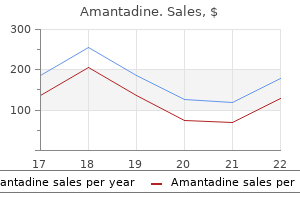
Amantadine
Amantadine dosages: 100 mg
Amantadine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy amantadine 100 mg lowest price
With each passing year hiv infection rate greece buy cheap amantadine 100 mg on line, more urologists are performing laparoscopy antiviral pills discount amantadine 100 mg line, particularly laparoscopic nephrectomy. The enhance in use, nevertheless, was very modest within the first decade following Clayman et al. Why did laparoscopic nephrectomy take so long to catch on, but then subsequently become a regular procedure This historical past of laparoscopic nephrectomy contrasts starkly with that of other laparoscopic procedures launched in the same time period (late Nineteen Eighties to mid 1990s). The major cause proposed in the mid Nineties was that laparoscopic nephrectomy was too tough for the common urologist to develop and to keep the required operative abilities, given the relative infrequency of nephrectomy in a typical urology follow. There have been other factors as well, including concern about oncologic efficacy, the inefficiency of increased operative time, and safety of the process in case of vascular harm. Once a important mass of surgeons started performing laparoscopic nephrectomy, combined with affected person demand, its recognition was inevitable. Commercial gadgets to facilitate laparoscopic hand help have been under improvement by this time [6], and in 1996 Bannenberg et al. Gelport the Gelport equipment contains the Alexis wound retractor, which is a pair of plastic rings related by a flexible skirt that holds the stomach incision open and provides the bottom for the second component, and the Gelseal cap, which snaps on to the outer ring of the wound retractor to provide a gas-tight seal by way of which a hand or laparoscopic ports can be positioned. The base is a set length wound retractor comprised of an inside flexible ring and an outer inflexible ring linked by an elastic skirt that holds the abdominal incision open and provides the bottom for the second element. The outer cap is a pair of locking rings that snap on to the base and shut an iris valve to present gas occlusion. Slight inward actions of the forearm could be made, however massive actions require that the iris valve be opened a bit. Similarly, pulling back or removing the forearm necessitates tightening the valve to stop gasoline leak. Other surgeons have overcome the fluid downside through the use of a disposable fluid-impervious robe. Surgical devices can be placed in to the stomach for use by the intra-abdominal hand. Of these, the most useful may be handheld bulldog clamps for short-term vascular occlusion. Additionally, there are instruments made specifically to be used by the intra-abdominal hand. However, the first surgeon then has just one hand free to manipulate a laparoscopic instrument. The proper hand is used intra-abdominally, which permits retraction of the liver by the back of the hand whereas dissecting the kidney. The assistant operates the videolaparoscope (#2) and an assisting instrument (#4). In this part, some methods which are totally different from open surgery and from normal laparoscopic surgical procedure are highlighted. A laparoscopic port may be inserted via both the Gelport and the Dextrus Access Port, and the Gelport will accommodate a quantity of ports or a hand and additional ports. This maneuver must be carried out solely with noncutting trocars and only after visual inspection has confirmed the inner stomach wall to be free of adhesions. Some surgeons place a hemostat on the blue tag of the laparotomy pad to stop its full placement in to the abdomen. We prefer to place the complete pad inside the stomach to permit its unrestricted use, but we do cut off the blue tag and instead clamp it to the drapes as a visible reminder that a pad is inside the stomach. Performing multiple duties concurrently with the intra-abdominal hand takes greatest advantage of its presence. Retraction and exposure can be obtained in a quantity of directions without delay, or the hand can concurrently retract and dissect. One of the most helpful multitasking hand positions is the "C" position (a term coined by Stephen E. Using the left hand for left renal surgical procedure, or the right hand for right renal surgery, the forearm is positioned parallel to the good vessels, palm lateral, wrist flexed 45�90�, index finger lifting the kidney, thumb exerting inferomedial traction on tissue, and the middle fingers extended. This place allows simultaneous retraction of bowel with the back of the hand, elevation of the lower pole, and dissection with the fingers. When the hand is elevating the lower pole, an irrigator�aspirator probe or another instrument may be positioned by way of an assisting port to help in the dissection. When dissecting out the renal hilum, the renal artery and vein may be encircled en bloc with the thumb and forefinger of the intra-abdominal hand. This maneuver is secure so lengthy as a careful touch is used, sensing resistance that signifies an early branch or an adjunct vessel. Encircling the hilum on this method offers the power to rapidly management it in case of vascular damage, and with this added confidence the next hilar dissection can proceed quickly. The imply operative time was 158 min and the major complication rate was only 4%, with a fee of conversion to open surgery of 3%. At the University of Michigan, the 5-year recurrencefree survival in a sequence of 108 patients with a imply tumor size of 6. In the total of 621 patients described in these series, the operative time averaged 261 min, with 7% main and 14% minor complication charges overall. Among the 12 such sequence containing one hundred or more sufferers, reporting 2034 patients in complete, the imply operative time was 182 min and the imply warm ischemia time 2. In the studies that reported convalescence, the imply time to return to nonstrenuous exercise levels was 24 days. The 1-month, 1-year, and 3-year actuarial graft survival rates are 97%, 95%, and 94%, respectively. Even when utilizing standard or robot-assisted techniques, many surgeons favor to create a minimum of part of the urinary diversion via a mini-laparotomy. Intraoperative blood loss, postoperative narcotic use, and time to oral intake have been similar in all three teams. However, the intra-abdominal hand does seem to reduce some specific complications, particularly the necessity to convert to open surgical procedure. In one literature compilation which included fifty six reports, there was a significantly Wolf et al. The mean operative time for hand help was ninety min shorter than that for normal laparoscopy. Silberstein and Parsons assessed the literature 2 years later and considered all types of nephrectomies, and included 25 studies comprising 3051 patients [105]. They found that hand-assisted nephrectomy was associated with significantly less operative blood loss and decreased danger of conversion, but that there have been no significant differences in operative time, size of stay, or risk of perioperative transfusion or complication. Narcotic use tended to be much less within the former group, however the difference was not considerably completely different. Conversely, there was considerably more neck pain associated with normal laparoscopy. There was no important distinction between the approaches when it comes to lower back pain. There had been no main variations as regards to shoulder, upper again, and decrease again ache. Another main consideration is surgeon expertise, with laparoscopy normally or with Table 76.
Cheap 100 mg amantadine with visa
At the identical time hiv infection rates by group purchase 100 mg amantadine visa, renal blood move increases within the contralateral kidney as renal perform decreases within the obstructed kidney hiv infection risk percentage order amantadine 100 mg with mastercard. The return of renal perform after a interval of complete unilateral ureteral obstruction is a vital clinical concern for the urologist. The renal function recovery fee after 1 week of ureteral obstruction is 100 percent, but after 4 weeks solely a 30% recovery could be expected [5]. If only a partial obstruction is current, the identical modifications occur, but to a lesser diploma. Patients with an acute stomach of surgical origin usually lie as still as potential. The ache is usually diffuse in an acute stomach as opposed to renal colic where the affected person can often level to the positioning of most tenderness, which is more doubtless to be the site of the ureteral obstruction. Other scientific indicators that could be encountered are fever, chills, nausea, vomiting, and tachycardia. The presence of pyuria, fever, leukocytosis, or bacteriuria suggests the chance of a urinary an infection and the potential for an infected obstructed kidney. This is a doubtlessly lifethreatening scenario and should be handled as a surgical emergency. Mechanism of renal colic Renal colic is the consequence of the acute dilation of the urinary tract proximal to an obstruction together with smooth muscle spasm at the website of the obstruction. In addition, ureteral smooth muscle spasm is directly stimulated by prostaglandin E2 [3]. Most of the ache receptors of the higher urinary tract liable for the perception of renal colic are situated submucosally within the renal pelvis, calyces, renal capsule, and upper ureter. Acute distention appears to be most necessary within the growth of the pain of acute renal colic. Muscle spasm, elevated proximal peristalsis, and native irritation on the website of obstruction might contribute to the development of ache through chemoreceptor activation and stretching of submucosal free nerve endings. Diagnosis the prognosis of renal colic is commonly made based on medical symptoms alone, though confirmatory exams are normally carried out. Additional checks are helpful not solely to confirm the prognosis but in addition to facilitate within the decision-making process on additional treatment. Before a call on therapy may be made, a urologist should know the scale, shape, orientation, radiolucency, and placement of the stone. Other elements that will affect additional remedy are kidney operate and the presence of infection, in addition to all different clinical information and comorbid circumstances the patient could have. In explicit, hematuria testing has a sensitivity of 81�84% and a specificity and unfavorable predictive worth of 48% and 65%, respectively [6, 7]. In addition to the presence of blood in the urine, the presence or absence of leukocytes, crystals, and micro organism, and the urinary pH should be documented. The statement of cystine, uric acid, struvite, or calcium oxalate crystals within the urine may be a sign of the kind of calculus in the end found. Autoregulatory process associated with obstruction the preliminary renal response to acute unilateral ureteral obstruction is the release of prostaglandins, particularly E2, leading to vasodilatation of the afferent arterioles and worsening of ureteral smooth muscle spasm. Subsequently, the dilation of the afferent arterioles leads to an increase in renal blood flow and glomerular filtration price [4]. As a consequence, more urine is produced, and the renal pelvis and ureter dilate further. Peak hydrostatic renal pelvis strain is attained inside 2�5 h after an entire obstruction. Urea, creatinine, and electrolyte testing could also be useful in identifying patients with renal function impairment as properly as in giving some data on the hydration status of the patient, which can determine their further administration. Also, the progress of the stone could be easily monitored with a follow-up radiograph. Renal ultrasound Renal ultrasound is most useful in diagnosing comparatively giant calculi throughout the renal pelvis or kidney. Ultrasound can be used to diagnose different pathologic conditions such as belly aortic aneurysm or cholelithiasis, which may generally be mistaken for acute renal colic. Also, in sufferers with renal failure and diabetes mellitus, the danger of contrast-induced nephrotoxicity is 25% [10]. A serum creatinine stage of more than 2 mg/mL is a relative contraindication to the use of intravenous distinction. The classic discovering of acute ureteral obstruction is a persistent nephrogram, caused by a rise within the intrarenal concentration of the contrast. Even with out observing any specific calculus, the presence of a persistent nephrogram in a single kidney with prompt distinction excretion by the contralateral kidney is highly suggestive of ureteral obstruction secondary to a calculus. Extravasation of contrast across the accumulating system could also be a sign of a ruptured fornix, whereas pyelolymphatic backflow signifies that distinction has entered in to the renal lymphatic drainage system. This inaccuracy could be greatest compensated for by ensuring that slices are small in relation to stone dimension. In some instances, if the stone passed shortly earlier than the study, these signs may be the only proof that the affected person had a stone. These secondary indicators include ureteral dilation with hydronephrosis and renal enlargement with streaking of the perinephric fatty tissue [2]. In specific, the mix of amassing system dilation and perinephric stranding had a constructive predictive worth of 98%, while the absence of each of these secondary signs had a adverse predictive value of 91% [21]. Stone location may be described in anatomic phrases, however the scan lacks the surgical orientation that most urologists choose. It is widely believed that transverse stone dimension is more necessary than length in predicting the likelihood of spontaneous passage. This end result might be explained by orthogonal imaging in curved parts of the ureter, where larger anteroposterior diameters had been found no matter stone location. This effect is enhanced by the native inflammation within the ureteral wall with subsequent edema at the website of the calculus. Differential diagnoses of renal colic Alternative urologic pathology Pyelonephritis Pyelonephritis is a common reason for flank ache, but the discomfort is often described as a comparatively mild boring 680 Section 5 Stone Management in Urology: General Principles Obstructive uropathy as a result of different causes Other obstructive causes include: � Blood clots; � Renal papillary necrosis; � Ureteral strictures; � Renal cysts; � Polycystic kidney illness; � Pyelocalyceal diverticulum. Vascular pathology Abdominal aortic aneurysms Patients with an stomach aortic aneurysm could present with signs of flank pain that mimic renal colic. Large aneurysms may lie in shut approximation to the ureter and cause hematuria from local ureteral irritation. This imaging option could be a valuable adjunct in high-risk patients in choosing essentially the most acceptable treatment option as well as pretreatment planning. Flank and costovertebral angle tenderness are additionally current, however extra severe than with renal colic. Renal abscesses Renal abscesses tend to cause ache just like pyelonephritis quite than renal colic.
Purchase amantadine 100 mg overnight delivery
Therefore hiv infection globally amantadine 100 mg order, the effectiveness and price financial savings attributed to medical remedy on this examine are probably overestimated hiv infection nejm amantadine 100 mg without a prescription. Chandhoke used a price model to determine the stone recurrence price at which medical remedy turns into cost-effective [5]. For the model, he assumed that all recurrent stones turned symptomatic and required either an emergency room visit or surgical procedure. Additionally, he assumed a restricted metabolic analysis consisting of an workplace visit, two 24-h urine collections, imaging studies at 6-month intervals, and drug remedy distributed based on a printed study. This sort of more superior analysis allows stratification of sufferers according to the aggressiveness of their 767 illness, but was restricted in that it evaluated just one technique of metabolic analysis and treatment and it probably overestimated the probability that a recurrent stone will become symptomatic or require remedy, thereby rising the price of conservative therapy. The model took in to account accrual of cost for analysis, medications, emergency therapy, and surgical administration for recurrent stones. For first-time stone formers, conservative therapy was the most cost-effective strategy, leading to a stone recurrence fee of one episode each 14 years (Table sixty six. For recurrent stone formers, conservative remedy was still the least pricey method, nevertheless it was associated with an unacceptably high recurrence price of 0. Treatment strategies by which all patients obtained medication, no matter 24-h urine findings, significantly improved recurrence rates (by as much as 60%) over strategies where solely patients with a metabolic abnormality were prescription drugs. Interestingly, since conservative remedy (the least pricey approach) was related to an unacceptably high recurrence rate, this model demonstrated the practical cost-effectiveness of treating all recurrent stone formers with medicine regardless of the relatively excessive cost of drugs, as a result of the related vital reduction in recurrence rates. Now that potassium citrate is on the market in generic form, the cost-effectiveness threshold for medical remedy must be additional lowered. Medical treatment For different metabolic causes (% of patients) No drug K-Cit K-Cit (35) For no metabolic abnormality (% of patients) No drug K-Cit K-Cit (30) First-time stone formers Stone formation price (stones/ patient/year) 0. The benefit of this decision-tree model is that the cost-effectiveness of any medicine may be decided by inputting its related threat reduction and cost, and evaluating it using any of the six metabolic evaluation and treatment methods. As such, comparability of treatment costs from one nation to the subsequent may not be meaningful [5]. Conservative remedy based mostly on dietary remedy alone was probably the most cost-effective technique in first-time stone formers in all 10 international locations. Likewise, in other nations with comparatively low medication prices, like Turkey and Switzerland, the cost difference between conservative and empiric remedy was marginal, although empiric therapy was related to a significant enchancment in efficacy. Several European studies have concluded that medical remedy is cost-effective in their respective international locations. Using medication prices of 220 Euros/year and a cost/stone episode of 2500 Euros in Sweden, Tiselius calculated that with an preliminary stone recurrence rate of 0. Strohmaier and H�rmann, presuming the next recurrence fee of 50% per yr, found that a 40% risk discount related to medical remedy would lead to yearly savings of 333. It is clear from these worldwide value analyses that differences in the value of medication and surgical procedure across healthcare methods, largely based on subsidization, are answerable for variations within the cost-effectiveness of medical management remedy methods. When medicine prices are regulated or backed, the low cost of Chapter 66 Cost-Effective Strategies for Management of Renal and Ureteral Calculi medicine favors drug therapy. On the opposite hand, when the price of medications is high, the comparatively rare want for surgery to treat stone recurrences and the fastened reimbursement for surgical procedures favor a conservative strategy. Conclusions Careful cost analyses are the key to developing costeffective remedy methods. Consequently, cost-effectiveness models, which soak up to account not solely cost but also efficacy, are invaluable for evaluating different remedy strategies and for evaluating treatments in several establishments or healthcare systems. However, even cost-effectiveness models are only as useful because the assumptions and price information inputted in to them and have to be rigorously scrutinized. Their advantage over cost analyses is that they are often utilized to any establishment or country by changing the variables, corresponding to success charges or price. While determination of cost-effective practices is invaluable at a societal stage, we must not lose sight of the impact of remedy choices on the person. Thus in lots of situations, a treatment choice is chosen to maximize efficacy or another outcome (such as stone recurrence rate) despite its larger price. Direct and indirect costs of nephrolithiasis in an employed population: alternative for illness administration International comparability of value effectiveness of medical administration strategies for nephrolithiasis. Unenhanced helical computed tomography vs intravenous urography in sufferers with acute flank pain: accuracy and financial influence in a randomized prospective trial. Cost-effectiveness of medical expulsive therapy using alpha-blockers for the treatment of distal ureteral stones. Efficiency and price of treating proximal ureteral stones: shock wave lithotripsy versus ureteroscopy plus holmium: yttrium-aluminum-garnet laser. Comparison between extracorporeal shock wave lithot- 770 Section 5 Stone Management in Urology: Cost-Effectiveness and Long-Term Stenting of percutaneous nephrostolithotomy. Synchronous bilateral percutaneous nephrostolithotomy: evaluation of scientific outcomes, cost and surgeon reimbursement. The Hickman peel-away sheath: different for pediatric percutaneous nephrolithotomy. The "mini-perc" approach: a less invasive various to percutaneous nephrolithotomy. Predictors of clinical significance of residual fragments after extracorporeal shockwave lithotripsy for renal stones. Clinical implications of clinically insignificant store fragments after extracorporeal shock wave lithotripsy. Residual fragments after percutaneous nephrolithotomy: price comparability of quick re-assessment versatile nephroscopy versus expectant management. Treatment of mid- and decrease ureteric calculi: extracorporeal shock-wave lithotripsy vs laser ureteroscopy. Optimal remedy for the distal ureteral stone: extracorporeal shock wave lithotripsy versus ureteroscopy. Cost and efficacy of extracorporeal shock wave lithotripsy versus ureteroscopy in the treatment of decrease ureteral calculi. Cost-effectiveness v affected person desire within the alternative of therapy for distal ureteral calculi: a literature-based choice evaluation. Lower pole I: a potential randomized trial of extracorporeal shock wave lithotripsy and percutaneous nephrostolithotomy for decrease pole nephrolithiasis-initial results. Efficacy and cost-effectiveness of extracorporeal shock wave lithotripsy for solitary decrease pole renal calculi. Chapter 66 Cost-Effective Strategies for Management of Renal and Ureteral Calculi fifty six. Randomized controlled trial of a low animal protein, excessive fiber diet in the prevention of recurrent calcium oxalate kidney stones. In: Urolithiasis 2000: Proceedings of the 9th International Symposium on Urolithiasis Cape Town (South Africa). Urolithiasis 2000: Proceedings of the 9th International Symposium on Urolithiasis Cape Town (South Africa). The efficacy of ureteral stents within the administration of various urologic circumstances causing higher urinary tract obstruction has been extensively proven and their contribution to urology remains monumental. Regardless of the stent design and composition, using ureteral stents is related to several issues, which limit their use and necessitates the escalation of research in course of the introduction of the "perfect" ureteral stent. The properties of the perfect stent embody the flexibility to hold its position (memory) over time (durometry), easy manipulation of its form (elasticity), and excellent tensile strength whereas having elongation capacity.
Buy generic amantadine 100 mg on line
Additionally hiv infection through needle prick 100 mg amantadine discount, standard trocars could be added adjoining to the commercially obtainable "multichannel ports hiv eye infection pictures purchase amantadine 100 mg line," through the identical skin incision but in to a separate fascial stab in a hybrid format. There are a quantity of single port devices available, each with their own advantages and downsides (Table 106. They differ within the variety of obtainable operative inlets and total size, but in any other case are identical. The retractor consists of 1 internal ring and two external rings, and a double-over cylindrical plastic sleeve; the latter is attached to the internal ring of the two external rings and descends, circles the inner ring, and exits between the two outer rings. The valve element incorporates three or 4 inlets for introduction of devices. The three-inlet valve (TriPort) has one inlet for a 12-mm instrument and two for 5-mm devices. Multiple trocar configuration this trocar configuration consists of a single skin incision with several ports placed via separate fascial websites. Two separate 5-mm trocars have been placed by way of an intraumbilical incision through two separate fascial stab incisions. The procedure was performed and the specimen extracted after the fasciotomies had been joined, leaving a near scar-free look. Multiple trocars of various measurement may be launched via the GelSeal cap and the specimen may be extracted once the GelSeal cap has been eliminated. It has a smaller gel cap and 4 premade self-retaining 5-mm trocars, though numerous sized trocars may be placed much like the GelPort. It removes smoke from the field of vision and filters it, as a substitute of venting it in to the room. The system displays and permits the insufflator to adjust as wanted to ensure a secure pneumoperitoneum. The massive caps comprise two separate channels that allow for insufflation and smoke evacuation. Two configurations are available for single-site surgery: a cap with two 10/12-mm cannulas and a single 5-mm cannula; and a cap with one 10/12-mm cannula and two 5-mm cannulas. The multichannel hybrid laparoscopic ports require specialised devices (flexible gastroscope, etc. These ports are placed via a single pores and skin and fascial incision using the Hasson method. It consists of three working channels that permit the introduction of instruments of up to 12. A plastic, however versatile, cap with three entry sites attaches to the two-piece metal gadget. Special curved instruments are inspired with this gadget along with an extra-long endoscope. Two rigid channels positioned vertically to the operative field accommodate the use of a scope and any other inflexible surgical instrument. Three pneumoperitoneum/vacuum ports exist to keep pneumoperitoneum and facilitate insufflation and/or smoke evacuation. The size 7 surgical glove is hooked up to the wound retractor and three to 4 of the finger tips are eliminated so the cannulas may be inserted and tied in place. The TransPort is more akin to a gastroscope/colonoscope than a regular laparoscopic instrument. This device creates the multitasking platform and makes use of a versatile endoscope along with multiple versatile endoscopic instruments. The umbilicus affords direct entry in to the peritoneal cavity and readily hides the surgical scar. Various incisions can be utilized, together with intra-, infra-, supra-, and peri-umbilical. Chapter 106 Laparoendoscopic Single-Site Surgery: Ports, Access, and Instrumentation 1279 date the desired port or trocar configuration. The incision is made through the pores and skin and dermis and carried down to the rectus fascia. For the a quantity of trocar configuration, the fascia is grasped, elevated, and pneumoperitoneum is achieved with the Veress needle technique. The AnchorPort system is inserted similarly, yet optical entry (placement of a 5-mm scope and camera via the port) can be used on all entries, not just the first. The AirSeal single port is inserted in a comparable fashion to a normal optically placed trocar besides that a specially designed hand piece permits for an off-set hand position to help information the cannula. The TriPort and QuadPort require that a sequence of producer directions are followed to enable accurate placement. This system may be positioned in a closed Veress needle fashion, with an enlarged fascial incision, or with the open Hasson method. Once by way of the peritoneum, the thumb-switch on the introducer is depressed and the distal ring is deployed. The introducer is then eliminated and the sleeve is pulled upwards to deliver the interior ring in to contact with the internal abdominal wall. The extra sleeve is eliminated and slack within the port is removed with the retracting ribbon. After the umbilicus has been dissected free of the rectus fascia, and the preperitoneal fat visualized, entry in to the abdomen is gained bluntly with both a finger or handheld clamp. The Alexis wound retractor is inserted by way of the fascia and care is taken to avoid entrapping bowel when folding the retractor. Both the gel cap of the GelPort/GelPoint or surgical glove of the handmade port is mounted in to place and insufflation is begun via the connected cannula or a preinserted laparoscopic trocar. By off-setting the incision closer to the meant target organ, a more direct access to the surgical subject is created, which may improve tissue retraction and instrument range of movement; nonetheless, the scar could also be extra seen exterior the umbilicus. Retroperitoneal Retroperitoneal entry is achieved with an open (Hasson) approach. The flank muscle fibers are separated with two S-retractors to visualize the anterior thoracolumbar fascia, which is incised to enter the retroperitoneal house with the tip of the index finger. To decrease clashing, specifically designed devices have been created, including instruments that are prebent and ones that articulate. Additionally, improvement in obtainable optics within the type of smaller diameter scopes, highdefinition imaging, low-profile hooked up cameras, and deflectable scope ideas considerably contribute to the broader acceptance of this surgical method. Compared to normal laparoscopic devices, they allow for the power to triangulate and reduce internal and external clashing. When compared to versatile instrumentation within the laboratory setting, prebent instruments have been much less time-consuming and have been found to have higher maneuverability [35]. The full line of devices includes a bipolar coagulator, varied graspers, dissectors, and needle drivers. As a end result, intraoperative telescope adjustments are sometimes pointless, and the surgeon is ready to optimally view the whole surgical field. The inflexible scopes are available in 5 and 10 mm versions with 0�, 30�, or 45� course of views. A 100� subject of view from a number of angles can seize the specified location head-on, from above, and even from behind.
Purchase 100 mg amantadine fast delivery
Tumor necrosis factoralpha-induced accentuation in cryoinjury: mechanisms in vitro and in vivo hiv infection eye splash cheap amantadine 100 mg free shipping. Contemporary outcomes of percutaneous biopsy of one hundred small renal lots: a single heart experience hsv-zero antiviral herpes treatment amantadine 100 mg purchase without a prescription. Radiofrequency ablation of renal cell carcinoma: half 2, Lessons discovered with ablation of one hundred tumors. Laparoscopic renal tumor cryoablation: appropriate software of real-time ultrasonographic monitoring. Utility of iodinated distinction medium in hydrodissection fluid when performing renal tumor ablation. Protecting the ureter during radiofrequency ablation of renal cell 1370 Section 7 Image-Guided Diagnostics and Therapeutics: Upper Tract and laparoscopic cryoablation for the therapy of stable renal plenty. Complications of laparoscopic and percutaneous renal cryoablation in a single tertiary referral center. Successful conservative management of colorenal fistula after percutaneous cryoablation of renal-cell carcinoma. Stereotactic percutaneous cryoablation for renal tumors: initial clinical expertise. Probe retraction throughout renal tumor cryoablation: a technique to reduce direct ureteral injury. Prophylactic gelatin sponge tract injection to prevent bleeding after percutaneous renal cryoablation in a swine mannequin. Single heart expertise with percutaneous and laparoscopic cryoablation of small renal plenty. Percutaneous cryoablation of renal masses >3 cm: efficacy and security in remedy of 108 sufferers. Correlation of radiographic imaging and histopathology following cryoablation and radio frequency ablation for renal tumors. Comparison of postoperative ache, convalescence, and patient satisfaction after laparoscopic and percutaneous ablation of small renal masses. In 2008, it was estimated that over 186 000 males can be identified with prostate cancer, with solely 10% of these men being diagnosed with high-risk prostate cancer [1, 2]. This shift towards low-risk illness, in addition to youthful age on the time of analysis, not solely improves the potential outcomes of treatment, but additionally emphasizes the necessity to discuss remedy choices inside the context of quality-of-life outcomes. Long-term outcomes have proven that oncologic management or "treatment" is attainable with definitive treatment in a high proportion of circumstances. Interest in brachytherapy re-emerged within the 1970s when Whitmore and associates at Memorial Sloan Kettering in New York established an open, retropubic method utilizing iodine125 seeds [9]. The 15-year outcomes were disappointing, with solely 21% of patients reported to be controlled. A resurgence of prostate brachytherapy occurred in the Eighties due to the transperineal strategy developed by Holm et al. The strategy adopted in Seattle utilized a "pre-plan" to account for the seed placement, whereas in New York a extra conservative strategy was developed to restrict the morbidity of the process by peripherally putting seeds to restrict central sizzling spots [11]. Patient choice Implantation of the prostate is a gorgeous option as a result of it concentrates treatment on the prostate and minimizes radiation exposure and morbidity to nearby organs, including the bladder, rectum, and small bowel. The implant serves as the supply mode of the isotopes, which decay over time and represent the actual therapy. History of prostate brachytherapy Prostate brachytherapy predates radical prostatectomy, having been introduced in the Twenties with radium needle implants. Later, in the 1960s, radioactive gold seeds had been used to deal with prostate cancer [8]. Accurate placement of the needles is achieved with this method and the isotopes are positioned via them in to the prostate. Several approaches are used for seed implant, however the necessary thing to success is more the implant quality than the approach. One strategy requires linked or stranded seeds to be positioned based on a "pre-plan" of the implant. Another approach is a realtime, adaptive implant, using an interstitial gun to place every seed. Using intraoperative software, a "forward" plan can be generated primarily based on the exact prostate volume and site. Also, with dynamic and adaptive evaluation, fewer sources can be utilized whereas sustaining a high quality implant. Use of fewer seeds provides a possibility for reducing each the rectal and urethral doses while still attaining sufficient prostate coverage. Given its shorter half-life, it was postulated that 103Pd would become the preferred isotope for tumors of upper Gleason score, because of their sooner tumor doubling time [21]. Nevertheless, there have been no information to date to suggest that isotope alternative should be primarily based on tumor grade or prostate cancer doubling time. Further, the long-term impact on efficiency of even a 3-month course of androgen ablative therapy needs to be thought-about. At present, an age-related bias exists throughout the urologic community, with youthful patients being referred extra usually for radical prostatectomy than both radiation or no therapy. Several research have proven an increased risk of bladder and colorectal most cancers in men who had been treated with radiation for prostate cancer [16, 17]. Nevertheless, this stays a valid concern and must be mentioned with each patient. Stage and grade migration over time could make long-term knowledge less relevant to the present patient. In several studies, implant quality as measured by the D90 dose (the radiation dose that covers 90% of the prostate volume) correlates with consequence. This research additional confirmed the importance of implant dosimetry for predicting end result. Unique to predictive fashions, this nomogram could additionally be used a priori to calculate a D90 dose that probably achieves a desired end result with further validation. Many of the unwanted effects seen with brachytherapy are related to radiation exposure of the urethra, bladder, and rectum. These unwanted facet effects can have critical quality-of-life implications, and brachytherapy requires knowledgeable consent from the patient. In a prospective analysis of the standard of life of sufferers present process primary remedy for prostate most cancers, Sanda et al. Long-term outcomes of retropubic everlasting 125iodine implantation of the prostate for clinically localized prostatic most cancers. A modified approach allowing interactive ultrasound-guided three-dimensional transperineal prostate implantation. Postimplantation dosimetric analysis of permanent transperineal prostate implantation: improved dose distributions with an intraoperative computer-optimized conformal planning approach.
Schisandra. Amantadine.
- What is Schisandra?
- Dosing considerations for Schisandra.
- Are there safety concerns?
- Improving concentration, coordination, and endurance.
- Improving liver function in patients with hepatitis.
- Vision problems, preventing premature aging, preventing motion sickness, diabetes, high blood pressure, and other conditions.
- How does Schisandra work?
- What other names is Schisandra known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96390
Generic 100 mg amantadine
Ipsilateral and dual-lumen double-pigtail polymeric stents the use of two ipsilateral double-pigtail polymeric stents for the management of extrinsic ureteral obstruction proof against antiviral essential oils 100 mg amantadine order mastercard a single stent insertion was proposed almost a decade ago [52] anti viral hand foam norovirus amantadine 100 mg safe. The first report included five sufferers who were handled for ureteral obstruction because of ureteral orifice stricture, retroperitoneal fibrosis, and center ureter stricture. These sufferers had been managed successfully by the insertion of two ipsilateral 7F ureteral stents, which have been exchanged at 3-month intervals till the sufferers were managed surgically [52]. In a subsequent report, malignant ureteral obstruction in seven patients was managed by the insertion of two ipsilateral stents [53]. Previous insertion of a single double-pigtail stent had been unsuccessful in the management of the obstruction. Three sufferers died inside three months after the insertion of the 2 ipsilateral stents, whereas the remaining four had a mean follow-up of 16 months (38 months maximum). A novel dual-lumen double-pigtail stent composed of two adhered ureteral stents has been evaluated in a porcine mannequin. The main advantage of this stent is that its insertion requires just one guidewire, whereas insertion of two ipsilateral stents requires two guidewires, making the procedure more cumbersome [16]. Biodegradable polymeric stents Biodegradable polymeric supplies and stents have been proposed in urology for over a decade. The stent is designed to maintain ureteral patency for forty eight h, after which it softens and eventually degrades. The stent contributed to the discount of vesicoureteral reflux and postoperative renal an infection because of its perform as a partial catheter. Drug-eluting and drug-coated polymeric stents Recently, polymeric ureteral stents which are coated with pharmaceutical substances or launch medication from their floor to the encompassing tissue have been introduced and clinically examined. Triclosan is a broad-spectrum antibacterial and antifungal agent which has been reported to inhibit the growth of widespread bacterial uropathogens in vitro, and is thus thought of useful for the reduction of urinary tract infection and subsequent encrustation of an indwelling stent [58]. A significant lower in Proteus mirabilis progress and survival was noticed in a rabbit experimental model when a triclosan-eluting ureteral stent was inserted within the urinary system (bladder) 776 Section 5 Stone Management in Urology: Cost-Effectiveness and Long-Term Stenting teral strictures in sufferers not suitable for surgical remedy were treated with the Wallstent by Pollak et al. In two patients, three stents have been implanted for the palliative administration of malignant illness and had been patent up till dying (3�5 months after implantation). Ingrowth of hyperplastic and granulation tissue was liable for the occlusion of all stents inserted for benign strictures, whereas tumor ingrowth and granulation tissue had been noticed in malignant instances. Wallstent endoprosthesis proved to be ineffective for long-term drainage in sufferers with benign ureteroenteric strictures. The mid-term clinical consequence of the Wallstent self-expandable stent implantation for the management of malignant ureteral obstruction was evaluated in forty sufferers with 54 malignant ureteral obstructions [37]. Patency was confirmed in 51 of the stented ureters through the imply follow-up period of 10. Almost half of the ureters (49%) required additional procedures to preserve patency. Tumor ingrowth requiring additional coaxial stent placement and borderline tumor overgrowth had been noticed in a single case each. Urothelial hyperplasia was noted in all stented ureters and additional retrograde insertion of a doublepigtail stent was deemed needed for a 1-month interval. The trumpet-like configuration was a constant finding in the course of the follow-up interval. Ten ureters (10 patients) with malignant obstruction have been treated with this mixture. The doublepigtail stents had been eliminated in seven patients 2 and three months after the implantation. Nevertheless, this mix was adequate to achieved inner urinary drainage. In these stories between 1 and 18 sufferers were handled, while the number of [59]. In eight sufferers significantly fewer antibiotics had been administered, and there was a slightly higher number of positive urine cultures, however significantly fewer symptomatic infections with long-term use of the triclosaneluting stent. Bacterial resistance to triclosan was not noted through the 3-month follow-up period [60]. A lately launched ketorolac-eluting stent was evaluated for its short-term efficacy in a double-blind randomized multi-institutional clinical trial [61]. The 276 sufferers included had been divided in to two groups (triclosan stent and standard stent). There were no significant variations in main and secondary intervention rates between the two groups. Fewer patients with the ketorolac-eluting stents used ache medication compared to the control group. A heparin-coated double-pigtail ureteral stent was introduced in an attempt to minimize microbial adhesion, biofilm formation, and subsequent encrustation of long-term indwelling stents within the urinary tract. In 5 patients, a heparin-coated ureteral stent was inserted in one ureter and a standard double-pigtail stent in the other for a month [62]. The thickness of the encrustations observed by electron microscopy on the heparincoated stents was significantly less compared to that on the standard ureteral stents. Moreover, the encrustation on the heparin-coated stents was less uniform and more compact. Two heparin-coated stents have been left indwelling long term (10 and 12 months) and on removing confirmed no evidence of encrustation and an unchanged heparin layer. The Wallstent consists of braided biomedical cobalt-based alloy monofilaments and is probably the most extensively used self-expandable endoprosthesis in the ureter [1]. Inserted in the ureter it seems to characterize a secure and efficient technique for the palliative therapy of malignant ureteral strictures. Benign and malignant ure- Chapter sixty seven Long-Term Stenting of the Ureter 777 handled ureteroileal strictures ranged between 1 and 24. Periodic trade of external�internal double-pigtail catheters until the tip of the follow-up period was performed in six ureteroileal conduits. The remaining instances had been managed by common trade of double-J catheters in retrograde style. The placement procedure was successful in all circumstances and patency was confirmed in all 4 patients. Additional interventions were deemed necessary in three instances because of urothelial hyperplasia, tumor ingrowth, and local recurrence of main most cancers invading the higher end of the ureter. It is a thermoexpandable shape-memory stent composed of nickel and titanium alloy. The Memokath 051 softens below 10 oC and regains its shape when reheated to 50 oC. Kulkarni and Bellamy have used the endoprosthesis for the administration of ureteral obstruction of each benign and malignant etiology [74].
Syndromes
- Feeling of fullness -- unable to drink as much fluid
- Feeding problems
- Adults: 150 to 310
- You vomit blood or pass blood in the stool
- Rubella (German measles)
- Have your blood pressure checked at least every year (blood pressure goal should be 140/80 mm/Hg or lower).
- Head injury
- Doppler ultrasound of the extremity
- General swelling, fluid retention
- Uremia (a result of kidney failure)
Buy amantadine 100 mg line
Prostate shape over the counter antiviral cream quality amantadine 100 mg, exterior striated urethral sphincter and radical prostatectomy: the apical dissection antiviral chicken pox 100 mg amantadine generic mastercard. Nerve sparing radical prostatectomy: results of hemostatic power sources on the recovery of cavernous nerve function in a canine model. Perioperative morbidity of laparoscopic radical prostatectomy in contrast with open radical retropubic prostatectomy. Analysis of three different vesicourethral anastomotic methods in laparoscopic radical prostatectomy. Vattikuti Institute prostatectomy: modern method and evaluation of outcomes. Intra- and perioperative outcomes comparing radical retropubic and laparoscopic radical prostatectomy: outcomes from a potential, randomised, single-surgeon examine. Prospective comparison of short-term convalescence: laparoscopic radical prostatectomy versus open radical retropubic prostatectomy. Comparison of high quality of life following laparoscopic and open prostatectomy for prostate cancer. Radical prostatectomy: a prospective comparability of oncological and functional outcomes between open and laparoscopic approaches. Recovery of quality of life in yr after laparoscopic or retropubic radical prostatectomy: a multi-institutional longitudinal examine. Changes in high quality of life in first 12 months after radical prostatectomy by retropu- 64. Laparoscopic radical prostatectomy a evaluation of the literature and comparison with open methods. Urinary continence after retropubic, perineal, and laparoscopic radical prostatectomy: prospective comparative research. Evidence from robot-assisted laparoscopic radical prostatectomy: a systematic evaluate. Radical retropubic versus laparoscopic prostatectomy: a potential comparability of functional end result. Comparative effectiveness of minimally invasive versus open radical prostatectomy. Classification of surgical issues: a brand new proposal with analysis in a cohort of 6336 patients and outcomes of surgical procedure. Comprehensive standardized report of problems of retropubic and laparoscopic radical prostatectomy. Prospective evaluation with standardised criteria for postoperative issues after roboticassisted laparoscopic radical prostatectomy. Effect of prostate weight on operative and postoperative outcomes of robotic-assisted laparoscopic prostatectomy. Laparoscopic radical prostatectomy: oncological evaluation after 1000 circumstances at Montsouris Institute. Extraperitoneal laparoscopic radical prostatectomy: A potential evaluation of 600 instances. Oncologic outcomes of laparoscopic radical prostatectomy: Intermediate-term follow-up. Learning curve of laparoscopic radical prostatectomy in a university instructing hospital: Experience after the primary 600 cases. Long-term useful and oncological outcomes after retroperitoneal laparoscopic prostatectomy according to a potential evaluation of 550 patients. Complications, urinary incontinence, and oncologic consequence of a thousand laparoscopic transperitoneal radical prostatectomies � Experience at the Charite Hospital Berlin, Campus Mitte. Risk-adjusted evaluation of optimistic surgical margins following laparoscopic and retropubic radical prostatectomy. Cancer recurrence and survival charges after anatomic radical retropubic prostatectomy for prostate most cancers. Results of radical prostatectomy in males with domestically advanced prostate most cancers: multi institution pooled evaluation. Is preoperative serum prostate-specific antigen stage considerably related to clinical recurrence after radical retropubic prostatectomy for localized prostate cancer Robot-assisted versus pure laparoscopic radical prostatectomy: are there any differences Making ends meet: a value comparison of laparoscopic and open radical retropubic prostatectomy. The new economics of radical prostatectomy: cost comparability of open, laparoscopic and robotic assisted techniques. Ergonomics issues of radical prostatectomy: Physician perspective of open, laparoscopic, and robot-assisted strategies. Anatomic radical retropubic prostatectomy � Long-term recurrencefree survival charges for localized prostate cancer. Cancer management and high quality of life following radical retropubic prostatectomy: Results at 10 years. Long-term consequence following radical prostatectomy in males with medical stageT3 prostate cancer. Prognostic significance of location of positive margins in radical prostatectomy specimens. Oncological and useful outcomes of antegrade radical retropubic prostatectomy for the remedy of clinically localised prostate cancer. Outcome of surgical procedure for medical unilateral T3a prostate most cancers: a single-institutoin experience. A new postoperative predictor of time to urinary continence after laparoscopic 119. Despite tepid help in North America, by the late Nineties, the technique had made its way to a handful of facilities in Europe. Prior historical past of abdominal or inguinal surgery Prior historical past of prostatitis, prostate surgery. The "technical" studying curve is significantly totally different from the "outcomes" learning curve, a concept that has been raised by those excited about seeing the safe and efficient software of this expertise [17]. As Herrel and Smith have reported, the educational curve to cut back positive surgical margins to a stage similar to open radical prostatectomy may take upwards of 150�250 cases [18]. Careful patient choice, nonetheless, may help cut back the slope of the early learning curve associated with the adoption of this process. The surgeon should be particularly cognizant of the challenges of huge prostates and obese sufferers. Large prostates, generally outlined as higher than 50 cm3 on ultrasound, are a challenge because of the confines of the bony pelvis. A caveat that should be thought of is that transrectal ultrasound typically underestimates prostate weight by 20% [19]. For similar reasons, in an obese affected person with a fatty bladder and/or rectosigmoid colon that restricts the working house, imaginative and prescient and ease of dissection could be dramatically impaired. Perioperative care points In order to guarantee both safety and efficiency in the working room, patient positioning should be a course of that involves each member of the surgical team. The anesthesiologist must be made conscious of the steep Trendelenburg positioning that shall be required and some of the nuances of sustaining a patient on this position for long durations of time. The nursing staff should have the ability to facilitate the swift and secure preparation and docking of the affected person cart. The affected person is initially positioned within the supine place, with arms tucked and padded at their side.

Order amantadine 100 mg free shipping
Compared with open surgical procedure hiv infection of monocytes amantadine 100 mg buy cheap, it leads to a faster return of bowel perform hiv infection oral route amantadine 100 mg buy with mastercard, much less 1032 Section 6 Laparoscopy and Robotic Surgery: Laparoscopy and Robotics in Adults Table 85. Size (cm) * 6 Follow-up (months) * 26 Overall survival (%) 50 Disease-free survival (%) 50 Study Moinzadeh et al. Patients with relative or absolute contraindications to laparoscopic surgery ought to be considered for an open surgical process. Larger lesions are additionally technically challenging, partly as a result of they could distort the encircling anatomy. This can lead to misinterpretation of the anatomic landmarks and enhance the propensity in the direction of critical, life-threatening complications. Patients undergoing adrenalectomy for big plenty must also be recommended on the possibility of concurrent en bloc nephrectomy. Different kinds of endocrinologic disorders can lead to disease-specific complications. Patients with Conn syndrome are prone to develop electrolyte abnormalities and require monitoring of blood strain. In patients with pheochromocytoma, close perioperative monitoring of blood strain is essential. To keep away from problems, care ought to be taken throughout creation of the pneumoperitoneum. The Veress needle ought to be positioned in proper place to keep away from harm to the liver, spleen, and intestines. During dissection, caution should be exercised to avoid harm to the encompassing structures such because the bowel and pancreas. When indicated, either a laparoscopic restore or open laparotomy ought to be performed. Vascular issues are essentially the most severe and should contain harm to the adrenal vessels, renal arteries and veins, and the inferior vena cava. Laparoscopic management of a vascular injury could also be attempted with electrocautery or clips. In the postoperative period, early ambulation is inspired to scale back the chance of a deep vein thrombosis. Chapter eighty five Laparoscopic and Robotic Adrenalectomy 1033 In chosen patients, chest physiotherapy is required to forestall lung atelectasis. Postoperative shoulder ache is a standard, though normally a self-limited, complication. Bipolar coagulation may be achieved utilizing conventional electrocoagulators or modern energy-based devices, such because the LigaSure vessel-sealing system (Valleylab) or the ultrasonic coagulator (Harmonic scalpel). Bipolar coagulators can be used for dissection, resulting in less change of instruments. They additionally take away the requirement for particular person dissection and isolation of blood vessels, minimizing avulsion and bleeding. However, the utilization of these instruments is proscribed by blood-vessel caliber and bigger veins is probably not adequately controlled by these units alone. Needlescopic devices are defined as those with a diameter of no more than 3 mm, due to this fact resulting in smaller incision than standard 5�12-mm ports. Besides higher cosmesis, needlescopic surgery may provide the benefit of reduced postoperative ache, hospital stay, and restoration time. It is essential to notice that needlescopic adrenalectomy ought to only be approached by experienced laparoscopic surgeons in rigorously chosen sufferers [32]. This approach preserves a larger hormonal reserve and will keep away from the need for hormonal supplementation following adrenalectomy. These devices enable for a minimal bleeding throughout transection of the adrenal parenchyma. Adrenalectomy is carried out according to the steps of typical transperitoneal adrenalectomy utilizing articulated or bent instruments that let triangulation intracorporeally despite the close proximity of several instruments (dissector, grasper, and scissors) by way of a single port. These instruments embody roticulators (Covidien, 1034 Section 6 Laparoscopy and Robotic Surgery: Laparoscopy and Robotics in Adults extensive laparoscopic expertise. These revolutionary strategies require longer follow-up and more data to assess their oncologic efficacy and perioperative outcomes. Therefore, they should be approached with warning and solely be attempted if the surgeon is confident of adhering to the principles of oncologic surgical procedure. We are currently witnessing a transition from typical open to less and fewer invasive surgical approaches. The paradigm of open surgical procedure for most cancers is being constantly challenged and presently, with maturing laparoscopic expertise, open procedures for adrenal lesions are being replaced by minimally invasive approaches with comparable efficacy. Hemostatic brokers (glues, Surgicel; Ethicon Endo-Surgery Inc) can be utilized for hemostasis when needed. Ablative strategies (radiofrequency/cryo/chemical) Ablative methods represent the new frontier of minimally invasive approaches and provide the benefits of low invasiveness and less technical challenges compared to conventional surgery. These advantages could translate in to decreased morbidity as the process can be carried out on an outpatient basis. Ablation of adrenal neoplasms carries a significant danger of releasing a great amount of hormones rapidly in to the bloodstream. Release of catecholamines can induce arrythmia or hypertension; thus, pretreatment with alpha- and beta-blockade is warranted. Chemical ablation has seen relative success within the management of encapsulated hepatic tumors and has now been applied to adrenal neoplasm. The function of ablation within the therapy of adrenal tumors has yet to be determined and there have been suggestions that its best potential lies within the remedy of recurrent illness, small biochemically active tumors [42], as well as palliative care [43]. Ablative methods have gotten increasingly popular within the urologic subject with intensive primary and medical research endeavors in place. Technologic advances in imaging and exact focusing on of the lesions will probably improve the appeal of those revolutionary approaches. However, till solid consequence data are mature, these techniques should be considered as experimental. Is laparoscopic adrenalectomy possible for adrenocortical carcinoma or metastasis Laparoscopic renal and adrenal surgery in overweight sufferers: comparability to open surgical procedure. This is an advanced laparoscopic procedure and ought to be undertaken only by these with Chapter 85 Laparoscopic and Robotic Adrenalectomy 1035 14. A posterior lumbar method for retroperitoneoscopic adrenalectomy: evaluation of surgical efficacy. Comparison of laparoscopic transabdominal lateral versus posterior retroperitoneal adrenalectomy. Outcomes from 3144 adrenalectomies within the United States: which matters extra, surgeon quantity or specialty Laparoscopic adrenalectomy is superior to an open approach to deal with main hyperaldosteronism. Laparoscopic vs open adrenalectomy for the treatment of main hyperaldosteronism. Robot-assisted laparoscopic adrenalectomy for adrenocortical carcinoma: preliminary report and evaluation of the literature. Robotic-assisted adrenalectomy: what advantages compared to lateral transperitoneal laparoscopic adrenalectomy Clipless and sutureless laparoscopic surgery for adrenal and extra-adrenal tumors. Needlescopic adrenalectomy�the initial collection: comparison with conventional laparoscopic adrenalectomy.
Amantadine 100 mg discount amex
As the dissection progresses towards the inguinal ligament antiviral rna interference in mammalian cells generic amantadine 100 mg visa, the exterior ring is identified and the fats and lymphatics in the space of the wire to the bottom of the penis medially are removed hiv infection common symptoms buy amantadine 100 mg free shipping. The lymph node dissection is sustained for 3�4 cm superior to the inguinal ligament. Once the nodal tissue and fats are faraway from the exterior oblique and the inguinal ligament, the femoral vessels will be identified inside the femoral sheath. To achieve entry to the deep nodes, the fascia lata is opened to the sting of the adductor longus medially and the sartorius muscle laterally. The triangular-shaped lymph packet inside the femoral triangle is carefully removed. Opening the femoral sheath down towards the apex of the triangle will reveal the deep lymph nodes. Care is taken to prevent damage to the femoral nerve by limiting the lateral dissection to the femoral artery. If the pores and skin overlying the exposed vessels appears to be compromised in any means, the sartorius may be mobilized from the anterior superior iliac crest, using ultrasonic or bipolar cautery, and transferred over the uncovered vessels. The lymph node packet could be too large to extract by way of the initial skin incision. In this case the packet may be divided using the bipolar cautery device and extracted in two long strips. We suggest placing the nodes in an extraction sac to decrease the prospect of inadvertent skin contamination. In the case of large specimens, the packet could be divided in to two long strips for extraction. At the end of the process a 7-mm Jackson�Pratt drain is placed contained in the cavity to ensure drainage at the most dependent site of dissection. Once the skin adhesive is dry, a round bandage is placed around the surgical area and held in place with an elastic bandage for twenty-four h. Complications the diagnostic and therapeutic advantages of early inguinal lymphadenectomy must be measured in opposition to the potential morbidity related to the process [7, 8]. Patients ought to be conscious of the minor and major postoperative complications related to this process (Table 78. Prognostic elements of survival: evaluation of tumor nodes and metastasis classification system. Can video endoscopic inguinal lymphadenectomy achieve a Postoperative management the affected person is discharged the day after surgical procedure. Long-term comply with up of penile carcinoma handled with penectomy and bilateral modified inguinal lymphadenectomy. Fortunately, survival rates for males with testicular most cancers are glorious, largely based mostly on a multidisciplinary treatment approach incorporating surgery, radiation and cisplatin-based chemotherapy. With the growing reputation of minimally invasive surgery, surgeons have been expanding the appliance of such approaches to the treatment of extra complicated disease processes. Patients with pN2 or pN3 illness have relapse rates of 50% and due to this fact adjuvant chemotherapy should be strongly considered in these patients [11]. In doing so, ejaculatory perform could be preserved in approximately 95% of males present process this procedure [17]. This method presents the advantage of a bilateral dissection with out compromising ejaculatory perform and has replaced the utilization of template dissections at some facilities. Open conversion rates have proven to be low, with uncontrollable bleeding being the most common purpose for conversion to an open procedure. Mean operative instances vary from 138 to 261 min, with mean size of stay ranging from 1. Such templates decrease dissection in retroperitoneal areas in which metastatic disease would be unlikely. Unilateral templates keep away from dissection below the level of the inferior mesenteric artery, minimizing sympathetic nerve fiber damage in this region. Avoidance of dissection of efferent sympathetic fibers emanating from the contralateral sympathetic trunk additionally reduces the risk of retrograde ejaculation. With further enhancements in surgical method, nerve-sparing techniques have been employed. The 926 Section 6 Laparoscopy and Robotic Surgery: Laparoscopy and Robotics in Adults Table 79. The remaining eight patients had been without proof of illness at a mean follow-up of 37 months [19]. None of the five sufferers was given adjuvant chemotherapy and all were with out recurrence at follow-up intervals of 2�35 months. Additionally, no retroperitoneal recurrences have been famous in sufferers who had pathologically confirmed stage I disease, implying that an adequate dissection was carried out. Viable tumor was present in three (19%) sufferers, of whom two obtained further adjuvant chemotherapy. The first was famous to have an enlarged renal hilar lymph node at his first 3-month postoperative follow-up. The second patient had a retroperitoneal recurrence 11 months postoperatively and finally died of his disease despite salvage chemotherapy. The authors discovered teratoma, necrosis/fibrosis, and energetic tumor in 4, 14, and one patient, respectively. The potential for open conversion either in the setting of intraoperative complication or in depth disease must also be discussed previous to surgery. Some surgeons advocate a low-fat food regimen 1�2 weeks prior to surgical procedure to scale back the chance of chylous ascites; nevertheless, evidence for such an approach is lacking. Patients should be positioned on a transparent liquid food regimen 48 h previous to surgical procedure and endure a mechanical bowel preparation the day previous to surgical procedure. Preoperative antibiotics are given previous to surgical procedure, and antiembolism compression stockings and sequential compression devices are placed on the decrease extremities to reduce deep vein thrombosis. Positioning and port placement General endotracheal anesthesia is required, as the patient must remain paralyzed all through the case. The affected person could be placed in the modified flank (similar to that for laparoscopic nephrectomy) or supine position. A transperitoneal strategy is the popular methodology as a outcome of the bigger and more anatomically acquainted working area for many urologists. The lateral extent of this packet is dissected free to the ureter after which adopted right down to the widespread iliac vessels. This packet can then be clipped and divided on the junction of the iliac vessels and placed in an endoscopic bag. In doing so, the vessel may be grasped on the caval facet and controlled to keep away from hemorrhage.