Aggrenox
Aggrenox dosages: 200 mg, 25/200 mg
Aggrenox packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

Buy discount aggrenox caps 25/200 mg on line
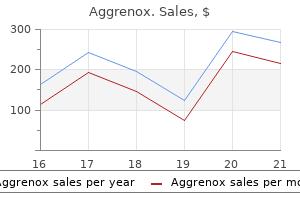
The lending behaviour is negatively punished � the continuing absence of the books reduces the lending behaviour treatment zone lasik aggrenox caps 25/200mg order with amex. Behavioural Treatment of Depression First generation behavioural treatments originated with Lewinsohn (1974) medications bipolar disorder purchase 25/200mg aggrenox caps with mastercard, Ferster (1973) and Seligman (1975). They were administered a mild electric shock, which prompted them to transfer from the placement of the shock to a shock-free area. The shock-free area was then also electrified, so the dogs have been then unable to escape shocks, no matter position they moved to . Helplessness resulted from a set of discovered associations between the situation, their behaviour and its penalties. The canine gave up trying to escape the shock, even after the state of affairs reverted to the original association. Notice that helplessness was not maintained by avoidance; it was the result of giving up on attempts to keep away from. If the behaviour had a major position in maintaining optimistic mood, then doing it much less creates fewer opportunities for reinforcement, which ends up in further discount, and so forth. Positive reinforcement is steadily lowered and this cycle of punishing interaction, decreasing frequency of behaviour and decreased reinforcement explains the persistence of melancholy. The core therapy precept is to improve opportunities for constructive reinforcement by activating behaviour � to restore regular temper and behaviour patterns (Hollon, 2001). Depression is commonly precipitated when contextual occasions influence on an individual, similar to main life stress, important losses, transitions, surprising changes, illness, incapacity and so on. These impacts are highly individual, or idiographic: the way in which such circumstances (antecedents) map onto behaviours and their penalties differs significantly across individuals. In some people this can lead to the discount and extinction of behaviours that have been previously strengthened, and have been key to maintaining enjoyment and euthymic temper. Case Illustration Bob: contextual events Bob was a 54-year-old man who offered with extreme main depression. His difficulties commenced round 10 years previously with rising pressure and bullying in his workplace, ultimately leading to redundancy from his position as a manufacturing unit supervisor. In the intervening interval he withdrew from a spread of social activities that he previously found enjoyable, together with an curiosity in horse racing and hill strolling. He had developed the behavior of spending lots of time indoors, and would spend lengthy durations serious about his previous. Rather than eliciting enjoyment it started to set off stress, anxiety, frustration and anger � all adverse emotions. He initially experienced aid leaving the work state of affairs, but the various work he discovered lacked the rewards of his previous job. Sadness, frustration and anger are comprehensible, and non-pathological, responses to a punishing environment. Thus, within the absence of work his motivation to engage in other mood-enhancing behaviours. This can be established by reviewing the course of the depressive episode and enquiring instantly about adjustments in action and context. This is often a mix of latest behaviours, that are having unhelpful consequences, and the absence of former behaviours, that may have useful penalties in the event that they had been activated. The client must mirror on their actions to find out which behaviours are helpful and that are hindering. This forms the premise of behavioural activation: doing more of the helpful and fewer of the unhelpful. Instead the line of questioning is rather more concrete: explore time, place, events, actions, emotions and penalties. This can feel quite jarring to therapists initially as a outcome of the therapeutic work bypasses meanings and attends extra to concrete experiences. Their emotions and body states tend to deplete regular energy which might make it effortful and difficult to enact usual behaviour. Additionally, at least in the initial part of therapy, the degree of reward from useful behaviours is more doubtless to be much much less potent than is often the case. It is anticipated there shall be highly particular interactions between the person, the situation, their actions and the ensuing emotions and moods. The overall purpose is to determine the results of behaviours on moods, symptoms and associated problems, then scale back depression symptoms via behaviour change. Depending on the functional evaluation this could be lowering avoidance, graded publicity to challenging tasks, exercise scheduling and/or initiating positively bolstered behaviours. A variety of practical analyses of this behaviour were carried out over the primary 4�6 sessions. There was no assumption staying indoors was triggered the same way each time, or had the same penalties. Across numerous situations, two patterns emerged concerning the antecedents and penalties: firstly, Bob tended to keep indoors on days when his mood was initially worse and, secondly, after deciding to stay in he would expertise a noticeable reduction in unfavorable feelings corresponding to tiredness, nervousness and dread. Not surprisingly, shoppers are inclined to experience more unfavorable than constructive affect when in a serious depressive episode. Negative feelings and ugly physique states are highly salient and can be very distressing. Situations and behaviours that scale back the depth of adverse have an result on therefore have a robust chance of being bolstered � not because they intensify constructive affect, however as a outcome of they reduce unfavorable have an result on. This is a good instance of negative reinforcement, in different words, the discount, subtraction or elimination of a consequence that makes it more probably the behaviour will recur. As the day progressed the initial reduction in 100 90 80 Intensity of affect 70 60 50 40 30 20 10 zero 6am 7am 8am 9am 10am 11am 12pm 1pm 2pm 3pm 4pm 5pm 6pm 7pm 8pm 9pm 10pm 11pm 12am Secondary issues. It might also result in a backlog of tasks Bob had agreed to do, and this is able to create tensions in his marriage. When a useful analysis was conducted over the entire day, Bob was able to acknowledge that avoidance offered shortterm relief however longer-term worsening. Preparation Functional analysis is the premise for deciding what to do more (activation) and what to do much less (deactivation). It is discovering together what is helpful and hindering for this specific client in this explicit state of affairs, then planning for behaviour change. It can be useful to contemplate the behaviour in detail; to think about doing it or ideally rehearse it through the remedy session. Therapist and consumer also need to consider whether the behaviour is feasible and manageable at that stage in remedy. Overall there are a number of helpful questions for therapists and clients to ask during the planning and preparation course of: 1. Is the consumer in a place to do the behaviour in the session, or at least imagine doing it He recognized that staying indoors was stopping him enjoying the activities he used to do, particularly hill strolling which had been a passion till he left work 10 years beforehand. The therapist agreed this was a good objective but negotiated to not set a date to do it, as a result of early in remedy it was troublesome to know how much time Bob would need to construct up his vitality and confidence for this task. This is graded task assignment: starting with small manageable steps and building up to tougher targets. Instead Bob and his therapist thought-about how far he was capable of walk at present when he did go out (calibration).
Aggrenox caps 25/200mg quality
Allergic bronchopulmonary mycosis as a outcome of symptoms hepatitis c cheap aggrenox caps 25/200 mg fungi aside from Aspergillus: A global overview symptoms blood clot leg buy aggrenox caps 25/200 mg fast delivery. The results of antifungal remedy on severe bronchial asthma with fungal sensitization and allergic bronchopulmonary aspergillosis. Chest radiographic and computed tomographic manifestations in allergic bronchopulmonary aspergillosis. However, the overwhelming majority of fungal infections of the urinary tract are brought on by Candida spp. The Presence of candiduria might signal numerous pathological states including invasive renal parenchymal illness, fungal bezoars in obstructed ureters, superficial decrease urinary tract infection, and lower urinary tract candidal colonization associated with urinary catheterization. Accordingly, the spectrum of clinical disease embraces asymptomatic candiduria, cystitis, pyelonephritis and renal candidiasis. The urinary tract is also susceptible to infection by one other group of fungi, specifically the endemic fungi including Histoplasma, Blastomyces, and Coccidioides spp. However, these pathogens are hardly ever responsible for the frequent scientific syndromes of urethritis, cystitis, and pyelonephritis. Instead, they often cause prostatitis, epididymitis, persistent bladder irritation or ulceration, ureteric obstruction and persistent renal disease [1]. Point prevalence studies indicate that 20%�25% of wholesome women have constructive vaginal cultures for Candida albicans [6]. However, isolation of Candida from urine cultures of healthy people is rather infrequent. In one examine, funguria was found in solely 1% of sufferers; half of them had diabetes mellitus and had been receiving antibiotics [7]. In distinction, candiduria is a common downside in hospitalized patients with indwelling urinary catheters occurring in up to 83% of patients with 489 490 Fungal infections of the genitourinary tract urinary tract drainage units [4]. In about 10% of instances, a couple of species of Candida may be isolated and candiduria cancoexist with or observe bacteriuria [14]. Pathogenesis and risk elements Ascending an infection is the most common route for infection of the urinary tract. The presence of urinary devices facilitates the introduction of the organism into the bladder. Ascending an infection may result in higher urinary tract an infection within the setting of vesicoureteral reflux or obstruction of the urinary move resulting in pyelonephritis but not often resulting in disseminated infection corresponding to candidemia. Candida cells thereafter penetrate via the glomeruli into the proximal tubules to be shed in the urine [19,20]. The presence of yeast within the urine might indicate widespread dissemination to many organs. In an post-mortem research, renal involvement was noted in 90% of sufferers dying from disseminated candidiasis. Multiple abscesses within the renal interstitium, the glomeruli, and peritubular vessels related to papillary necrosis have been seen in these autopsies [20,21]. Candiduria is a standard discovering in renal transplant recipients with an incidence rate reaching 11% in a single study [24]. Diabetes mellitus is the single commonest underlying disease noted in most studies about funguria [4,14]. This affiliation is expounded partly to insulin deficiency, which affects the intracellular killing system including the myeloperoxidase, hydrogen peroxide, and the superoxide anion system of polymorphonuclear leukocytes resulting in impairment of the phagocytic and fungicidal activity of neutrophils against Candida spp. Furthermore, the expansion of Candida in urine is extra enhanced when urinary levels of glucose exceed one hundred fifty mg/dl. Additional danger elements for the development of candiduria embrace the frequent use of broad-spectrum antibiotics. Antibiotics suppress the conventional flora of the perineum and allows the overgrowth of opportunistic fungi with subsequent ingress over the urethra and colonization or infection of the bladder. In one study, Candida was discovered in the urine of 93% of sufferers who had recently acquired antibiotics [14]. However, carbapenems and third-generation cephalosporin, corresponding to ceftazidime, were found to be related to the best charges of Candida colonization [25]. Several mechanisms have been incriminated for the association between antibiotic use and candiduria. Sulfonamides, for instance, cut back the neutrophil intracellular killing mechanism of Candida. Whereas, tetracycline, doxycycline and aminoglycosides have been shown to suppress neutrophil phagocytosis [26�29]. Besides antibacterial brokers, antifungal brokers, similar to fluconazole, have been shown to favor colonization Genitourinary candidiasis 491 with C. Indwelling urinary drainage gadgets play a serious role in predisposition to candiduria. These devices embrace indwelling urethral catheters, suprapubic catheters, ureteral stents, and nephrostomy tubes. These devices inevitably become colonized with time and serve as a portal of entry for microorganisms into the urinary system. As overseas bodies, they mechanically harm the urinary epithelium and glycosaminoglycan layer and disrupt sufficient antibacterial neutrophil operate allowing yeast overgrowth. In one study, urinary tract drainage gadgets have been present on the time or inside 30 days previous to funguria in 83% of sufferers [4]. Similar phases of growth and the presence of extracellular polysaccharide matrix have also been reported for bacterial biofilms [32�34]. In a scanning electron microscopy study of fifty urethral catheters that had been indwelling for a imply of 35 days, 44 catheters had proof of biofilm formation. Multifactorial mechanisms of resistance in fungal biofilms have been proposed together with the physiological state of fungal cells, the steric hindrance or barrier operate of the extracellular matrix, the overexpression of drug efflux pumps, the variations in fungal membrane sterol composition, and completely different developmental phases. Such a broad spectrum of defense is effective towards many types of antifungal agents and would clarify the issue in eradicating candiduria within the presence of urinary catheters [36�38]. It is necessary to note that each one the aforementioned danger components for candiduria also pre-dispose a affected person to bacteriuria. Asymptomatic candiduria is normally a benign situation that hardly ever leads to candidemia except within the setting of urinary tract obstruction [39]. Conversely, asymptomatic candiduria might be an early predictor or an indication of hematogenous dissemination in critically and chronically ill patients associated with excessive mortality charges if left untreated [40]. Ultimately, there are only a few extensively agreed upon conditions in which asymptomatic patients should be treated for candiduria together with these with neutropenia or a pending urologic procedure. If the second specimen yields no progress of yeast, contamination by the perineal flora is the probably reason for candiduria and no further action should be undertaken [16]. Diagnostic standards differentiating between colonization and infection in sufferers with asymptomatic candiduria are missing. Pyuria and quantitative cultures of urine have proved to be of little value in separating an infection from colonization.
Diseases
- Fluorosis
- Ankyloblepharon filiforme adnatum cleft palate
- Alport syndrome
- Schmidt syndrome
- Physical urticaria
- Onat syndrome
Purchase 25/200mg aggrenox caps free shipping
Safety medications like abilify aggrenox caps 25/200mg online, Effiacy and Pharmacokinetics (pk) of Micafungin (mica) in Pediatric (ped) Patients (pts) symptoms ulcer stomach discount aggrenox caps 25/200 mg without prescription. Population pharmacokinetics of micafungin and its metabolites M1 and M5 in kids and adolescents. Micafungin versus fluconazole for prophylaxis against invasive fungal infections throughout neutropenia in sufferers undergoing hematopoietic stem cell transplantation. International, open-label, noncomparative, medical trial of micafungin alone and together ninety two. Micafungin together with systemic antifungal agents in the treatmentof refractory aspergillosis in bone marrow transplant sufferers. American Society of Hematology forty fourth Annual Meeting; Philadelphia, Pennsylvania, 2002. Although the incidence of bacterial wound infections has considerably decreased with the broad acceptance of topical antibiotics, early burn wound excision, and patient isolation practices, the incidence of fungal wound infections stay unchanged [2,3]. Fungal infections stay a typical explanation for morbidity, mortality, and price in burn sufferers [1�4]. This variation may be the results of completely different standards in the efficiency of surveillance cultures and may reflect variations within the frequency, quality, and quantity of diagnostic efforts in suspected circumstances [5]. In a North American multicenter evaluation of 435 burn patients with optimistic fungal cultures, cultures obtained from burn wounds comprised over one half of all reported fungal cultures. Respiratory cultures were the second most typical culture, site adopted by urine, blood, and different sources [6]. However, whether fungal invasion itself contributed causally to mortality or simply represented a marker for different contributors was not definitely assessed in this report [2]. In addition to wound infections, burn patients are also cited as being among the highest threat teams for invasive fungal infections. Data from the National Nosocomial Infection Surveillance Program demonstrated that burn patients with central venous catheters have the best danger of candidemia of any hospitalized group [8]. In an try and decide the contribution of fungal infections to mortality in burn sufferers, 97 autopsies over a 12-year interval were reviewed [9] and, out of 44% patients with fungal components on histopathology, mortality was attributed to the fungal an infection in 33% (14 out of 42 patients). The most 473 474 Fungal infections in burn patients frequent websites of infections with attributable mortality were wounds (86%) and the pulmonary system (14%), adopted by abdomen, kidney, and fungemia, with some sufferers having multiple sites. Aspergillus and Candida were essentially the most frequently recovered fungi; however, in circumstances where fungus was an attributable reason for dying, Aspergillus was extra generally recovered alone or in association with different fungi. The mostly encountered opportunistic fungal pathogens in burn sufferers include Candida spp. Alterations to innate immunity following burn damage have also been reported and embrace impaired production and release of granulocytes and macrophages from the bone marrow [20], diminished macrophage phagocytic capacity [11] and neutrophil dysfunction [21�23]. Initially, the immunologic response to severe burn injury is pro-inflammatory but later turns into predominately anti-inflammatory in an effort to preserve homeostasis and restore regular physiology [11]. As a results of the secondary anti-inflammatory state and subsequent alterations to the adaptive and innate immune techniques, burn patients are extra susceptible to bacterial and fungal wound infections and severe sepsis [11,12,15]. Although burn wounds are sterile immediately after the thermal injury, these wounds ultimately turn into colonized with hospital-associated microorganisms, including fungi. Furthermore, fungal colonization and wound an infection may also stop adequate wound healing and skin grafting [10]. Occasionally, burn wounds may also become infected with different genera of zygomycetes, especially with Rhizopus or Mucor spp. In addition, necrotic or degenerated tissues are favorable culture media for colonization and growth of assorted microorganisms together with fungi. Broad-spectrum antibiotics, commonly administered to sufferers after severe burn injuries, total parental nutrition, long term invasive monitoring, and deep venous catheters are further risk elements for fungal infections [10]. Furthermore, severe thermal injuries induce a state of immunosuppression that predisposes burn patients to infectious problems [11]. The mechanisms responsible for this decreased resistance to infection stay poorly understood however a quantity of perturbations of each the innate and adaptive immune methods have been documented in animal models and patients [12]. Previous research demonstrated that burn accidents lead to alteration in T-cell perform [12]. Changing sample of fungal an infection in burn patients, 520�528, Copyright 2012, with permission from Elsevier. Hematogenous spread of Aspergillus and Mucor results in in depth pores and skin hemorrhage or necrosis. Hemorrhagic spots and disseminated erythematous nodules may be found on normal pores and skin [3]. Fungal an infection must also be suspected in patients with fever, regardless of the consumption of broadspectrum antibiotics for >7�15 days, and deteriorating condition [24]. Standardized definitions for sepsis and infection which would possibly be particularly relevant to the burn affected person were developed in 2007 [27]. These definitions distinguish the change in affected person status as a end result of an infection from adjustments that occur secondary to the hypermetabolic response of the burn itself (Table 29. The efficacy of biochemical markers of inflammation, such as C-reactive protein, procalcitonin, and interleukin-6 to diagnose sepsis in burn patients, has Table 29. Plus one of many following criteria: � Infection is confirmed on a culture � Pathologic tissue supply identified. However, a latest systematic evaluation means that procalcitonin may be a helpful biomarker for early analysis of sepsis in burn patients [28]. It is crucial to recognize the distinction between the significance of a positive superficial wound culture and "true" infection. The differentiation is made by pathology, in which fungal wound infection is defined as invasion of fungal parts into viable tissue; in distinction, fungal wound colonization is defined as fungal parts in eschar (nonviable burned skin) or "neo-eschar" (a previously excised, now necrotic wound surface), however not viable tissue [2]. Silver-based topical antimicrobials, corresponding to silver sulfadiazine, possess potent bactericidal and fungicidal properties related to their impact on respiratory enzymes in cells of microorganisms [30]. However, these topical agents have the potential for direct toxicity and have been proven to retard wound therapeutic [29]. Silver impregnated dressings present managed and extra extended silver ion launch and sustained concentrations to the burn wounds; moreover, they cut back the risk of nosocomial infection, given restricted number of dressing changes [31]. However, a conclusive proof on the impact of silver-containing dressings or agents to forestall wound infection is missing [32]. Fungal wound infection (not colonization) is independently related to mortality in burn sufferers. Systemic Candida infection in burn sufferers: A case-control study of administration patterns and outcomes. Correlation of tradition with histopathology in fungal burn wound colonization and infection. Incidence of systemic fungal an infection and related mortality following severe burns. Guideline for diagnosis, prophylaxis and remedy of invasive fungal an infection publish burn injury in China 2013. Therapy ought to subsequently be tailor-made based on the fungal speciation and antifungal susceptibility [24]. Once invasive fungal infection through burnt tissue is recognized, especially with Aspergillus or Mucor infection that preserves angioinvasive potential, quick and in depth wound debridement and early closure of wound defect are the surgical approaches to the treatment. Where infected tissue may not be removed, an publicity or semi-exposure technique of wound closure is recommended, with the handled wound stored clean and dry [10].
Order aggrenox caps 25/200 mg fast delivery
The position of childhood abuse and neglect in the sensitization to tense life occasions in adolescent melancholy treatment 1st degree heart block aggrenox caps 25/200mg buy visa. Network destabilization and transition in despair: New strategies for studying the dynamics of therapeutic change medications for anxiety aggrenox caps 25/200mg generic line. Acceptance and Commitment Therapy and the model new behavior therapies: Mindfulness, acceptance and relationship. The comorbidity of main melancholy and anxiousness problems: Recognition and administration in main care. Psychotherapy and medication in the therapy of adult and geriatric despair: Which monotherapy or mixed treatment Cognitive behavioural remedy for delicate to reasonable melancholy and anxiousness: A guide to low-intensity interventions. Predicting optimal outcomes in cognitive therapy or interpersonal psychotherapy for depressed individuals using the Personalized Advantage Index strategy. Comparative efficacy and durability of continuation part cognitive remedy for preventing recurrent melancholy: Design of a References 281 double-blinded, fluoxetine- and capsule placebo-controlled, randomized trial with 2-year follow-up. Is there a job for continuation section cognitive therapy for depressed outpatients Clinical, cognitive, and demographic predictors of response to cognitive remedy for melancholy: A preliminary report. Preventing recurrent melancholy utilizing cognitive therapy with and without a continuation section: A randomized scientific trial. Mental health consequence of long-term and episodic adolescent depression: 15-year follow-up of a community sample. Temperament, character and personality disorders as predictors of response to interpersonal psychotherapy and cognitive-behavioral remedy for despair. Anxious and nonanxious major depressive disorder in the World Health Organization World Mental Health Surveys. Cognitive-behavioral therapy for adolescent depression: A meta-analytic investigation of modifications in effect-size estimates. Journal of the American Academy of Child and Adolescent Psychiatry, 46(11), 1403�1413. A review of main care interventions to enhance well being outcomes in adult survivors of opposed childhood experiences. Insecure attachment, dysfunctional attitudes, and low shallowness predicting potential symptoms of despair and anxiousness throughout adolescence. First onset versus recurrence of depression: Differential processes of psychosocial threat. Evaluation of cognitive diathesis� stress fashions in predicting main depressive dysfunction in adolescents. Natural course of adolescent major depressive disorder in a community sample: Predictors of recurrence in young adults. Moderation of the alliance-outcome association by prior depressive episodes: Differential effects in cognitive-behavioral therapy and short-term psychodynamic supportive psychotherapy. Effects of self-focused rumination on adverse considering and interpersonal problem-solving. Mindfulness-Based Cognitive Therapy for depression: Replication and exploration of differential relapse prevention effects. Relation of the therapeutic alliance with consequence and different variables: A meta-analytic review. Multiple diagnoses in Posttraumatic Stress Disorder within the victims of a natural catastrophe. Cognitive behaviour remedy and supportive therapy for bipolar issues: Relapse rates for therapy interval and 2-year followup. Association between intrusive adverse autobiographical reminiscences and despair: A meta-analytic investigation. An examination of avoidance in major depression compared to social anxiety dysfunction. The effect of mindfulness-based cognitive therapy for prevention of relapse in recurrent main depressive dysfunction: A systematic evaluation and meta-analysis. Psychometric properties of the reconstructed Hamilton Depression and Anxiety Scales. Transduction of psychosocial stress into the neurobiology of recurrent affective dysfunction. Stressful life transitions and wellbeing: A comparability of the stress buffering hypothesis and the social identity mannequin of id change. Mindfulness and reduced cognitive reactivity to sad temper: Evidence from a correlational study and a non-randomized ready list managed research. Cognitive�behavioral remedy of melancholy and depressive symptoms throughout adolescence: A evaluate and meta-analysis. The effects of self-focused rumination on global unfavorable self-judgements in depression. The competences required to deliver effective cognitive behavioural therapy for individuals with melancholy and with anxiousness issues. Antidepressant monotherapy vs sequential pharmacotherapy and mindfulness-based cognitive remedy, or placebo, for relapse prophylaxis in recurrent depression. Cognitive reactivity to unhappy temper provocation and the prediction of depressive relapse. Mechanisms of change in mindfulness-based cognitive remedy for despair: Preliminary proof from a randomized managed trial. Intrusive reminiscences and rumination in sufferers with post-traumatic stress disorder: A phenomenological comparison. Intrusive photographs and recollections of earlier adverse events in patients with obsessive compulsive disorder. Sudden gains and important periods in cognitive-behavioral therapy for depression. Cognitive changes, crucial sessions, and sudden gains in cognitive-behavioral therapy for melancholy. Case formulation in cognitive behaviour therapy: the remedy of challenging and complex cases (2nd ed. Emotional processing, three modes of mind and the prevention of relapse in depression. How does cognitive remedy stop depressive relapse and why should attentional control (mindfulness) coaching help Prevention of relapse/recurrence in main depression by mindfulnessbased cognitive remedy. Animal intelligence: An experimental research of the associative processes in animals. Effort-based decisionmaking in main depressive dysfunction: A translational mannequin of motivational anhedonia. Exploring the roles of method and avoidance in melancholy: An integrative model. Developmental trauma disorder: Toward a rational prognosis for children with complex trauma histories.
Effective 25/200 mg aggrenox caps
The device is indicated within the outpatient setting where affected person mobility is necessary treatment quinsy purchase aggrenox caps 25/200 mg line. When used alone symptoms west nile virus 25/200mg aggrenox caps sale, or along side surgical procedure, it promotes normal spinal cord alignment, decompression of the nerves and spinal cord, safety of soppy tissues, and bone healing. The initial use of skeletal traction for the therapy of spinal fractures has been attributed to Hippocrates and the Greeks in the 4th century B. The system consisted of forceps which were spread aside and affixed to the again of the neck. Citing the growing number of automobile accidents and hyperflexion accidents, Alfred Taylor outlined a technique by which pores and skin traction could be used to stabilize the cervical backbone. It utilized the mandible and inion for support and was used successfully in the administration of pediatric atlantoaxial rotatory subluxations and cervical radiculopathy in grownup patients. Relative contraindications might embody occipitocervical dislocations and subluxations, intracranial pathologies requiring open surgical management. She had neck pain, an lack of ability to move her lower extremities, and weak point and numbness in her hands. A detailed neurological assessment confirmed an American Spinal Injury Association A spinal twine damage at the C7 degree. Six-month postoperative photographs present strong fusion with bridging trabecular bone and no motion between the spinous processes on flexion/extension views. The affected person regained motor and sensory capabilities in the preliminary forty eight hours following surgery. The rationale for going immediately to traction was the complete injury and the perceived have to scale back the subluxation as quickly as possible. In this setting, our opinion was that magnetic resonance imaging would delay the treatment and could reduce the possibility of a neurological recovery. Once a radical history has been taken and a detailed neurological evaluation (including analysis of sensation and motor responses) of the affected person has been carried out, she or he is placed within the supine position on a tough floor. The sites where the 2 pins are to be inserted ought to be cleaned with an anti- septic resolution. The pins are positioned 2 cm superior to the pinna consistent with the exterior auditory meatus whereas being inferior to the equator of the calvarium to forestall slippage. They can be positioned anterior to , consistent with, or posterior to the exterior auditory meatus relying on the degree of neck flexion or extension required to obtain spinal cord decompression and cervical alignment. Manipulation of the peak of the rope-and-pulley system allows for control of the degree of flexion or extension of the cervical spine. Tighten each pins concurrently until torque indicator on one pin protrudes roughly 1 to 2 mm, indicating adequately tightened screws. Pearls: � Pay attention to eyes and eyebrows to keep away from pinning eyes open or closed. For children: Use lower last torque for tightening (4�8 inch-lb for kids aged 3�10 years, 2�4 inch-lb for kids beneath age three years). Use multiple (6�10) pins so as to distribute stress evenly circumferentially and keep away from fracture or extreme skull penetration. Also, use specifically equipped pediatric pins with short ideas and wide flange, if out there. Once in place, secure the ring to the posts at each level with torque wrench, maintaining head in right alignment. Check post-placement X-rays instantly after placement and when upright day 1 and day three. Pearls: � Important note: Every brand and magnificence of halo vest and head ring comes with a detailed set of directions for utility. It is beneficial to review these instructions fastidiously previous to making use of the apparatus. Some surgeons have used 5 lb per level as the utmost amount of weight utilized, while different prior studies have recommended traction weights of forty five to eighty pounds be utilized. Typically, upon reduction of a subluxation, a traction weight between 15 and 20 lb is enough to keep the discount. They discovered that 68% of patients in their cohort had an improvement in neurological standing following the applying of traction. Based upon a cadaveric evaluation, they suggested that the tongs might help traction weights of as much as a hundred lb. Of observe, these "high-weight" reductions have been performed underneath steady direct observation by the remedy group who immediately decreased the weight upon achieving discount. The common time taken to obtain discount in these 39 Cranioskeletal Traction for the Management of Trauma to the Cervical Spine attempted inside the initial 8-hour period immediately following injury. This would counsel that a neuroprotective effect could additionally be present for a brief time period following damage. In sufferers with neurological injuries with radiographic evidence of canal compromise, our practice has been the instant utility of traction within the emergency department. Prospective randomized control research evaluating the optimum time level at which closed discount for spinal twine decompression must be attempted could be perfect. There is a small but actual risk of displacing or dragging disc materials posteriorly into the spinal canal with any technique of discount, probably inflicting neurological compromise. Obtunded or intubated patients with an unknown neurological status require a selection. She was delivered to the emergency room, awake and coherent, and a neurological examination demonstrated only a proper sided C5 nerve deficit. Abnormal signal traversed the C4�C5 disc house and there was splaying of the spinous processes of C4�C5 with abnormal sign within the interspinous ligaments. Upon noting the massive disc herniation at C4�C5, the decision was made to not make the most of traction (out of concern for inducing a cord deficit); rather, a direct operation was carried out which decompressed the wire anteriorly and then stabilized posteriorly. The actual time point following harm at which closed discount must be performed stays unclear. Cotler and colleagues have noticed greater neurological restoration if discount is 5. Patients can also develop stress ulcers over the occiput if craniocervical traction is maintained for prolonged intervals of time. Lerman et al posit that the pullout power also decreases in heavily used tongs due to wear-and-tear on the pins/pin springs. In such cases, alternative or recalibration of the tongs could additionally be indicated to prevent device failure and/or detachment from occurring. A torque wrench is used to tighten the pins to a pressure no larger than 10 inch-lb to stop penetration of the inner table. Hexagonal lock nuts, which are threaded onto the ends of the pins, are used to forestall pin loosening and detachment. In pediatric sufferers, further pin sites may be used to improve the distribution of the traction weight. It additionally allows for management of the backbone in three totally different planes and can be utilized efficiently following discount with the halo ring as a substitute for surgical decompression. It may additionally be used as an adjunct following open reduction and inner surgical cervical fixation. Bucholz et al reported on 109 sufferers who underwent fixation for C1�C2 accidents (including atlantoaxial subluxations, hangman fractures, axial body fractures, and arch fractures of the atlas) and C3�T1 accidents.
Discount aggrenox caps 25/200mg otc
However treatment brown recluse bite 25/200mg aggrenox caps for sale, the sample of temper variation was as important as her signs at any cut-off date symptoms rheumatoid arthritis cheap 25/200 mg aggrenox caps otc. Evelyn was achieving quicker recovery from depressed moods, had much less severe signs throughout depressed phases, and fewer residual signs following them. However, she reported ruminating much less about negative emotions and never letting them get in the way of her plans to the identical extent. She described less self-loathing and a greater perception that depressed moods would reverse. During periods of despair, Evelyn would doubt there had been any change, or no less than not one that was significant to her. Staying Well In Chapter 4 we thought-about strategies for preventing relapse and staying nicely. Notice that Evelyn had several of the vital thing options of shoppers at larger risk of relapse: � � � � Significant childhood adversity � uncared for emotional and help needs. Unstable remission � response to treatment, however with intermittent symptom reversals and residual symptoms. It was due to this fact important to prioritize Evelyn for continuation remedy, so she moved into a 21-month continuation section, with roughly month-to-month booster sessions. Consequently the therapeutic focus was to help Evelyn reverse the consequences of reactivation when it occurred: to resist impulses to avoid, withdraw, escape or disengage; flip consideration to current wants and wishes; have interaction in behaviours to satisfy these needs; replicate on the consequence of actions rather than ruminate about meanings and implications. Given her danger profile, there was likely to be a gap between the challenges produced by cognitive reactivation, and her capability to stay nicely through implicit data. Practitioner Tips: Highly Recurrent Depression � In highly recurrent melancholy, minor stress can be adequate to trigger depressive episodes, via a strategy of cognitive reactivation. Rather than making an attempt to keep away from it, find out how best to respond in order that depressed moods are reversed and time-limited. Highly Recurrent Depression � Major life stress is much less likely to be the treatment focus, as a result of despair may be precipitated with out it. However, life stress sometimes occurs, and when it does contextual factors need to be included in remedy in the ordinary method. For instance, if suicide is engaging because it will put an end to psychological turmoil and escape a foul relationship, explore other methods of discovering mental peace and resolving relationship problems. It also can assist to uncouple self-depression fusion, in different words, identification with the depressed state. Encourage reflection on how unhelpful self-identities became internalized; this can give purchasers an alternate reason why they generally dislike themselves and become depressed. Sometimes shoppers over-invest in a single most well-liked self-identity to deactivate other self-representations that have a miserable effect. There is a logic to this strategy, but it may possibly slim consideration within the over-invested area and lead to secondary problems. When this occurs, encourage diversification in order that the shopper has a broader range of helpful identities. People with highly recurrent despair are vulnerable to relapse and recurrence, notably in the event that they: (a) have an unstable remission with residual signs; (b) suffered trauma, neglect or abuse in childhood; (c) experienced an earlyonset despair throughout adolescence (see Chapter 7). It is crucial to provide booster periods to high-risk purchasers, to assist them consolidate and generalize their studying. Memory for the therapy could be incomplete and implicit, so continuation ought to purpose to make their studying more specific. This has implications for parameters such because the dose of remedy and frequency of remedy periods (McCullough, 2003). In Chapter 8 we noticed how recurrent despair can have a reactivating, oscillating pattern with people switching between different mood-states. These options also can present in chronic depression, however the extra common pattern is a steady depressed state with individuals enjoying few, if any, intervals of wellness and euthymic mood (Barnhofer, Brennan, Crane, Duggan & Williams, 2014). As we famous in Chapter 2, less skilled therapists typically wrestle treating persistent melancholy: it could be frustrating and dispiriting when the change process is tough and gradual. Chronic Sub-types Twenty per cent of major depressive episodes develop a persistent and chronic course and threat factors for this embody: family history of mood dysfunction, historical past of childhood abuse, early-onset depression and excessive ranges of comorbidity (Garcia-Torro et al. Not surprisingly, when purchasers have been depressed for a long time period they tend to experience self-depression fusion, helplessness and hopelessness (Riso & Newman, 2003). It is helpful to think about different patterns of chronicity, and in our experience four questions are essential to ask clients within the assessment phase: 1. They will assist to inform the therapy parameters and therapeutic strategy more than likely to be helpful in every case. In our experience, the answers to these questions reveal three major persistent sub-types that require a subtly different treatment approach: latest chronicity, prior wellness and lifelong depression. Without intending it, depressed clients can under-represent periods of wellness in their life, as a result of recollections of those instances are much less available during depressed moods. It is therefore helpful to ask specific questions on different phases of life, and triangulate the answers with scientific information and family member accounts. Some clients may have skilled long-term gentle depression, called dysthymia, with major episodes superimposed. Other shoppers may have skilled recurrent episodes that gradually become more persistent and persistent. Others could have sustained intervals of wellness with persistent episodes interspersed, and so forth. What matters is to determine the related features for every case and reply to them as wanted. A one that has been depressed for two years has a unique change potential in contrast with somebody who has been depressed for 20 years. Two years is probably a small proportion of their whole life: 7% in a 30-year-old, 5% in a 40-year-old, 4% in a 50-year-old, and so on. As would be anticipated, individuals who have been depressed a very lengthy time are prone to have obtained quite a lot of therapies, both pharmacological and psychological. Others may have uncommon or complicating components which are contributing to the persistence of their difficulties. No Could uncommon or complicating factors be contributing to the persistence of the melancholy In the thoughts of the client, these could have the looks of a full course of treatment. This can really feel more practical to clients who, by now, tend to really feel helpless and hopeless about change. The major difference in contrast with non-chronic despair is the higher likelihood of slow and gradual change so, on average, clients need an extended time frame to overcome the depressed state, not only a greater variety of classes. It is essential to make these expectations explicit during remedy planning, for example, to ask how soon the shopper is hoping to really feel higher, what it will be like for them if progress is sluggish to start with, and so on. What works finest is to provide blocks of classes with proximal goals, for example, offering round ten periods initially to discover out what progress can be made.
Sweet Dock (Bistort). Aggrenox.
- Digestive disorders like diarrhea, mouth and throat infections, wounds, and other conditions.
- How does Bistort work?
- Dosing considerations for Bistort.
- What is Bistort?
- Are there safety concerns?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96120
Aggrenox caps 25/200mg low cost
Patients might present with vertebrobasilar insufficiency (dizziness symptoms multiple sclerosis buy aggrenox caps 25/200mg overnight delivery, ataxia medicine hat jobs 25/200mg aggrenox caps cheap with amex, and vision changes), dysphagia, facial numbness, vertigo, Horner syndrome, or indicators of anterior spinal wire ischemia (complete motor paralysis, lack of ache and temperature, autonomic dysfunction, areflexia, urinary retention, and retained proprioception and vibratory sensation). Radiography, though less delicate and specific than the superior techniques, has historically been used for initial 28 Initial Assessment (Including Imaging) of Cervical Spinal Cord Injury imaging in awake patients. In addition, soft-tissue pathology and presence of a hematoma could be evaluated with using soft-tissue home windows. Dynamic views have been advocated in the awake, cooperative, symptomatic patient with regular static X-rays to exclude discoligamentous injuries. The occipitocervical and subaxial spine is assessed for occipitocervical damage, atlantoaxial fractures and instability, side dislocations, vertebral physique fractures, listhesis, and posttraumatic kyphosis, among other accidents. Radiographs can be used to determine atlanto-occipital dissociation; however, the sensitivity for figuring out pathology is poor. Vertebral bodies should be analyzed for radiolucencies indicating fracture strains, height loss, subluxation, facet pathology, and angulation. Distraction of spinous processes on lateral radiographs indicates a hyperflexion mechanism. Soft-tissue damage anterior to the cervical spine is represented by prevertebral soft-tissue swelling, which is measured between the anterior floor of the vertebral our bodies and the air shadow of the airway. Various limits of normal have been reported from roughly three to 10 mm between C2 and C4. In addition to traumatic accidents, underlying degenerative modifications and congenital stenosis of the cervical spine are necessary to acknowledge because of their contribution to cord accidents, similar to central wire syndrome. The morphology of the fractured lamina and left pedicle is well visualized, in addition to protrusion of bony fragments into the spinal canal. The condyle�C1 interval has the very best sensitivity and specificity for atlanto-occipital dissociation among all measurement parameters. Spinal cord compression against the posterior cortex of C2 and a excessive rate of neurological injury42 occurs after these atypical fractures. In addition to delineating bony pathology, traumatic disc herniations and epidural hemorrhage could be identified by soft tissue and lung windows. Flanders et al50 reported that craniocaudal length of edema and excessive cervical lesions correlated with poor functional outcomes. Sagittal T2-weighted photographs are crucial for the analysis of the spinal twine and are the one sequences which have prognostic worth, but axial pictures also provide element about the quantity of spinal twine compression, canal compromise, and placement of disc herniation. T1-weighted photographs, in distinction, present excellent delineation of anatomic buildings together with the most important ligaments of the backbone. Spinal cord pathology may additionally be assessed on T1 imaging regardless of the normal use of T2 sign abnormalities for routine scientific assessment. Edema, hyperacute hemorrhage, and infarction appear dark on T1-weighted imaging whereas subacute hemorrhage may be seen as a bright signal. Hemorrhage within the spinal twine is identified by hypointensity on T2-weighted imaging. Hemorrhage generally happens in the nuclei of the spinal cord and represents the point of most impact. In the cervical backbone, intraspinal hemorrhage reflects a whole neurological injury. In the case of a bigger hemorrhage, more time is required for deoxyhemoglobin to be transformed into methemoglobin. A thorough evaluation of anterior and posterior ligamentous structures is crucial especially within the setting of vertebral subluxation or dislocation. The ligamentous anatomy of the higher cervical backbone maintains spinal alignment and stability. The failure of all anterior buildings or all posterior plus two anterior constructions is a threat issue for cervical instability. Posterior ligamentous complicated accidents can have an effect on the supraspinous ligament, interspinous ligament, and ligamentum flavum. Ligamentum flavum injury may be seen as discontinuity or displacement into the thecal sac. Additional accidents have been identified in 12% of patients, which included ligamentous accidents, fractures, and dislocations. Subluxation, transverse foramen fractures, and cervical accidents between C1 and C3 are probably the most commonly cited danger components for arterial harm. In this examine, intramural hematomas are seen on T1 imaging as a hyperintense rim surrounding a circulate void. An improve in arterial diameter compared to the contralateral artery is one other indicator of injury. Disadvantages, similar to size of imaging time, undefined effectiveness of imaging further physique areas in the acutely injured affected person with this modality, and low specificity and sensitivity, restrict its use within the trauma setting. Marrow edema from trabecular microfractures signifies vertebral body fracture but edema is much less prone to happen in the bony posterior components. This imaging technique measures pace and directionality of water molecules alongside linear structures, corresponding to nerve fibers, and identifies abnormalities of linear molecular movement. Fractional anisotropy is a commonly referenced parameter that ranges from zero (representing isotropic diffusion or movement in a sphere) to 1 (representing anisotropic diffusion in a cylinder). Fractional anisotropy normally approximates the worth "1" as a end result of intact nerve fibers are lengthy, thin cylinders. If an injury happens, the diffusion of water molecules becomes unrestricted (isotropic) and approaches "zero". Cervical fractures are sometimes secondary to hyperextension and are unstable, three-column injuries. As a end result, the risk of neurological harm after cervical injury is 3 times larger than the general population. In a evaluate of ankylosing spondylitis patients with cervical fractures, radiography when used alone was unable to visualize the complete cervical backbone in 92% of sufferers, and solely 48% of fractures could probably be identified. Introduction to the guidelines for the management of acute cervical backbone and spinal twine injuries. Reliability and validity of the International Spinal Cord Injury Basic Pain Data Set gadgets as self-report measures. Prospective screening for blunt cerebrovascular injuries: evaluation of diagnostic modalities and outcomes. Blunt cerebrovascular harm in cervical spine fractures: are more-liberal screening standards warranted Vertebral artery accidents associated with cervical spine injuries: a evaluate of the literature. Incidence of vertebral artery thrombosis in cervical spine trauma: correlation with severity of spinal wire injury.
Buy cheap aggrenox caps 25/200 mg line
Select reactions have been reported to happen extra frequently with certain formulations asthma medications 7 letters proven aggrenox caps 25/200mg. A potential analysis discovered a 20% imply total frequency (range 0%�100%) of acute infusionrelated reactions amongst eighty four sufferers at 64 facilities [121] treatment croup aggrenox caps 25/200mg for sale. While these reactions hardly ever required discontinuation of therapy, slowing the infusion fee had no impact on the infusion-related reactions described. Reactions in particular person sufferers can also be formulationspecific and never necessarily recur upon rechallenge with a unique formulation. Renal dysfunction secondary to amphotericin B administration is often the treatmentlimiting opposed impact of amphotericin B. Proposed mechanisms include direct interaction with epithelial cell membranes (causing mobile disruption) and renal vasoconstriction (with resulting reductions in renal blood flow) [124,125]. Manifestations could embody renal tubular acidosis, casts within the urine, azotemia, oliguria, and magnesium and potassium losing [124,125]. The incidence of amphotericin B-induced nephrotoxicity varies extensively between research because of differences in definition, research population, underlying risk factors, period of remedy, formulation and use of premedications. However, such reactions (often described as a doubling of the baseline creatinine value) have been reported as much as 50% of sufferers receiving AmBd [126�131]. Risk elements embody underlying renal dysfunction, formulation, concomitant nephrotoxins, and dosing (daily and cumulative) [128,132�135]. Numerous methods have been employed in attempts to reduce the incidence and severity of amphotericin B-induced renal dysfunction. This consists of cautious affected person choice and (whenever possible) minimizing concomitant nephrotoxins. Use of saline loading [125,138�140], aggressive fluid resuscitation [141], and steady infusions [142,143] have also been investigated. Studies evaluating the incidence of nephrotoxicity between preparations has additionally been evaluated. Hematologic toxicities associated with the administration of amphotericin B mostly include anemia, leukopenia, and/or thrombocytopenia [147]. Anemia (usually normochromic, normocytic) has been reported secondary to amphotericin B administration, and could additionally be a consequence both of direct inhibition of erythropoietin [148] or secondary to renal toxicity. Hematological most cancers was also a threat issue for severe thrombocytopenia in sufferers receiving amphotericin B. Elevations in liver function tests have much less incessantly been associated with amphotericin B administration [149]. This could embody oropharyngeal, cutaneous, mucocutaneous, and vulvovaginal infections. The efficacy of AmBd caused by many Candida spp has been established in invasive candidiasis, together with candidemia, osteomyelitis, disseminated candidiasis, endophthalmitis and endocarditis [5,151�153]. Use in candidemia is mostly restricted to settings where drug intolerance or resistance has been demonstrated to alternate treatments [5]. Extensive expertise with AmBd has also been documented for invasive candidiasis in the neonatal population [154,155]. More lately, AmBd has been used because the comparative agent towards each caspofungin [105] and voriconazole [156]. In the case of voriconazole, an alternative exists for continued oral remedy once the patient is secure. It has been studied in an open label, phase-I [118] and retrospective evaluation of open-labeled trials. The potential function of AmBd as a part of combination therapy (with fluconazole) was examined in a randomized examine in non-neutropenic patients with candidemia [161]. The availability of equally efficacious and bettertolerated agents limits the role of amphotericin B for invasive candidiasis. In addition to its continued function in severe illness [162], some authorities [163] acknowledge the potential for a continued function within the therapy of neonatal infections. For many years, AmBd represented the usual of take care of the therapy of invasive aspergillosis [4,164]. Overall efficacy rates various with preparation, inhabitants, website of infection, and affirmation (possible, probable, definite). While amphotericin B maintains activity in vitro against zygomycetes, therapy outcomes (especially within the immunocompromised host) stay poor [186,187]. AmBd [188] or lipid-based formulations [188,189] of amphotericin B are regularly prescribed in this clinical setting, particularly as initial therapy and frequently together with surgical intervention [187,188]. Patients improved or with stable disease following initial AmBd remedy (usually two weeks) can usually be transitioned to azole remedy. In a randomized, double-blind multicenter examine for disseminated histoplasmosis evaluating AmBd (0. However, no distinction in time to defervescence, price of blood culture conversion, or change in Histoplasma capsulatum antigen levels was observed. AmBd can be the popular remedy for immunocompromised or pregnant sufferers [8,200]. Low relapse rates have been reported when cumulative doses of AmBd larger than 1 g have been employed. In common, using amphotericin B for the therapy of sporotrichosis is restricted to pregnant sufferers or these with osteoarticular, pulmonary, or Adverse effects 161 disseminated infections [9]. In an identical circumstance, fluconazole and itraconazole have largely replaced the need for the use of amphotericin B in the therapy of coccidioidomycosis [10,201]. Due to lack of medicine energetic towards most of the emerging mycoses, restricted optimistic medical experience (primarily case stories or case series) and/or in vitro information has been reported for amphotericin B towards Exophiala oligosperma [202] and uncommon molds [203]. Numerous research have examined the efficacy and security of amphotericin B in the treatment of fever in neutropenic oncology sufferers. Early revealed experience with AmBd helped establish a task of antifungal therapy in empiric regimens for sufferers persistently (>7 days) febrile despite broad-spectrum antibacterials [204,205]. However, given the expanded options of alternative therapies and the underlying risks for toxicities related to amphotericin B, revealed tips for the empiric management of fever in neutropenic oncology patients suggest limiting the role of amphotericin B in this patient inhabitants [214,215]. These might embrace sufferers at highest danger and/or with scientific proof or radiologic evidence for invasive fungal infections (such as aspergillosis or mucormycosis) or these receiving prior azole remedy susceptible to invasive mould infections. Orally-administered nystatin has been examined as an antifungal prophylaxis in a wide range of populations, including low birthweight infants [217], oncology [218], and stable organ transplant recipients [216,219]. In select patient populations (such as strong organ transplant recipients), use of nystatin has largely been changed by azoles [216,219]. Current printed pointers for the prevention of invasive fungal infections in most cancers sufferers mirror that the toxicities of amphotericin B, along with the expanding choices for alternate methods, limit the routine use of amphotericin B on this setting [214,215]. Amphotericin B has also been examined as an antifungal prophylaxis in select stable organ transplant recipients [231� 234]. Active remedies demonstrated superior infection- and colonization-free charges when compared with placebo (40. Prophylactic strategies for strong organ transplant recipients vary widely between transplant facilities and patient populations. Such infections could include cryptococcosis, histoplasmosis, and coccidiodomycosis. However, due to the supply of alternate agents (such as fluconazole and itraconazole), amphotericin B performs a limited position in such prevention.

Aggrenox caps 25/200mg order on-line
After 14 days of dosing harrison internal medicine buy 25/200mg aggrenox caps with mastercard, the variations between those that had obtained a loading dose and the nonloading dose group have been much less pronounced symptoms 13dpo 25/200mg aggrenox caps mastercard, with C1h approximately 9 g/mL and C24h roughly 1. Caspofungin doses of 70 mg every day for 14 or 21 days resulted in greater serum concentrations on the finish of infusion (approximately 15 g/mL) and higher concentrations 24 hours after the dose (approximately 2. This means that steady-state was not reached by day 14, however subjects had been approaching steady-state by the third week of dosing [61]. A latest investigation additionally highlighted apparent differences in susceptibility between echinocandins amongst C. A research evaluating echinocandin resistance in Candida glabrata found that the proportion of resistant isolates elevated between 2001 and 2010. There are different reports of scientific failures due to isolates with reduced susceptibility to echinocandins, suggesting that other unknown mechanisms may also contribute to echinocandin resistance [47]. A paradoxical impact of fungal organisms with regrowth at excessive echinocandin concentrations has been reported in several in vitro investigations, and additional complicates the examine of echinocandin resistance [49]. In the presence of excessive concentrations of echinocandin, it has been advised that resistance mechanisms among Candida and Aspergillus spp. The majority of reviews have occurred with caspofungin, but one current paper additionally noticed these effects with micafungin and anidulafungin in opposition to sure isolates [49�54]. This impact was additionally not obvious in clinical research of invasive candidiasis [52,56�58]. One research suggests that prime concentrations of echinocandins restore the enzyme -1,3-glucan synthase, presumably by recruiting chaperone proteins [59]. Based on these knowledge, further studies are needed to additional elucidate the scientific and microbiologic significance of the paradoxical effect reported with echinocandins. Following doses of 50�150 mg/ day, micafungin displays linear pharmacokinetics with doseproportional increases in serum concentrations. Steady-state concentrations sometimes are achieved after 4 days of intravenous dosing. Micafungin undergoes ring opening and liver metabolism to three metabolites: M1, M2, and M5. M1 undergoes arylsulfatase transformation to a catechol kind, which is then remodeled by catechol-o-methyltransferase to a methoxy form (M2). Fecal excretion is the primary route of elimination, with 71% of the dose eradicated as parent drug and metabolites 28 days after dosing. One research means that when weight will increase to above 66 kg, the systemic clearance of micafungin will increase by a measurable issue and continues to increase with weight with no observable plateau this implies that obese patients might require adjusted dosing [67]. Anidulafungin Anidulafungin is extremely protein certain (>99%) and has a larger apparent quantity of distribution (30�50 L) and considerably longer half-life (26�40 hours) than the other echinocandins (Table thirteen. Doses of one hundred mg once every day, following a loading dose of 200 mg intravenously end in trough concentrations of two. Overall, pharmacokinetic parameters in contaminated patients were similar to that previously reported among wholesome volunteers. Drug clearance was faster among males and people with increased body weight, but only defined a small proportion (20%) of intersubject variability noticed with anidulafungin. In addition, both women and men with invasive candidiasis appeared to have approximately 30% faster clearance than subjects with oropharyngeal/esophageal candidiasis or invasive aspergillosis. Tissue concentrations Substantial information describing tissue concentrations of echinocandins have emerged from both animal models and human investigations (Table 13. After intraperitoneal administration in murine models (60), caspofungin had the very best ratio of tissue-to-plasma concentrations within the liver (16), followed by kidneys (2. In rats, micafungin had the highest concentrations in lung, kidney, and liver with tissue:plasma ratios of three. Administration of a single intravenous dose of 5 mg/kg of radiolabeled anidulafungin in rats resulted in the highest tissue-to-plasma concentrations in liver [12. Although human studies and case reports are scarce some have shown the extent of tissue penetration of the echinocandins. Caspofungin ocular penetration is poor with case reports describing undetectable to very low intraocular levels (6% of plasma concentration) in patients with fungal endophthalmitis [77,78]. However, caspofungin has excellent lung penetration with high ranges (more than five occasions the plasma concentration) being reported in the alveolar cells of a lung transplant patient receiving remedy for suspected pulmonary aspergillosis [80]. Micafungin has wonderful penetration into the cellular components of the lung with more than 100% of plasma concentration depositing in alveolar macrophages of healthy volunteers. Elderly Pharmacokinetics of caspofungin and micafungin has been studied in elderly topics, and have been similar to nonelderly adults [85,86]. With caspofungin dosing, six aged males and 6 elderly women (67�77 years of age) with creatinine clearances 60 mL/min had barely greater serum concentrations of caspofungin at 1 hour and 24 hours after infusion compared to younger men (aged 24�44 years) [86]. With micafungin, pharmacokinetics amongst 10 aged (66�78 years of age) volunteers was similar to 10 younger men (20�24 years of age) receiving single intravenous doses of micafungin 50 mg [85]. Pharmacokinetics of anidulafungin has not been specifically reported in elderly patients. Women Serum concentrations amongst ladies receiving echinocandins could additionally be relatively larger than that among men, but no dosage changes are currently really helpful on the basis of gender [3�5]. Plasma concentrations of caspofungin amongst patients with mild- to end-stage renal disease receiving 50 mg day by day for remedy of invasive aspergillosis or candidiasis have been just like that amongst sufferers with no renal impairment [5]. Anidulafungin pharmacokinetics among 26 subjects with renal impairment or end-stage renal disease had been similar to eight subjects with regular renal function following single intravenous doses of fifty mg anidulafungin [91]. Pharmacokinetics of anidulafungin was not affected in these undergoing hemodialysis, whether anidulafungin was given earlier than or after a dialysis session [91]. Pharmacokinetics of micafungin in those with severe hepatic impairment was described amongst 9 liver transplant recipients. Pharmacokinetics of anidulafungin amongst subjects with mild-to-moderate hepatic dysfunction was much like wholesome controls receiving single 50 mg doses of anidulafungin. Clearance was elevated by 57% in these with extreme hepatic impairment, with 78% increase in quantity of distribution that might be potentially attributed to ascites and edema. Burn sufferers using caspofungin to deal with candidemia in burn sufferers was investigated in a case report of two sufferers. One explanation is the hypoalbuminemia seen in burn sufferers, since caspofungin is nearly 97% certain to albumin. However, a larger pattern dimension is required to investigate this variability amongst burn patients. It may be essential to monitor therapeutic drug ranges in burn sufferers receiving echinocandins to optimize dosing [94]. Hepatic insufficiency Hepatic insufficiency appears to scale back elimination of caspofungin and micafungin, whereas plasma concentrations of anidulafungin are decreased in those with severe hepatic impairment receiving anidulafungin [5,92]. Dose reduction ought to be thought-about when administering caspofungin to sufferers with moderate hepatic insufficiency [5]. In this examine, subjects with moderate hepatic impairment received 35 mg every day, following the 70 mg loading dose. Serum concentrations have been reduced with growing body weight (>75 kg), but had been elevated amongst those with albumin concentrations >23. Of the themes studied, 75% have been within the goal concentration range of 1�3 g/mL during remedy.
Aggrenox caps 25/200 mg visa
Injury induces poor interleukin-12 production in treatment online aggrenox caps 25/200mg discount otc, but interleukin-12 therapy after damage restores resistance to infection symptoms dizziness nausea 25/200mg aggrenox caps discount fast delivery. Induction of worldwide anergy somewhat than inhibitory Th2 lymphokines mediates posttrauma T-cell immunodepression. Marrow granulocytemacrophage progenitor cell response to burn harm as modified by endotoxin and indomethacin. Impaired perform of polymorphonuclear leukocytes in patients with burns and different trauma. Comparison of quantitative microbiology and histopathology in divided burn-wound biopsy specimens. American Burn Association consensus convention to define sepsis and an infection in burns. Serum procalcitonin as a diagnostic biomarker for sepsis in burned sufferers: A meta-analysis. Amsterdam, the Netherlands: Elsevier Science Health Science division, 2012:137�156. Susceptibility to allergic bronchopulmonary aspergillosis was also associated with polymorphism of Toll-like receptor 9 [20]. Fungal conidia are immunologically inert because of the presence of floor hydrophobin that forestalls immune recognition of airborne fungal spores [23]. In asthma and cystic fibrosis sufferers and secondary to defective airway clearance, spores are trapped by the luminal mucus and subsequently germinate, and form mycelia [24]. Normally the hyphal forms are killed by lung macrophages and neutrophils, that are the primary line of defense [25,26]. The consequences of this response are intense airway inflammation, airway harm, and reworking with the development of bronchiectasis and fibrosis. Patients usually manifest with uncontrolled asthma, wheezing and productive cough. According to the brand new proposed standards, the diagnosis of allergic bronchopulmonary aspergillosis requires the following [1]: Predisposing situations (one should be present): Bronchial asthma Cystic fibrosis Obligatory criteria (both should be present): Positive Aspergillus skin check or elevated IgE levels in opposition to A. Cavities and pleuropulmonary fibrosis are normally suggestive of the development of continual pulmonary aspergillosis (see Table 30. Allergic bronchopulmonary aspergillosis: Review of literature and proposal of latest diagnostic and classification criteria. The first is the attenuation of the inflammation and immunologic response, for which corticosteroids are the mainstay of remedy. The second is the attenuation of the antigen burden arising from fungal colonization of the bronchial tree. Furthermore, improvement in lung operate and time to first exacerbation have been similar within the two groups. Reducing the fungal burden within the respiratory tract by utilizing an antifungal might decrease antigenic stimulation, scale back inflammatory response, ameliorate signs, and possibly scale back the long-term danger of disease progression. Treatment with itraconazole lowered eosinophilic airway irritation, serum IgE levels and exacerbations requiring oral corticosteroids remedy compared to the control group. Treatment group was reported to have more response outlined as a discount of at least 50% within the corticosteroid dose, a lower of at least 25% within the serum IgE focus and improvement of no much less than 25% in train tolerance or pulmonary-function exams or resolution or absence of pulmonary infiltrates. A randomized managed [1] trial to research the efficacy of itraconazole monotherapy vs. Exacerbations occurred less incessantly during the energetic treatment phase compared to placebo durations. While combination remedy with itraconazole is recommended if sluggish or poor response to corticosteroids, relapse, corticosteroid-dependent, or corticosteroid toxicity. Follow up and monitoring: Patients on treatment should initially be followed every 6�8 weeks with serum IgE ranges, chest radiograph, and lung operate take a look at [1]. Ideally, these individuals must be identified early in the course of the illness to mitigate or even stop the progressive bronchial harm that will lead to central bronchiectasis. Thus, the first step in analysis is documenting sensitivity to Aspergillus with both immediate cutaneous hypersensitivity or elevated IgE levels towards A. Response to therapy is associated with 25%�50% decline (but not normalization) of total IgE levels along with clinical and radiologic enchancment. Aspergillus hypersensitivity and allergic bronchopulmonary aspergillosis in sufferers with bronchial bronchial asthma: Systematic evaluation and meta-analysis. Global burden of allergic bronchopulmonary aspergillosis with asthma and its complication chronic pulmonary aspergillosis in adults. Prevalence of Aspergillus sensitization and allergic bronchopulmonary aspergillosis in cystic fibrosis: Systematic evaluate and meta-analysis. Allergic bronchopulmonary aspergillosis in cystic fibrosis: Reported prevalence, regional distribution, and patient traits. Scientific Advisory Group, Investigators, and Coordinators of the Epidemiologic Study of Cystic Fibrosis. Sensitization to Aspergillus species in the congenital neutrophil issues persistent granulomatous illness and hyper-IgE syndrome. Central airways obstruction as a outcome of Aspergillus fumigatus after lung transplantation. Influence of interleukin-10 on Aspergillus fumigatus infection in sufferers with cystic fibrosis. Mannosebinding lectin genotype and serum ranges in patients with continual and allergic pulmonary aspergillosis. Polymorphisms in toll-like receptor genes and susceptibility to pulmonary aspergillosis. Allergic bronchopulmonary aspergillosis in cystic fibrosis-State of the art: Cystic Fibrosis Foundation Consensus Conference. Selective protection against conidia by mononuclear and mycelia by polymorphonuclear phagocytes in resistance References 487 26. Prevention of corticosteroid-induced suppression of human polymorphonuclear leukocyte-induced harm of Aspergillus fumigatus hyphae by granulocyte colony-stimulating issue and gamma interferon. Purification and characterization of an elastinolytic metalloprotease from Aspergillus fumigatus and immunoelectron microscopic evidence of secretion of this enzyme by the fungus invading the murine lung. Virulence of an aspergillopepsin-deficient mutant of Aspergillus fumigatus and evidence for another aspartic proteinase linked to the fungal cell wall. Selective expression of a serious allergen and cytotoxin, Asp f I, in Aspergillus fumigatus. Evidence of a number of extracellular phospholipase activities of Aspergillus fumigatus. Exacerbation of invasive aspergillosis by the immunosuppressive fungal metabolite, gliotoxin. Allergens as proteases: An Aspergillus fumigatus proteinase directly induces human epithelial cell detachment.