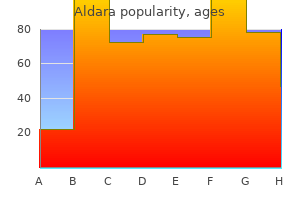
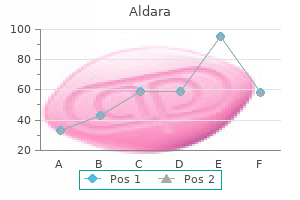
Aldara
Aldara dosages: 5 percent
Aldara packs: 1 creams, 2 creams, 3 creams, 4 creams, 5 creams, 6 creams, 7 creams, 8 creams, 9 creams, 10 creams
Buy aldara 5 percent on-line
To accomplish this acne 1st trimester order aldara 5 percent on-line, the clinician must be cognizant of basic podiatric conditions acne pistol boots aldara 5 percent otc, including painful lesions over bony prominences, heel ache, foot infections, and ache on the plantar surface of the foot. Footpad Use Footpads redistribute strain over an inflamed, tender area of the foot. Commercially out there aperture footpads are recommended for the temporary reduction of warts, corns, hyperkeratoses, and bunions. Verruca virus introduced into the plantar surface of the foot could produce a painful hyperkeratotic lesion, generally referred to as a plantar wart, on the sole of the foot. A simple callus may be painful and outcome within the formation of a "onerous corn" when formed over the bony prominence of a digit. When tenderness is elicited over a couple of metatarsal head, the analysis is metatarsalgia. A pad positioned beneath the first metatarsal head to raise the second and third metatarsals could provide some relief. A bunion develops when unbalanced forces applied to the primary metatarsal trigger lateral displacement of the distal end of the hallux. The affected person could complain of numbness over the distal, medial side of the first toe because of compression of the terminal branch of the medial dorsal cutaneous nerve. It is believed to characterize an overuse syndrome in an athletically active baby with tenderness within the posterior heel area. The middle hole is placed over the lesion and the encircling pad absorbs the friction. The hole within the pad is placed over the bunion and the surrounding pad absorbs the friction. Pain at the insertion of the Achilles tendon is worsened with extended standing or strolling and is aggravated by passive or active vary of movement in both circumstances. Directed palpation can distinguish one entity from the other, however both are treated similarly. Tenderness of the Achilles tendon suggests tendinopathy, whereas tenderness between the tendon and the calcaneus suggests retrocalcaneal bursitis. Importantly, Achilles tendinopathy has been noted to develop spontaneously after the usage of quinolone antibiotics, often with rupture. The situation may occur throughout quinolone use or a few weeks after therapy and prompts immediate discontinuation of use of the drug if acknowledged. Plantar fasciitis is usually unilateral and found in girls who put on high-heeled footwear. The pain is maximally severe within the morning or after prolonged sitting and improves after strolling, usually referred to as first-step ache. Some sufferers with plantar fasciitis may have a calcaneal heel spur, however the presence or absence of this radiographic discovering is clinically irrelevant. Frequently, this annoying condition resolves spontaneously, however decision is gradual, with as long as 6 to 18 months needed. Corticosteroid injection is utilized by some clinicians; however, its benefit remains unproved. Repeated injections of corticosteroids ought to be averted and have been related to rupture of the plantar fascia and fats pad atrophy. The neuroma forms after chronic irritation to the digital sensory nerve between the metatarsals. Patients report the sensation of a lump or cord within the interspace and describe paresthesia or numbness in the third or fourth toes. The origin is the medial tubercle of the calcaneus, which is the most common website of pain. A heel spur could additionally be seen on radiographs, however inflammation of the plantar fascia, not the spur, is the supply of the ache. B, Palpation of the tubercle of the calcaneus reproduces the pain of plantar fasciitis. D, Rolling the arch of the foot forwards and backwards over a frozen water bottle will stretch the fascia and, over time, could lessen the ache of plantar fasciitis. A small amount of gel substance was aspirated with a needle, however a cyst of this size is greatest completely excised surgically. Painful ganglion cysts are handled by aspiration, with or with out injection of a corticosteroid (see Chapter 52). After local or regional anesthesia (see Chapters 29 and 31), insert a 20-gauge needle into the cyst and withdraw yellow, thick, synovial fluid. Corticosteroid injection is commonly advocated for ganglion cysts, but recurrence is common after aspiration and corticosteroid injection, as high as 57% in a single study. As with some other fracture, pay consideration to the potential for disrupted joint cartilage, hypermobility of the fracture segments, and malposition or malunion of the fracture fragments. In the acute setting, a non�weight-bearing ankle splint that extends past the great toe supplies safety till the patient with an advanced fracture of the great toe obtains follow-up with a foot and ankle surgeon. Open fractures require careful cleansing, often antibiotic therapy, and shut follow-up. Fractures of the lesser toes usually end result from jamming the toe into a nightstand or bedpost when barefoot. After the fracture is lowered, splint the injured toe towards an adjoining noninjured toe. Place a soft corn pad or other suitable materials between the toes to prevent skin maceration, and hold the toes along with adhesive tape or a self-adherent wrap corresponding to Coban (3M Company, St. Demonstrate the procedure to the patient or household and dispense or prescribe sufficient materials in order that the splint may be changed every 2 to three days at house. A postoperative shoe (or similar footwear) may be a cushty alternative for the primary a quantity of days. Three particular injuries-toe fractures, sesamoid-bone fractures, and puncture wounds to the plantar floor of the foot-are mentioned in detail right here. A, Displaced fractures of the lesser toes (arrow) are sometimes a result of jamming the foot right into a bedpost or nightstand when barefoot and are simply reduced with in-line traction. After discount of the misalignment by in-line traction, generally the one remedy required is a postoperative shoe and taping in place for 4 to 6 weeks. Each bone lies throughout the tendon of its respective flexor hallucis brevis muscle stomach. Comparison radiographs make clear whether the radiographic abnormality represents a fracture. For a tibial sesamoid injury, an aperture bunion-type pad, bolstered medially with zero. Subsequent radiographs not often present bony consolidation, but the fracture interface appears smoother. B, Bunion shields can be used to redistribute strain away from fractured sesamoid bones. The hole within the pad is positioned over the fracture and the encompassing pad absorbs the pressure. A B in the plantar surface of the foot, and no universally accepted commonplace of care exists. Treatment recommendations range from easy cleaning of the wound to aggressive d�bridement.
5 percent aldara with visa
To carry out the lift-and-slide acne webmd order aldara 5 percent with mastercard, rescuers line up opposite one another on each side of the patient acne after stopping birth control aldara 5 percent order amex, ideally with a minimum of two rescuers per facet. In some circumstances, such as in environments with restricted house, standing over the patient and lifting straight upward could additionally be required. In addition to the usual thoracic, pelvic, and decrease extremity straps, use of an abdominal strap might scale back lateral movement without compromising respiration. If essential, padding ought to be positioned underneath the occiput to preserve the head in the neutral place. Most taping methods involve the use of one piece across the forehead and one piece throughout the c-collar. Placing straps across the top and neck might cause hyperextension or axial stretching of the neck. Standing Position Traditionally, standing sufferers have been positioned on a backboard by positioning the board behind the affected person, stabilizing the top, and decreasing the affected person and the backboard backward till the patient was mendacity on it. Current suggestions are to apply a c-collar and allow ambulatory sufferers to walk to the stretcher and help them into supine place on the mattress. Pediatric Patients little info is on the market on the correct choice and software of spinal immobilization devices for children. Half the whole growth in head circumference is achieved by the age of 18 months, giving kids a disproportionately giant head compared to the rest of the body. Before 8 years of age, these anatomic and developmental variations lead to a better incidence of upper cervical backbone accidents (C1�C2). Because accidents on this space are regularly unstable, correct cervical immobilization in the neutral place is critically essential. In the neutral position, the pediatric cervical backbone is normally lordotic or prolonged. The clinical significance of this is currently unclear, but theoretically it could be hazardous for young youngsters. As a rough guide, the exterior auditory meatus ought to be on the same level because the midpoint of the shoulder. If not modified, the standard backboard along side the disproportionately giant head of a kid could pressure the neck into hyperflexion and potentially worsen an underlying cervical backbone harm. Nypaver and Treloar66 confirmed that every one children required elevation of the again (mean height, 25. Children younger than 4 years required larger elevation than did those 4 years or older. Too large a collar generally ends in hyperextension, which might exacerbate a preexisting spinal harm. Underlying spinal abnormalities from conditions similar to ankylosing spondylitis, rheumatoid arthritis, or kyphosis can also contribute to exacerbation of injuries with c-collar utility. If the affected person permits handbook stabilization, this should be used in its place. Thoracolumbar Immobilization In common, problems are more likely to occur from failure to immobilize spinal accidents rather than from the process of immobilizationitself. Whencomplicationsdoarise,theymay be associated to improper choice or use of equipment or prolonged immobilization. Victims are usually strapped in place on a spine board to stop sliding throughout transport. If too few straps are used or if the straps are loosely applied, movement throughout transport can happen. Even when utilized correctly, spinal immobilization on a hard board may be extraordinarily uncomfortable for patients and should induce pressure-related tissue injury. In one study, 100% of healthy volunteers reported important pain after only half-hour on an extended backbone board. Other studies have demonstrated elevated tissue interface pressure in sufferers on backbone boards without air mattress padding. Excessive strapping can intervene with respiratory perform in each children73 and adults. Although this is most likely not an issue in healthy volunteers, the effects on patients with chest trauma or preexisting respiratory disease could additionally be significant. If vomiting does occur, logroll the affected person and board as a unit and suction the airway as wanted. Although this process could additionally be related to some spinal motion, airway safety takes precedence. Conclusion Although spinal immobilization has not been proven to decrease the probability of spinal injury and is related to a variety of problems, prehospital spinal immobilization stays commonplace. Nevertheless, recent proof supports a widespread shift to selective spinal immobilization by prehospital suppliers. Until these new recommendations turn out to be universal, emergency medication practitioners ought to know when spinal immobilization is indicated, acknowledge properly and improperly applied units, reduce pointless immobilization time, and work with prehospital suppliers to guarantee appropriate indications and correct use. In 1903 archaeologists from the Hearst expedition found two specimens whose open fractures had been treated with picket splints and bandages. Carefully utilized splints lower pain while minimizing further damage to muscular tissues, nerves, and blood vessels. Over the last 3 many years, prehospital splinting supplies, tools, and methods have evolved significantly. Indications and Contraindications Indications for splinting an extremity are often clear. Pain after trauma, with or without deformity, ought to arouse suspicion of underlying bone or joint harm. Other indicators include swelling, discoloration, deformity, crepitus, and lack of neurovascular operate. Thus, generally the place a musculoskeletal injury is suspected, a splint should be applied and maintained. However, within the setting of multisystem trauma with life-threatening accidents, speedy transport may be more important than extremity splinting. Equipment Various forms of splints are at present out there for immobilizing higher extremity injuries. Emergency care suppliers must be nicely trained and familiar with their equipment. Bent into any of three easy curves, this can be very robust and offers support for any fractured or injured extremity. These traits make it an ideal tool for emergency care providers and outdoor fanatics. As a outcome, vacuum splints normally are more comfortable than other inflexible splints.
Purchase aldara 5 percent amex
Motorcycle Helmet Removal For the reasons described earlier skin care specialist cheap aldara 5 percent line, bike helmets must be eliminated within the prehospital setting skin care magazines aldara 5 percent purchase line. Following division of the outer rigid shell, incise the internal foam materials and remove it whereas maintaining the head and neck in impartial alignment. Although this approach does provide an alternate technique of eradicating the helmet, the extraordinary vibrations produced throughout use of the cast cutter might exacerbate an underlying spinal harm. In addition, this technique could also be slow and troublesome with modern, well-fitting, high-quality helmets. In addition, the Championship Auto racing T eams and National Association for Stock Car Auto racing strongly advocate its use. Complications It is theorized that underlying cervical spine injuries could also be exacerbated by failure to adhere to correct helmet removing strategies, although clinical information is lacking. Conclusion Prehospital care suppliers should take warning when evaluating and treating an athlete with a suspected head and neck damage. When indicated, prehospital helmet elimination may be achieved in a safe and effective manner by well-trained prehospital care providers. The main concern of eradicating helmets and protective padding is causing additional damage to the patient. American Academy of Orthopaedic Surgeons, Committee on Injuries: Fractures and dislocations of the backbone. In Emergency care and transportation of the sick and injured, Chicago, 1971, American Academy of Orthopaedic Surgeons, p 111. Hauswald M, Ong G, Tandberg D, et al: Out-of-hospital spinal immobilization: its impact on neurologic harm. Chan D, Goldberg r, Tascone A, et al: the impact of spinal immobilization on healthy volunteers. Hauswald M, Hsu M, Stockoff C: Maximizing comfort and minimizing ischemia: a comparability of 4 strategies of spinal immobilization. Stroh G, Braude D: Can an out-of-hospital cervical backbone clearance protocol identify all sufferers with injuries National Spinal Cord Injury Statistical Center: Spinal cord damage details andfiguresataglance,2015. Podolsky S, Baraff lJ, Simon rr, et al: Efficacy of cervical spine immobilization methods. National Association of Emergency Medical Technicians, American College of Surgeons, Committee on Trauma: Pre-hospital trauma life help, St. Ben-Galim P, Dreiangel N, Mattox kl, et al: Extrication collars can lead to irregular separation between vertebrae in the presence of a dissociative harm. Markenson D, Foltin G, Tunik M, et al: the kendrick Extrication Device used for pediatric spinal immobilization. Geeraerts T, Chhor V, Cheisson G, et al: Clinical evaluation: preliminary administration of blunt pelvic trauma sufferers with haemodynamic instability. Vermeulen B, Peter r, Hoffmeyer P, et al: Pre-hospital stabilization of pelvic dislocations: a brand new strap belt to present temporary hemodynamic stabilization. American College of Surgeons Committee on Trauma: Advanced trauma life help for doctors, ed 7, Chicago, 2004, American College of Surgeons. Veenema k, Greenwald r, karnali M, et al: the initial lateral cervical spine film for the athlete with a suspected neck harm: helmet and shoulder pads on or off Hunt k, Hallworth S, Smith M: the results of rigid collar placement on intracranial and cerebral perfusion pressure. Bauer D, kowalsk r: Effect of spinal immobilization on pulmonary operate in healthy, non-smoking men. Christensen kS, Trautner S, Stockel M, et al: Inflatable splints: do they trigger tissue ischemia International Trauma life Support: Utilization of traction splints with open femur fractures. Almquist Jl: Spine injury management: a comprehensive plan for managing the cervical spine�injured football participant. The peak incidence of traumatic amputations happens between the ages of 15 and 40 years and approximately 80% of injuries happen in males. Motor vehicle collisions are the main mechanism of injury, adopted by industrial and agricultural accidents. Local crush accidents happen most commonly, and sharp guillotine amputations are least frequent. Seventy % of amputations overall happen within the upper extremity and distal amputations are more frequent than proximal. This articleisdiscussestothecare of a andmanagement amputated physique part essential the salvage preservation of emergency Successful revascularization of amputated components might ensure viability, but neurologic, osseous, and tendinous healing are critical for ultimate operate. Rehabilitation from replantation surgery could additionally be prolonged, (often >1 year) and frequently repeat surgical procedures are required. The first profitable microvascular anastomosis of a digital vessel was described in 1965, and now replantation success rates vary from 50% to 90%. With advancements in technology, there are additionally options to replantation similar to targeted reinnervation, transplantation of composite tissue, or the potential for upper extremity transplantation to restore higher extremity function. Replantation is more prone to happen with sharp/penetrating injury, distal degree of amputation, lack of multilevel involvement, and when the harm is isolated to the extremity. Ultimately, the microsurgical group and affected person should reach the decision together after a rational rationalization of the potential outcomes. Replantation is more commonly carried out for upper extremity amputation as a end result of a lower extremity prosthesis typically supplies an excellent useful outcome and is commonly superior to outcomes with replantation. Upper extremity prostheses are less able to obtain nice motor activity and a "bad hand" could also be more practical than a "good amputation" within the higher extremity. The thumb accounts for 40% to 50% of hand perform with its utility in pinch and grip. The decision to replant is made on a case-by-case foundation by the microsurgical team, who should weigh all the components concerned. In basic, sufferers can count on to obtain 50% of unique sensation and motor function of the replanted half, with youthful sufferers and extra distal amputations having one of the best outcomes. For instance, an amputated fingertip not suitable for replantation may be a perfect donor source for a skin graft on the stump. In common, never discard amputated tissue till all potential uses of the severed elements are thought of. Guillotine-type injuries are the least common but have the best prognosis due to the limited space of destruction. Crush accidents are the most typical, but produce extra tissue injury and therefore have a poorer prognosis. Avulsion accidents have the worst prognosis as a result of a big amount of vascular, nerve, tendon, and gentle tissue damage invariably happens. If unsuccessful, the judicious use of a tourniquet is endorsed as a quick lived adjunct to management extremity hemorrhage. In partial amputations, observe the exhausting and delicate indicators of vascular harm (Table 47.
Aldara 5 percent trusted
Erroneous needle placement also can produce problems similar to pneumothorax during a brachial plexus or intercostal block skin care home remedies 5 percent aldara otc. Use of Epinephrine With Local Anesthetics Epinephrine along side local anesthetics prolongs the length of anesthesia and produces a temporary hemostatic effect skin care steps proven aldara 5 percent, but its inclusion in digital block options has historically been discouraged due to the idea that it can lead to ischemia and necrosis. Although tissue ischemia and sloughing have been reported with concentrations of 1: 20,000, current practice entails concentrations within the vary of 1: 100,000 to 1: 200,000 and the utilization of submaximal doses. Several authors recommend that epinephrine-containing solutions can be safely injected into the fingers without opposed sequelae. Current knowledge help using epinephrine, when appropriately applied, for the performance of digital blocks of the fingers and toes. The use of phentolamine, which produces postsynaptic -adrenergic blockade, is beneficial for clinically significant vasoconstrictor-induced tissue ischemia. This treatment is often given by local infiltration, within the space the place epinephrine has been injected, at a dose of 0. If local infiltration is ineffective due to tension inside a tissue compartment or if the world of vasoconstriction is giant, give phentolamine by the intraarterial route. Patients can also demonstrate systemic reactions to hidden allergens that will mimic a systemic response, corresponding to anaphylactic reactions to the latex in surgical gloves. High Blood Levels Systemic toxic reactions end result from excessive blood ranges of native anesthetic. Several elements are necessary in producing excessive blood levels, together with the site and mode of administration, price of administration, dose and concentration, addition of epinephrine, specific drug, clearance, most secure dosage, and inadvertent intravascular injection. Dose and Concentration the larger the entire dose, the higher the height blood level. It is unsure whether or not rising the focus while maintaining the entire dose by lowering the volume impacts the serum degree. Addition of Epinephrine Epinephrine produces vasoconstriction and reduces systemic absorption, thereby leading to decrease peak blood ranges. Occasionally, the apprehension, tachycardia, or palpitations induced by epinephrine may be incorrectly interpreted by both the clinician and affected person as an "allergic" response. Site and Mode of Administration In evaluating the routes of administration for a given dose, the intravascular route produces the highest ranges, adopted by topical mucosal application after which infiltration. The extra vascular the positioning, the extra systemic absorption that occurs and the upper the level obtained. The following blocks are organized in lowering order of systemic absorption: intercostal, caudal, epidural, brachial plexus, and subcutaneous. It follows that the positioning of administration is a crucial variable in figuring out the secure dose of an anesthetic. For instance, 400 mg of lidocaine might produce a nontoxic blood stage with subcutaneous stomach wall infiltration however produce a toxic degree when used for an intercostal nerve block. Agents with excessive lipid solubility and decrease protein binding (etidocaine > bupivacaine > lidocaine > mepivacaine) tend to become sequestered in tissue and have slower absorption and lower blood ranges. Agents with a higher volume of distribution or quicker clearance (etidocaine > lidocaine > mepivacaine > bupivacaine) additionally produce decrease blood levels. Together, these results produce margins of safety for each anesthetic, with etidocaine having the best security margin, followed by bupivacaine, which is equal to or higher than lidocaine. Esters are tough to measure in blood due to their rapid hydrolysis by pseudocholinesterase. The liver metabolizes amides, with the clearance fee being a operate of hepatic blood move and the extraction capability of the liver. Decreased hepatic blood circulate, produced by norepinephrine, propranolol, or common anesthesia, slows clearance and potentially raises drug blood ranges. Decreased drug extraction, related to congestive coronary heart failure, cirrhosis, or hypothermia, could produce a higher blood stage. Decreased clearance of esters and an elevated danger for toxicity happen in sufferers with either low ranges or an atypical form of pseudocholinesterase. Low levels happen in numerous disease states, together with extreme liver disease and renal failure, and in being pregnant. Atypical pseudocholinesterase is an inherited trait, and its presence reduces the hydrolysis fee of procaine to a greater extent than low levels do. There are significant differences between pediatric and adult drug distribution and metabolism. Neonates exhibit each decreased levels of pseudocholinesterase and lowered hepatic metabolism, thus rising the danger for toxicity. In older youngsters, the effects of increased hepatic metabolism and a relatively larger quantity of distribution improve their tolerance for larger doses. Because lidocaine is metabolized within the liver by cytochrome P-450 enzymes, medication that inhibit these enzymes could gradual lidocaine clearance and increase the danger for lidocaine toxicity. Although the effect of ciprofloxacin and erythromycin on infiltrated lidocaine has not been studied, these medication lower the metabolism of lidocaine and increase the focus of its major metabolites when lidocaine is injected intravenously. The maximum protected dose of a drug could additionally be outlined as the dose that produces a blood stage of the drug slightly below the toxic stage (Table 29. Furthermore, the dose must be modified according to the site and mode of administration. Maximum secure doses as said on bundle inserts ought to be used solely as tips because most of them are derived from animal experiments and are primarily based on absorption information only. Levels range with the site of administration, use of a vasoconstrictor, and to some extent, the well being of the affected person. To ascertain the power of an answer in milligrams per milliliter, think about the following: A 1% answer is ready by dissolving 1 g of drug in one hundred mL of answer. Note: To calculate the strength from the percentage quickly, simply move the decimal level one place to the right, as follows: 0. For instance: 1: 100,000 concentration of epinephrine = 1 g/100,000 mL = 1000 mg/100,000 mL = 1 mg /100 mL or 0. Drugs could additionally be toxic even throughout the "safe range" when inadvertently injected intravenously. Inadvertent Intravascular Injection Most toxic reactions are attributable to inadvertent intravascular injection of anesthetics whose doses were calculated for their intended extravascular sites. For instance, lidocaine, 300 mg, is a safely infiltrated dose that may probably trigger toxicity if directly injected into the bloodstream. Anesthetics which are injected intravascularly must move through the lungs earlier than they reach different organs. Intraarterial injections into subcutaneous end-arteries about the head or neck are capable of retrograde move into the cerebral circulation if the injection strain exceeds arterial pressure. Because the blood volume in the brain is simply roughly 30 mL at any given second, even 1 mg of lidocaine injected into the carotid artery can theoretically produce toxic concentrations. These brokers additionally gradual electrical conduction and lead to reentry phenomena and numerous supraventricular and probably deadly ventricular dysrhythmias, especially with bupivacaine and etidocaine. Prevention of Toxicity Knowledge of things contributing to toxicity guides preventive measures.
5 percent aldara discount mastercard
Patients might have weak spot of skin care brand names 5 percent aldara buy amex, or an lack of ability to extend acne jaw line trusted 5 percent aldara, the involved toe or toes. Repair is favored if the affected person has vital ache or any flexion deformity of the involved toe. Repair is also favored when both ends of the tendon are easily visualized within the wound and the affected person is prepared to undergo extended immobilization after restore. Superficial cutaneous nerves are simply injured on the dorsum of the foot throughout wound exploration, which might lead to the formation of a continual, painful neuroma. Splint the ankle at 90 degrees with the toes in the neutral position, and advocate non�weight bearing status until specialty follow-up. Anatomic and biomechanical issues, the physiology of flexor tendons and tendon healing, and follow-up rehabilitation and bodily therapy are complicated and formidable. A satisfactory consequence is harder to achieve with an injured flexor tendon than with a similar degree of damage to an extensor tendon. Unlike extensor tendons, flexor tendons are influenced by numerous complex pulley mechanisms. In addition, flexor tendon injuries are sometimes associated with nerve and vascular accidents. The main scientific mandates for emergency providers are to diagnose or think about flexor tendon injuries, present preliminary proper wound care, and expedite appropriate consultation and follow-up. Therefore a partial flexor tendon harm may be clinically silent until rupture occurs days or weeks later. Delayed repair of undiagnosed flexor tendons could additionally be difficult by tendon retraction or scar formation, and tendon switch and grafting may be needed. It will not be attainable on the initial go to for the emergency provider to diagnose the presence of all flexor tendon accidents, nor the total extent of such injuries. Even although session is suggested earlier than definitive disposition, the same limitations within the examination would equally confront a specialist. Notwithstanding the earlier discussion, complete flexor tendon accidents are often obvious on physical examination, both by testing individual tendons or by the resting posture of the injured hand. In contrast, partial tendon lacerations are commonly clinically unappreciated as a outcome of no useful deficit is evident. The emergency supplier could not be capable of arrive at a whole or correct diagnosis with out surgical exploration. A specialist, normally on an elective outpatient foundation, surgically repairs utterly transected flexor tendons. The ultimate end result of flexor tendon surgery is determined by multiple factors; however, surgical repair of most flexor tendons achieved inside 10 to 21 days of injury (delayed primary repair) generally produces final outcomes similar to those repaired instantly. It is acceptable to deal with partial flexor tendon lacerations, if appreciated, with cautious wound cleaning, pores and skin closure, splinting, and referral for reevaluation in 1 to 5 days. Some surgeons will repair all partial tendon lacerations, whereas others take a more conservative strategy. Although no definitive normal of care has been promulgated, many clinicians prescribe 3 to 5 days of antibiotics efficient in opposition to gram-positive organisms (including Staphylococcus aureus) if a tendon is injured. Antibiotics are recommended if the degree of contamination is important, cleaning has been delayed, there are uncommon sources of harm, or the affected person is immunocompromised. Initially considered a minor ankle sprain by both the patient and provider, the diagnosis was missed in more than 20% of cases in a 2008 case collection. A, the depth of this wound precludes extensive exploration to visualize the tendon. Clues to a partial flexor tendon laceration embrace weak spot of flexion or ache with attempts at flexion in opposition to resistance, but many partial lacerations are clinically silent. The prudent course would come with meticulous wound care, splinting, pores and skin closure, and get in contact with with a hand specialist to organize reexamination in a couple of days, whereas cautioning the patient that a flexor tendon injury may be current and delayed restore for as much as 1 to 3 weeks yields results comparable to immediate repair. C, When examined with the fingers in extension, the tendon was readily visualized, a surprise to the clinician given the benign and superficial look of the laceration. D, However, when the fingers had been flexed (arrow), the place of the hand when the damage occurred, a 20% to 30% laceration of the tendon was demonstrated. Fluoroquinolone antibiotics have been implicated in Achilles tendon rupture, particularly within the elderly. This led the Food and Drug Administration to problem a "black box" warning on the use of all fluoroquinolones for this situation in 2008. Pain will not be perceived within the tendon itself; instead, heel or diffuse ankle pain could additionally be skilled. With his hand at rest, his index finger lies in extension, in contrast to his other fingers, that are partially flexed. B, Loss of the digital cascade within the center finger illustrated here ought to be indicative of a flexor tendon laceration without further examination. The small glass laceration in the palm accounts for the profundus laceration, obvious only at follow-up. Splinting and follow-up in a number of days are prudent based mostly on the harm mechanism and site. C, the flexor digitorum profundus tendon is examined by immobilizing the digit in query and asking the patient to flex the distal interphalangeal joint against resistance. D, the flexor digitorum superficialis tendon is examined by immobilizing the digits not being tested and asking the affected person to flex the proximal interphalangeal joint towards resistance. Pain and weak point associated with flexion in opposition to resistance might counsel a partial tendon laceration, but that is often a really subtle or inaccurate analysis that should be repeated when the pain and swelling have subsided. Point-of-care ultrasound has emerged as a useful gizmo to diagnose both full and partial tendon ruptures. The sensitivity and specificity of ultrasound for Achilles tendon rupture, as reported in the radiology literature, are 96% to 100% and 83% to 100%, respectively. A defect in the Achilles tendon could additionally be appreciated in some instances of Achilles tendon rupture, but not on this case. The Achilles tendon is assessed, proximally to distally, for synchronous movement, using dynamic sonography during passive dorsiflexion and plantar flexion of the ankle with the probe over the world of curiosity. Splinting the foot in mild plantar flexion (gravity equinus) can shield the tendon till follow-up in 1 to 5 days. Both the quadriceps and patellar tendons are subject to rupture, and the situation happens predominantly in males. Quadriceps tendon rupture is more common in the elderly and in these with systemic degenerative disease, arthritis, and steroid use, and is associated with important morbidity no matter remedy. It may also be seen in younger sufferers, such as after taking a basketball leap shot. Patellar tendon rupture can be a critical damage but happens extra commonly in healthy patients, youthful than forty years, collaborating in sporting events. The trauma may be seemingly minor, similar to lacking a step or jumping from a low peak. An obvious suprapatellar delicate tissue defect and an incapability to carry out a straight-leg elevate while supine made the analysis of a complete quadriceps tendon rupture obvious. Diffuse delicate tissue swelling, bilateral knee effusions, normal radiographic findings, and the ability to stroll with bilateral knee immobilizers delayed the diagnosis of bilateral quadriceps tendon rupture till follow-up.
Syndromes
- Delirium
- A measurement called standard deviation (SD) is used to compare the height of different children.
- Loss of appetite
- Hematoma (blood accumulating under the skin)
- Burns and blisters where the acid contacted the skin
- Wearing protective clothing
- Tube through the mouth into the stomach to wash out the stomach (gastric lavage)
- Measles - mumps - rubella (MMR)
- Blood chemistry
5 percent aldara generic
This method prevents the scissors from slicing the knot itself and leaves a 3-mm tail acne 24 cheap 5 percent aldara with visa, which protects the knot from unraveling acne treatment aldara 5 percent discount on line. The index finger is placed on the side of the needle holder, where it guides placement of the needle. Pull the suture across the wound to determine the right degree of dermal entry on the other aspect. Pass the needle downward through the dermis on the other side in order that it exits at the bottom of the wound. B Start right here If the wound has been undermined, the needle enters at the base of the flap and is passed upward by way of the dermis. C Pull the two tails of the suture in the identical direction alongside the axis of the wound to appose the wound edges, and then tie the knot. Subcutaneous knots are "buried" at the bottom of the wound to prevent painful nodules beneath the dermis and to keep the majority of the foreign materials away from the pores and skin surface. Surface Closure the dermis and the superficial layer of dermis are sutured in a single layer with nonabsorbable synthetic suture. If the edges of the wound are apposed after closure of the deeper layers, small 5-0 or 6-0 sutures can be used merely to match the epithelium on all sides. Wounds with greater pressure and separation should have pores and skin stitches placed closer to one another and closer to the edge of the wound with consideration for an interrupted vertical mattress suture; layered closure is essential in such wounds. When suturing the skin, right-handed operators should move the needle from the right side of the wound to the left. Once the needle exits the pores and skin on the other aspect of the wound, regrasp it with the needle holder and advance it by way of the tissue; care must be taken to avoid crushing the point of the needle with the instrument. Forceps can stabilize the needle by holding it within the tissue through which the needle has simply handed. If the purpose of the needle turns into boring earlier than all the connected thread has been used, the suture must be discarded. Complications Sutures act as international bodies in a wound, and any stitch may damage a blood vessel or strangulate tissue. Therefore, the clinician should use the smallest measurement and the least variety of sutures that can adequately shut the wound. Drive the needle tip downward and away from the reduce edge into the subcutaneous layer. The needle tip is directed towards the opposite side at the similar stage by rolling the needle holder. This methodology incorporates extra tissue within the sew within the deeper layers of the wound than on the surface. As another, if a small needle is used in thick pores and skin or the space throughout the wound is nice, the needle may be removed from the primary aspect, remounted on the needle holder, and superior to the opposite aspect. The distance from each exit of the suture to the laceration is half the depth of the dermis. C, Correct number of stitches used for a wound under a mean quantity of tension. Rotate the wrist (pronate) so that the needle enters the skin perpendicularly, not at an angle, because the wrist supinates. If sutures are tied too tightly across the edges of the wound or if particular person stitches are underneath excessive pressure, blood supply to the wound may be compromised, thereby rising the prospect of infection. If the perimeters of a wound invert or if one edge rolls under the opposite aspect, a poorly formed, deep, noticeable scar will end result. Excessive eversion that exposes the dermis on each side may even end in a bigger scar than if the perimeters of the skin are perfectly apposed, but inversion produces a more seen scar than eversion does. Wounds over cell surfaces, such as the extensor surfaces of joints, ought to be everted. In other words, the stitch is wider at its deepest part and narrower on the surface. A continuous sew is an effective technique for closing relatively clear, low-risk wounds which are underneath little or no tension and are on flat, immobile pores and skin surfaces. In a continuous, or "running," sew, the loops are the uncovered portions of a helical coil tied at each finish of the wound. A continuous suture line may be positioned more quickly than a collection of interrupted stitches. A continuous stitch has the extra advantages of strength (with pressure being evenly distributed alongside its whole length), fewer knots (which are the weak factors of stitches), and more effective hemostasis. Likewise, if infection develops and the incision should be opened at one level, chopping a single loop could enable the complete wound to fall open. A easy steady stitch has a tendency to produce suture marks if used for the closure of large wounds and if left in place for greater than 5 days. Place an interrupted stitch at one end of the wound and minimize solely the free tail of the suture. This approach allows the operator to see the needle path, thereby making certain that the correct depth has been reached, and promotes eversion of the pores and skin edges. B, "Tacking" type of vertical mattress suture extending into the deep fascia to obliterate lifeless house under the wound. The suture enters the bottom of the flap, is introduced up into the dermis, and exits simply proximal to the wound edge along the bottom of the flap to be tied and reduce. After each passage of the needle, tighten the loop slightly, and maintain the thread taut in your nondominant hand. Place the last loop just past the tip of the wound and tie the suture, using the last loop as a tail to tie the knot. The interlocking method allows use of the continuous sew alongside an irregular laceration. On event, wounds require an extended interval of assist, longer than that offered by floor stitches. Some sufferers with wounds that require pores and skin closure are unlikely or unwilling to return for elimination of the sutures. On occasion, the patient (child or adult) is prone to be as frightened by and uncooperative with suture removal as they were for suture placement. Surface sutures are more probably to produce stitch marks in kids because the wounds are beneath greater rigidity than those in adults. The continuous subcuticular (or dermal) suture approach is right for these conditions; the wound can be closed with an absorbable subcuticular sew, thereby obviating the need for later suture elimination. In sufferers vulnerable to keloid formation, the subcuticular approach can be utilized in lieu of surface stitches to keep away from disfiguring stitch marks. The subcuticular stitch requires a 4-0 or 5-0 suture made of both absorbable materials or nonabsorbable artificial monofilament. An absorbable suture may be buried throughout the wound, whereas a nonabsorbable suture is used for a "pullout" sew. It passes by way of tissues as simply as nonabsorbable monofilament sutures do and is absorbed if left within the wound. Start the pullout subcuticular sew at the pores and skin floor approximately 1 to 2 cm away from one finish of the wound. Take bites through tissue in a horizontal direction, with the needle penetrating the dermis 1 to 2 mm from the skin floor.
Aldara 5 percent purchase with visa
The runners acne youtube 5 percent aldara overnight delivery, nevertheless acne en la espalda aldara 5 percent purchase with visa, might make it tougher to slide a affected person onto the board. Advantages of backboards over full-body splints embody their ease of storage, low price, and excessive versatility. The backboard can be used to slide a victim out of an automobile or to defend a victim during removing of a windshield. Studies have demonstrated that spinal immobilization on a tough backboard causes head, back, and jaw pain. This idea was reaffirmed by Hauswald and colleagues,51 who found that growing the amount of padding on a backboard decreases the amount of ischemic pain attributable to immobilization. In some circumstances, tissue ischemia can result in frank stress ulcers, notably within the aged or nutritional poor populations. This cervical extrication splint resembles a kendrick Extrication Device however is more rugged and sturdy. In addition to offering spinal immobilization, it additionally acts as a harness that can be utilized for hauling sufferers over flat surfaces and for vertical lifts. In reality, one examine found that utilizing the inside track stretcher triggered less spinal motion than did a traditional long backboard and logroll method. It is comfortable, rigid, and adaptable to sufferers of assorted lengths and offers unobstructed radiographic transparency of the whole backbone. If necessary, it can be utilized almost immediately or removed with out disturbing the place of the victim. When cervical movement restriction is desired, a c-collar can be used with the news stretcher. One limitation of the inside track stretcher is the potential for trapping clothes, skin, or different objects between interlocking parts. It also interferes slightly with the ischial section of a half-ring traction splint, but works well with Sager-type devices. Full-Body Splints A number of full-body splints can be found and could also be used by some prehospital suppliers. This full-body splint has a detachable head harness and a thoracic harness, in addition to pelvic and lower extremity belts. The space between the lower extremities facilitates wrapping with bandage material in the occasion of fractures. Another full-body splint designed to reduce the pain associated with most of the immobilization units described beforehand is the vacuum mattress splint. It can even assist help an injured extremity or impaled object or allow an obese or kyphotic affected person to lie supine on a long backboard. A, the HeadBed, a cervical immobilization gadget manufactured from a waterproof corrugated board. Additionally, tightly securing the top to any device with out equally securing the physique has the potential to enhance forces on the cervical backbone during transportation and transfer. Because any manner of strapping is unlikely to completely forestall motion of the torso, the pinnacle ought to at all times have the flexibility to shift axially as a unit with the body. Lateral Neck Stabilizers Procedure Cervical Spinal Motion Restriction the primary priority in cervical spinal movement restriction is maintaining the pinnacle and backbone within the neutral position. If patients are capable of cooperate, instruct them to hold their head and neck within the neutral place and remain nonetheless. Once the cervical spine has been manually stabilized, examine the neck for swelling, ecchymosis, deformity, bony tenderness, or penetrating wounds. Once the collar is in place, caution aware patients towards motion of the pinnacle. Investigate any persistent complaints light-weight objects similar to blocks (10 � 10 � 15 cm) manufactured from medium-density foam rubber are commonly used to provide further lateral stabilization of the pinnacle and neck. The Universal Head Immobilizer is made from a Herculite nylon and a polyethylene foam platform that fastens to the stretcher with Velcro straps. The lateral pillows are then attached to the nylon platform via large Velcro interfaces. Backboards can be modified by an occiput cutout (B) or a double mattress pad (C) to increase the chest, the precise scientific penalties of which are unknown. For extremely quick necks, a particular c-collar such because the No-Neck (laerdal Medical Corporation) is recommended. Cervical Collar Application A 1 Posterior-First Method 2 3 While one supplier applies in-line stabilization (not traction! Maintain in-line stabilization within the neutral place until the patient is totally immobilized. Attach the loop Velcro from the posterior portion of the collar to the hook Velcro on the anterior portion. Patients with extraordinarily lengthy necks or especially brief ones may be immobilized via a horse collar fashioned from a blanket or towel. Sitting Position To immobilize sufferers who require extrication and are found in a sitting position, providers can use a brief backboard or commercially obtainable cervical extrication device. At least two rescuers ought to be current to apply an extrication splint to a sitting affected person. If essential, fastidiously rock the affected person forward a couple of degrees to facilitate placement of the splint. It can be a good suggestion to pad the groin area when inserting the pelvic help straps as a result of these straps might cause the patient appreciable discomfort. This process could have to be modified for sure accidents and preexisting conditions. For instance, patients with pelvic fractures might not tolerate placement of the pelvic help and bottom straps, and the gravid stomach of a pregnant patient may stop placement of the center strap. It may be essential to place padding behind the top to keep a impartial place. Use the forehead as a degree of engagement for one strap and the c-collar for the opposite. The patient must be rotated and laid in a supine position onto a backboard or cot as wanted. The legs can then be prolonged and secured or left within the flexed place with a pillow placed beneath the knees for assist. If wanted, apply a lateral immobilizer to help stop motion of the top and neck and secure the physique with straps. Once the patient is on the stretcher, the thoracic straps might must be readjusted. The device must be eliminated as soon as potential, with care to keep away from unnecessary movement of the backbone till important injuries are ruled out. Physical examination, spinal immobilization, airway administration, and transport are easier to accomplish with the patient in the supine position.
Buy discount aldara 5 percent online
Anesthetize a localized space of the tongue topically by masking the realm with 4% lidocaine-soaked gauze for 5 minutes skin care questionnaire 5 percent aldara safe. Determine the maximum protected dose of local anesthetic and avoid exposure to larger doses skin care news buy cheap aldara 5 percent line. Large lacerations require infiltration anesthesia (1% lidocaine with buffered epinephrine) or a lingual nerve block. If the tip of the tongue has been anesthetized, a towel clip or suture can be utilized to keep protrusion of the tongue in an uncooperative affected person. Further anesthesia and subsequent wound cleaning and closure are possible while an assistant applies light traction on the tongue. Blood vessels within the fascia are the most important source of the bleeding in scalp lacerations. Scalp Lacerations the scalp extends from the supraorbital ridges anteriorly to the external occipital protuberances posteriorly and blends with the temporalis fascia laterally. The outer layer consists of the pores and skin, superficial fascia, and galea (the aponeurosis of the frontalis and occipitalis muscles), which are firmly adherent and surgically considered as one layer. The integrity of the outer layer is maintained by inelastic, robust, fibrous septa, which maintain wounds from gaping open unless all three portions have been traversed. The galea itself is loosely adherent to the periosteum by means of the slack areolar tissue of the subaponeurotic layer. Stellate lacerations are common on this area, not only because the scalp is vulnerable to blunt trauma but additionally because its superficial fascial layer is inelastic and firmly adherent to the pores and skin. Stellate lacerations pose additional technical issues in closure and have a greater propensity for infection. Debris and other contaminants could be deposited a number of centimeters from the visible laceration; therefore, careful exploration plus cleaning of scalp wounds is necessary. When scalp wounds are d�brided, obviously devitalized tissue ought to be eliminated, but d�bridement should be conservative because closure of large defects on the scalp is difficult. The presence of a rich vascular community within the superficial fascia results in profuse bleeding from scalp wounds. The subgaleal layer of free connective tissue incorporates emissary veins that drain through diploic vessels of the skull into the venous sinuses of the cranial hemispheres. In scalp wounds that penetrate this layer, micro organism could additionally be carried by these vessels to the meninges and the intracranial sinuses. Thus, a scalp wound infection can result in osteomyelitis, meningitis, or a mind abscess. Profuse bleeding, especially from extensive scalp lacerations, is greatest managed by suturing130 (see additionally Chapter 34). Ask an assistant to keep compression across the wound whilst you full closure of the wound. A easy procedure that often provides hemostasis of scalp wounds is to place a wide, tight rubber band or Penrose drain around the scalp from the brow to the occiput. The disadvantage of this system is that tissue grasped by the hemostat could additionally be crushed and devitalized. If bleeding from the sting of the scalp wound is vigorous and definitive repair must be postponed whereas the patient is resuscitated, Raney scalp clips or a hemostat can be utilized quickly to the edge of the scalp wound to control the hemorrhage. However, a typical error is to mistake a tear within the galea or the periosteum for a fracture during palpation inside the wound. Of particular importance are stab or puncture wounds in the scalp and brow, corresponding to from a nail, spike, screwdriver, knife, or ice pick. Without a laceration to discover, such wounds may seem benign, and the affected person can initially seem comparatively asymptomatic, but the skull or brain has been penetrated. When evaluating a puncture or stab wound to the top, a computed tomography scan could provide unexpected findings of a cranium fracture, linear or depressed, or an underlying brain damage or early hemorrhage. B, Puncture wounds in the brow and scalp from such objects as a knife, nail, screwdriver, or ice pick can penetrate the cranium and mind, and initially the patient seems properly and the wound appears benign. As stated in different sections, avoid shaving, and as a substitute clip hair to keep away from additional damage. Because of the in depth collateral blood provide of the scalp, most lacerations in this space heal without drawback, even after delayed therapy. Nonetheless, wound cleaning must be adequate to avoid the devastating complication of scalp infection. With microvascular methods, massive sections of skin avulsed from the scalp could be reimplanted. Some of these similar methods are used to salvage avulsed scalp, similar to those used for amputated extremities. Separate closure of the galea introduces further suture materials into the wound and may improve the danger for an infection. However, in extremely massive wounds, separate closure may be necessary to provide a more secure approximation of the galea than can be obtained with a large-needle, single-layer closure. In this case, an inverted sew (with an absorbable 3-0 or 4-0 suture) will bury the knot beneath the galea. Avoid smaller suture material as a end result of it tends to break when agency knots are being tied. Leave the ends of the tied scalp sutures a minimum of 2 cm lengthy to facilitate subsequent removal. Absorbable sutures may provide comparable cosmetic and functional outcomes in scalp laceration restore. Place gauze sponges over the laceration to present direct native pressure beneath the elastic bandage. Advantages of this technique embody cosmetic results much like suturing, increased velocity of restore, no need for clipping of hair, and no need for return go to for suture or staple removal. To shut a scalp laceration that extends through the galea, use an extended needle, forceps, and 3-0 sutures (blue polypropelene sutures make removing easier). The affected person ought to be informed that the glue will steadily fall off within two weeks. If the drop of glue fails to fall off, it might be merely removed with tweezers or comb. Some nail mattress lacerations are minor and of no consequence, whereas others portend a poor consequence until the mattress is repaired. Suture the nail bed if a large subungual hematoma is associated with an unstable or avulsed nail. A good consequence is determined by sustaining the area beneath the eponychium (cuticle) because the laceration heals and the brand new nail grows out, which is a slow process. Prohibiting bathing with sutures in place in any a part of the physique has no scientific advantage. Partial Nail Avulsions If the nail is partly avulsed (especially on the base) or free, lift the nail to assess and potentially repair the nail mattress. Repeat, each 1�2 cm alongside the wound, bisecting the wound just as if using sutures. B, from Karaduman S, Yurukrumen A, Guryay S, et al: Modified hair apposition approach as the primary closure methodology for scalp lacerations, Am J Emerg Med 27:1050, 2009.
5 percent aldara order amex
It is a water miscible lotion acne jensen boots aldara 5 percent purchase otc, distributed as a sealed pack containing a single-use pad acne pustules 5 percent aldara generic overnight delivery. This product has been shown to neutralize many chemical warfare brokers and toxic industrial chemicals. Neutralizing products have been shown to be superior to traditional decontamination methods in head-to-head trials. Transfer patients with main or reasonable injuries to areas designated for such circumstances. Send sufferers with minor or no accidents to applicable holding areas for further evaluation. Medical care at this stage is determined by the toxin to which the patient has been uncovered and the potential toxicity of that agent. Wounds, after copious irrigation, may need thorough exploration and presumably surgical removal of the contaminant. Train workers within the procedures and protocols, establish communication between group agencies and hospitals, frequently examine equipment, and rehearse setups. Obtain template protocols from both the peer-reviewed medical literature and the government literature if needed. Heard K: the changing indications of gastrointestinal decontamination in poisonings. American Academy of Pediatrics Committee on Injury, Violence, and Poison Prevention: Poison treatment within the residence. American Academy of Pediatrics Committee on injury, violence, and poison prevention. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. Eddleston M, Haggalla S, reginald K, et al: the hazards of gastric lavage for intentional self-poisoning in a resource poor location. Dunning K, Plymyer Mr: Charcoal peritonitis inflicting continual pelvic ache: a novel complication following bariatric surgery. Askenasi r, Abramowicz M, Jeanmart J, et al: Esophageal perforation: an uncommon complication of gastric lavage. Coutselinis A, Poulos l, Boukis D: A deadly complication to gastric lavage leading to malpractice suit: a case report. Justiniani Fr, Hippalgaonkar r, Martinez lO: Charcoal-containing empyema complicating therapy for overdose. Bachrach l, Correa A, levin r, et al: Iron poisoning: issues of hypertonic phosphate lavage therapy. Miyauchi M, Hayashida M, Yokota H: Evaluation of residual poisonous substances within the stomach utilizing upper gastrointestinal endoscopy for administration of patients with oral drug overdose on admission: a potential, observational research. Hojer J, Personne M: Endoscopic elimination of gradual release clomipramine bezoars in two instances of acute poisoning. Haider F, De Carli C, Dhanani S, et al: Emergency laparoscopic-assisted gastrotomy for the treatment of an iron bezoar. Miyauchi M, Hayashida M, Hirata K, et al: Gastric lavage guided by ultrathin transnasal esophagogastroduodenoscopy in a life-threatening case of tobacco extract poisoning: a case report. Briggs Al, Deal ll: Endoscopic elimination of pharmacobezoar in case of intentional potassium overdose. Donoso A, linares M, leon J, et al: Activated charcoal laryngitis in an intubated patient. Okumura T, Suzuki K, Fukuda A, et al: the Tokyo subway sarin attack: disaster administration, half 1: neighborhood emergency response. Okumura T, Suzuki K, Fukuda A, et al: the Tokyo subway sarin assault: catastrophe administration, half 2: hospital response. Nozaki H, Hori S, Shinozawa Y, et al: Secondary publicity of medical staff to sarin vapor in the emergency room. George G, ramsay K, rochester M, et al: Facilities for chemical decontamination in accident and emergency departments within the United Kingdom. Moll J, Kerns W, Tomaszewski C, et al: Incidence of aspiration pneumonia in intubated sufferers receiving activated charcoal. Effectiveness of multiple-dose activated charcoal in enhancing carbamazepine elimination. Prescott lF, Hamilton Ar, Heyworth r: Treatment of quinine overdosage with repeated oral charcoal. Position statement and practice guidelines on using multi-dose activated charcoal within the therapy of acute poisoning. Jones J, Heiselman D, Dougherty J, et al: Cathartic-induced magnesium toxicity during overdose administration. Brent J: Water-based solutions are one of the best decontaminating fluids for dermal corrosive exposures: a mini evaluate. They are essentially related in function and design; however, the former is usually reserved for medical considerations and the latter for analysis of traumatic pathology. Following a blunt mechanism of damage, its best utility is as a triage tool within the evaluation of hemodynamically unstable, multiply injured patients. Peritoneal aspiration, in which an attempt is made to retrieve free intraperitoneal blood, precedes lavage. A finding of intraperitoneal blood is a marker for intraperitoneal organ injury and obviates the necessity for subsequent lavage. In the lavage portion, normal saline is launched by catheter into the peritoneal cavity, recovered by gravity, and analyzed for proof of great intraperitoneal harm. Peritoneal lavage can be used as a therapeutic software in patients with hypothermia and as a method of removing toxins. It was integral to both discount of unnecessary laparotomies and discovery of unsuspected and life-threatening intraabdominal hemorrhage in patients with significant closedhead injury. It has been demonstrated that emergency clinicians and surgeons could be educated on this method to a level of competence sufficient for this need. Here its role is extra dominant than for blunt trauma due to the far higher likelihood of occult harm to hole viscera and the diaphragm after a penetrating mechanism. Thus, the presence of one or more mandates the need for pressing laparotomy and precludes the undertaking of other diagnostic research. This is particularly true in sufferers with extreme closed-head injury or excessive spinal twine harm, in whom bodily assessment of the stomach is sort of compromised. May be unreliable because of closed-head harm, intoxicants, distracting injury, or spinal wire harm. The length of remark should be 6 to 24 hours, relying on whether or not diagnostic exams have been carried out, the results of the exams, and medical circumstances, including the absence of factors rendering the examination unreliable. Adjustment of the method and web site of performance allows relative contraindications to be overcome. Relative contraindications include previous abdominal surgery or infections, weight problems, coagulopathy, and second- or third-trimester being pregnant. The sole absolute contraindication is when clinical mandates for urgent laparotomy exist already.
Aldara 5 percent low price
Lower Extremity Background Injuries to the lower extremities acne questionnaire cheap 5 percent aldara overnight delivery, including sprains skin care event ideas aldara 5 percent generic mastercard, fractures, and dislocations, are additionally commonly encountered by prehospital care providers. One fundamental distinction between splinting upper and lower extremity injuries is use of a traction splint within the management of femoral fractures. The use of traction and countertraction for alignment and discount of fractures dates from the time of Hippocrates. Similar to the arm splints described earlier, many prefabricated leg splints are commercially available. Anteroposterior and lateral views of the right femur show a displaced, angulated, and foreshortened femoral fracture. Such accidents may end in substantial hemorrhage into the thigh, even to the purpose of hemorrhagic shock. During World War I, the modified splint was credited with reducing the mortality rate related to fractured femurs from 80% to 15%. This in turn increases tissue stress, decreases the potential house for blood loss, and inhibits further hemorrhage. In addition, traction splints help reduce ache, forestall further damage to neurovascular structures, and reduce the incidence of fat embolism. Contraindications Do not use traction splints on sufferers with pelvic fractures, hip injuries with gross displacement, important accidents involving the knee, or avulsion or amputation of the ankle or foot. In these circumstances, the quantity of traction required to realign the fractured femur can distract the distal fracture website. There has been some controversy over whether a traction splint should be applied to an open femoral fracture for fear that the use of traction may enable contaminated bone fragments to retract into the wound. A 2011 replace to the International Trauma life Support guidelines recommends use of traction splints on open femur fractures only in the austere surroundings or when entry to definitive care might be significantly delayed. If traction does force contaminated bone fragments into the wound, this information have to be relayed to the receiving clinician and antibiotics initiated as quickly as potential. In either case, stabilization of the fracture site to prevent additional hemorrhage, neurovascular injury, or gentle tissue harm should take priority, whereas making every effort to reduce the danger for increased contamination. Equipment whatever the sort or producer, the essential traction splint consists of a steel body that extends from the proximal finish of the thigh to an space distal to the heel. The padded proximal end matches against the ischial tuberosity and serves as the anatomic fixation point. The proximal portion of the splint could additionally be a ring that encircles the proximal finish of the thigh, a partial ring, or a padded bar. All traction splints even have a number of delicate elastic straps that assist the thigh and leg. Each of these splints has its own advantages, disadvantages, and distinctive methodology of application. For example, traction splints that use a half-ring design apply countertraction to the ischial tuberosity from under the shaft of the femur. A extensive number of gadgets are commercially obtainable, every with its personal advantages, disadvantages, and unique strategies of application. Place the ankle hitch across the posterior of the heel so that the traction strap hangs inferiorly, beneath the foot. While one rescuer gently applies traction and lifts the leg, slide the splint under the affected person. Stop making use of traction as quickly as the leg has resumed its regular size (compare with the unhurt side). Pain is at all times associated with the application of a traction splint, so make every effort to provide appropriate analgesia. In addition, reassure the affected person that, though the initial utility of traction is usually quite painful, stabilization of the fracture website will help scale back subsequent discomfort. If the injured leg is markedly deformed, an assistant should first attempt to straighten it with guide traction and keep that place till a splint has been utilized. The amount of traction necessary to straighten a badly deformed extremity will vary, but not often exceeds 15 lbs of drive. If the patient strongly resists whereas traction is being utilized, stop the process and splint the injured extremity within the position during which it was found. If the splint has an adjustable bar, determine the suitable length by measuring the unhurt leg. To make certain that the injured extremity will stay elevated once handbook traction has been released, unfold the heel stand and lock it into place. Place the Sager Emergency Traction Splint (Minto research and Development) between the legs and towards the ischial tuberosity, carefully avoiding or protecting the genitalia. Next, place the ankle harness instantly above the medial and lateral malleoli and connect it to the distal end of the traction splint. For dynamic quantifiable splints corresponding to Sager-type units, gently extend the internal shaft of the splint till the desired quantity of traction is achieved, both by comparing leg length or using the quantitative scale to set the specified drive. Grasp the Kydex buckle and slide the thigh strap up under the leg so that the perineal cushion is cosy against the perineum and ischial tuberosity. Tighten the Kydex buckle thigh strap to draw the perineal-ischial pad to the lateral portion of the crotch. Extend the inside shaft of the splint by opening the shaft lock and pulling the internal shaft out till the specified amount of traction is famous on the calibrated wheel. As a tough information to decide the amount of traction needed, apply 10% of body weight to a maximum of 22- to 25-lb (10- to 25-kg) traction. Next, apply the shortest 6-inch extensive strap over the ankle harness and lower the leg. Note that the splint can alternatively be strapped to the outer portion of the leg. After software of the splint, be sure to recheck distal neurovascular standing and then safe the patient and splint firmly to the ambulance stretcher. Take additional care whereas shifting the affected person and when closing any transport vehicle door to avoid pointless motion and additional harm. If the splint extends beyond the dimensions of the stretcher, further assist for the splint may be needed. Complications Complications are typically the outcome of incorrect utility and include pain, ongoing hemorrhage, peroneal nerve damage, perineal injury, movement at the fracture site, ligamentous injury, damage to unrecognized fractures elsewhere, or additional neurovascular compromise. Conclusion When properly utilized, traction splints reduce the ache, hemorrhage, and potential injury to adjacent structures which are associated with femoral fractures. Major pelvic trauma such as this will lead to uncontrollable hemorrhage and hypovolemic shock. Indications and Contraindications Apply a pelvic circumferential compression gadget to any affected person with vital pelvic ache, tenderness, or proof of pelvic instability after trauma, particularly if the affected person is hypotensive. Procedure Stabilization of the pelvis consists primarily of compressing the bony ring. To apply a sheet, place it over a protracted backbone board after which gently logroll the affected person by not extra than 15 levels into position on the board.