in the different way, then the forces of these muscle tissue will distract the distal phase in a superior and medial path.