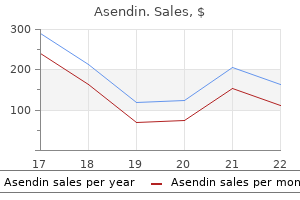
Asendin
Asendin dosages: 50 mg
Asendin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 360 pills

Cheap 50 mg asendin amex
Dissect up the oesophagus to the neck and complete it safely there depression worksheets 50 mg asendin buy overnight delivery, using an acceptable conduit such as a section of colon mood disorders symposium johns hopkins order 50mg asendin with visa. If residual tumour remains on the gastric resection margin the anastomosis could not heal, so that the affected person develops leakage and peritonitis, or quickly develops stomal obstruction from recurrent tumour, or tumour is disseminated extensively during the procedure. As cytotoxic chemotherapy improves, palliative resection could also be of higher worth since some brokers are more practical if the tumour bulk is lowered. Alternatively, the nasal tube could also be passed in to the upper jejunum for feeding functions. In sufferers who discover the tube insupportable, the higher finish could be introduced out in the neck as a pharyngostomy. Ensure that the lung is undamaged and that it may be re-expanded by the anaesthetist if he has deliberately collapsed it. Open a window within the gastrocolic ligament and use a tool such an ultrasonic dissector to coagulate and divide the left gastroepiploic and short gastric arteries. You should protect the right gastroepiploic artery as this would be the primary provide to the stomach remnant. However, the proximal reduce edge should be properly away from progress or the stoma will either leak or subsequently hinder from recurrent development. However, if the tumour may be very extensive it might be extra damaging to carry out gastrectomy than to depart the patient alone. Make certain that the road of proximal part is at least 5�7 cm above detectable disease. Put a stay suture via the jejunal loop and ask an assistant to hold the suture. This will assist you, once you have made the enterotomy and gastrotomy, to place the ends of the stapler in to each opening. Close the remaining defect either with one other linear stapler or using an absorbable suture. It is essential not to burst the tumour in the course of the resection as this will increase the risk of early recurrence. A laparoscopic strategy is commonly employed but tumours within the posterior wall of the stomach are difficult to reach and open access could additionally be higher. In some patients this will lead to dramatic shrinkage of the tumour and reduction of the obstruction. Some tumours that seem to be neoplastic run a benign course and are labelled pseudolymphomas. There may be a mass, a plaque, sessile or pedunculated polyps, or infiltration resembling linitis plastica. Ulcers are irregular and dendritic, sometimes with raised edges, sometimes a number of. Since the lesions are essentially within the submucosa, one of the best diagnostic methodology is deep biopsy. There may be diarrhoea, usually attributed to irritability of the bowel from contact with its high acid content. The syndrome is attributable to a gastrin-secreting tumour of the pancreatic islets which may be benign or malignant, or there may be hyperplasia with out tumour formation (see Chapter 16). The serum gastrin is raised and appears to act as a trophic hormone performing on gastric parietal cells which endure hyperplasia. The gastric fundic mucosa seems hypertrophied and extends virtually to the pylorus, hypersecreting acid in response to the hypergastrinaemia at basal rates approaching maximal acid output. Helicobacter pylori eradication prevents ulcer recurrence after simple closure of duodenal ulcer perforation. Recommendations for requirements of sedation and affected person monitoring during gastrointestinal endoscopy. Recent tendencies in admissions and mortality as a result of peptic ulcer in England: increasing frequency of haemorrhage amongst older subjects. Influence of bursectomy on operative morbidity and mortality after radical gastrectomy for gastric cancer: results of a randomized controlled trial. Laparoscopic surgical procedure for gastric most cancers: a collective review with meta-analysis of randomized trials. Risk components related to operative mortality and morbidity in patients undergoing emergency gastrectomy. The suspicion is confirmed when very excessive basal levels of acid output are measured and maximal pentagastrin stimulation has little or no added effect. In case of doubt, carry out calcium stimulation check (5 mg/kg/hour infused for three hours) or a secretin challenge (4 units/kg intravenously). [newline]If a solitary tumour is found in the head of the pancreas within the absence of metastases, enucleate it. If a tumour is discovered in the physique or tail of the pancreas, excise the body and tail. If no tumour is discovered in the pancreas, duodenum or elsewhere, excise the physique and tail of the pancreas for histological exclusion of hyperplasia. Acquired diverticula might affect the duodenum, jejunum and to a lesser extent the ileum, and are frequently multiple. Affected segments of bowel are infected, thickened and narrowed, and infrequently lined with fibrinous exudate. The mesentery is thickened and the mesenteric fats typically extends over the serosa of the bowel in the course of the anti-mesenteric border (fat wrapping). Tuberculous and Yersinial infection can produce similar adjustments of ileitis; if doubtful remove a lymph node for bacteriological and histological examination. The diagnosis is indicated by dilatation of subserous and mesenteric lymphatics, thinning and pigmentation of the bowel wall and splenic atrophy. Severe refractory coeliac illness may trigger ulcerative jejunitis and predispose to small bowel lymphoma. Small-bowel ulcers and strictures might happen spontaneously, follow radiotherapy or transient strangulation in an exterior hernia or after the ingestion of potassium tablets. The return of a shiny, pink appearance, pulsation of the mesenteric vessels and peristalsis throughout the affected phase point out viability. The remaining small bowel, which has a mesentery, is variable in total size (about 3�5 m) and tough to measure with accuracy in vivo. It is arbitrarily divided in to a proximal 40%, the jejunum (Latin: jejunus � hungry, empty), and a distal 60%, the ileum (Greek: eilios � twisted). On palpation the jejunal wall is thicker than that of the ileum, so that the analyzing fingers gain the impression of a double layer, rather like feeling a shirt through the sleeve of a jacket. Pick up the small bowel on the duodenojejunal flexure and feed it via your fingers all the means down to the ileocaecal valve. Note the diameter and contents of the bowel and the thickness and colour of its wall.
Generic 50mg asendin free shipping
Influenza B is classified in to two distinct lineages Yamagata and Victoria but not in to subtypes organic depression definition asendin 50 mg on-line. Avian H5Nl commonly referred as bird flu is a highly pathogenic strain of influenza virus that infects and kills humans in shut contact with diseased birds but has not acquired pandemic potential because of depression test german asendin 50 mg buy low cost restricted human to human transmissibility. The currently circulating influenza virus strains are H3N2, pandemic HlNl and influenza B. Influenza is transmitted from person-to-person via airborne droplet unfold or through contact. The portal of entry is the respiratory tract and the virus attaches itself to the respiratory epithelium by way of the hemagglutinin which is the principle virulence issue. The incubation interval is 1-3 days and the period of infectivity is often 7 days after sickness onset and sometimes longer in these with severe illness. It has been estimated that the novel HlNl pandemic brought on 18,000 deaths globally with case fatality charges starting from 0. Hence if specific remedy has to be administered, it has to be began before outcomes turn into obtainable. In many instances, the report of the throat swab is obtained when the patient has already recovered. Henceforth molecular analysis of influenza should be restricted to hospitalized sufferers with severe disease when a definitive prognosis helps in tracking the severity of the outbreak. Clinical Features In most people influenza is a minor sickness characterized by a combination of fever, runny nose, sore throat, cough, bodyache, headache, abdominal ache, diarrhea and vomiting. The danger of issues is higher at extremes of age (children below 2 and the elderly), pregnant ladies and these that have simply delivered, those with underlying comorbidities corresponding to any chronic neurologic, metabolic, cardiac, pulmonary or renal illness, those that are immunocompromised and those with extreme bronchial asthma. In the novel HlNl epidemic the aged had been spared as a result of pre-existent immunity and morbid weight problems emerged as an important risk issue. The m ost dreaded complication of influenza is pneumonia with acute respiratory distress syndrome, respiratory failure and generally shock and renal failure. Progression may be very rapid and most sufferers require ventilator help over the next 24 hr. Occasionally other complications similar to encephalitis, seizures, quadriparesis and myocarditis have been reported. Transplacental transmission to new child and neonatal issues have also been reported. The pandemic HlNl pressure and most current seasonal flu strains are immune to the M2 inhibitors. Hence as per current recommendations oseltamivir is the primary line drug and zanamivir ought to be used in these with oseltamivir resistant virus. The therapeutic dose of oseltamivir is 30 mg twice daily in those with weight less than 15 kg, forty five mg twice every day for 15-24 kg, 60 mg twice every day for 25-34 kg and 75 mg twice daily for those 35 kg and above. In patients with very severe illness double the really helpful dose for 10 days could additionally be used. Patients must be counseled in regards to the pink flag signs and asked to search medical care within the occasion these happen. These defervescence, breathlessness, dyspnea, tachypnea, hemoptysis in older youngsters and adolescents, excessive weak spot, poor oral consumption and altered sensorium. The use of antivirals in all children under the age of 5 with flu like sickness is nevertheless deba table. In patients with indicators of lower respiratory involvement, antibiotics like coamoxiclav or cephalosporins (cefuroxime, ceftriaxone or cefpodoxime) also needs to be used as bacterial coinfections are common. Emerging Viruses 239 this section deals briefly with a few of the new rising viral ailments seen in India. Prevention Vaccination is the best preventive strategy and is mentioned further in Chapter 9. The dose is 30-75 mg of oseltamivir (as per weight) to be taken once day by day for 10 days. It should be remembered that chemoprophylaxis is the most important risk issue for drug resistance. Chemoprophylaxis ought to be thought of only for very high-risk family contacts like pregnant ladies and the severely immunocompromised. Household transmission could be reduced by good air flow within the room, proper hand hygiene and adherence to cough etiquettes. Vaccination for all health care workers especially during outbreaks must be thought-about. A distance of a minimum of 1 m must be stored between sufferers because the droplets can travel for this distance solely. The workers caring for these patients should use a properly fitting surgical mask that should be modified every 4 hr. Negative strain rooms, N ninety five masks, gowns although ideal are attainable solely in high useful resource settings. School children show one of many highest infection rates and outbreaks are widespread in class. For lowering transmission, the school rooms should be well ventilated, youngsters should be trained in hand hygiene and cough etiquettes and sick children should be prohibited from attending college until afebrile. The presentation is that of a viral hemorrhagic fever with fever, body pain, headache, profuse bleeding, leukopenia, thrombocytopenia, altered liver functions, deranged coagulation parameters, rhabdomyolysis and renal failure. The disease mimics dengue with salient differences being early and extra fast platelet fall and rhabdomyolysis. Strict isolation of affected patients is essential to forestall nosocomial transmission. Rodents are pure hosts and people purchase infection by inhalation of aerosols contaminated by rodent excreta or saliva. The disease presents as a febrile illness with physique pain, headache, thrombocytopenia, elevated liver enzymes, bleeding and renal failure. Nipah virus is a crucial reason for encephalitis increasingly reported from West Bengal, India. Its pure asymptomatic hosts are fruit bats who can transmit infection and illness to pigs and people. Clinical features in people are fever adopted by options of encephalitis and sometimes pneumonia and respiratory misery. Prevention facilities around limiting human publicity to raw date palm juice contaminated by fruit bat excreta and infected pigs. Chandipura virus, a rhabdovirus, is implicated as a explanation for epidemic viral encephalitis in kids in a number of states in India however not overseas. It is transmitted by chunk of contaminated sandflies and is associated with high mortality and neurologic sequelae. A arge outbreak of acute encephalitis with excessive fatality fee in kids in Andhra Pradesh, India, in 2003, associated with Chandipura virus. Etlopathogenesls Staphylococci are functionally categorised on foundation of production of an enzyme and virulence issue coagulase. Staphylococcal infection is acquired normally by direct contact with an infected patient or carrier and sometimes contaminated objects.
50mg asendin purchase overnight delivery
The strategies for reaching this aim are: Attaining excessive rntes of routine immunization great depression definition quizlet discount asendin 50 mg overnight delivery. When poliovirus transmission is decreased to well-defined and focal geographic areas depression symptoms shaking asendin 50 mg order on line, intensive house-to-house, child-to-child immunization campaigns are carried out over a interval of days to break the final chains of virus transmission. Other circumstances with a presentation similar to those of paralytic poliomyelitis embrace traumatic neuritis and less fre quently, meningitis, encephalitis and diseases produced by toxins (diphtheria, botulism) (see Chapter 19). Treatment Treatment ought to be early and acceptable to the stage and diploma of paralysis. Children with bulbospinal polio and respiratory paralysis require hospitalization. In the acute stage, kids with isolated paralysis of a quantity of limbs could be managed at residence. They should be suggested complete relaxation, proper positioning of the affected limb and passive range of movement on the joints. Massage and intra muscular injection must be averted throughout acute part of sickness. The child should be made to lie on a agency mattress and keep limbs in impartial position. Warm moist fomentations could be given with delicate towels, dipped in heat water to relieve pain and spasms. This helps to stimulate proprioceptive impulses from muscles and tendons, helping improve muscle power. As the acute part of sickness subsides, recovery in muscle power is helped by giving physiotherapy, helping ambulation and prevention of deformities. Prevention of Poliomyelitis the out there vaccines and the really helpful schedule are mentioned in Chapter 9. Hand-Foot-Mouth Disease Hand-foot-mouth illness is a typical viral illness primarily affecting children beneath 5 yr. The most typical causes of hand foot mouth illness are coxsackie virus A16 and enterovirus 71. The illness often presents as outbreaks, typically in preschool youngsters and transmission is by direct contact with an affected patient or infected fomites. Hepatitis A and E are liable for many of the water-borne (community acquired) hepatitis whereas B, C and D are answerable for post-transfusion hepatitis. Hence, it spreads readily by the feco-oral route by way of contaminated meals and water and from person-to-person living with poor sanitation. Symptomatic illness is unusual and outbreaks uncommon in creating countries with poor hygiene since most people are contaminated in childhood. In regions with intermediate endemicity like India, a big proportion of people escapes infection in childhood and should develop symptomatic disease as adults. Clinical Features the onset is with a prodrome characterised by low grade fever, feeling of being unwell and sore throat. This is followed by growth of ulcers or blisters in the oral cavity, totally on the posterior facet and then a papulovesicular pores and skin rash on the palms and soles and less commonly, on buttocks, knees, elbows and genital area. Complications include momentary loss of toe nails or finger nails about 4 weeks after onset of disease. Rare complications embody aseptic meningitis, encephalitis, polio like paralysis, myocarditis and respiratory misery syndrome. Outbreaks, particularly as a outcome of enterovirus 71, are reported from China, Vietnam, Taiwan and Malaysia, during which neurologic problems are common and mortality vital. Some specialists consider that entero viruses trigger hand-foot-mouth disease now occupy the ecologic area of interest vacated by eradication of polioviruses. Diagnosis is clinical and requires differentiation from different diseases inflicting oral ulcers like herpangina, herpetic gingivostomatitis and aphthous ulcers and from chicken pox. Treatment and Prevention Treatment is especially symptomatic and includes analgesics and soft food plan. Isolation of affected kids at residence and promotion of hand hygiene to prevent illness spread is necessary. This is followed by a brief prodromal part lasting up to a week, which is characterized by lack of appetite, fatigue, abdominal pain, nausea and vomiting, fever, diarrhea, darkish urine and pale stools. In this case, excessive fever, marked belly pain, vomiting, jaundice and the development of hepatic encephalopathy associated with coma and seizures happen. In sufferers who survive, neither functional nor pathologic sequelae are widespread regardless of the widespread necrosis. Its titer increases over 4-6 weeks, then declines to nondetectable levels within 6 months of infection. Laboratory evaluation of liver operate includes estimation of complete and direct bilirubin, transaminases, alkaline phosphatase, prothrombin time, whole protein and albumin. Referral to a liver transplant middle is acceptable for patients with fulminant hepatitis. Acute hepatitis is marked by signs much like different acute hepatitis diseases, i. Fulminant hepatitis is heralded by pathologic mental standing modifications inside 2 to 8 weeks after the preliminary symptoms in an otherwise healthy child. Although liver damage is normally gentle throughout childhood, severe sequelae, including cirrhosis and hepatocellular carcinoma, may develop insidiously at any age. If adminis tered inside two weeks of exposure it both prevents development of illness or reduces its severity. Epidemiological transition of hepatitis A in India: issues for vaccination in growing nations. In areas of low endemicity, horizontal an infection is the principle route of transmission. During the early section of infection, the amount of virus within the liver and blood is normally massive, whereas the liver injury is usually mild. The host immune system gradually recognizes the virus and begins to clear the virus. It results in active irritation of the liver and elevation of serum aminotransferases. Interferons are a group of naturally occurring brokers with antiviral, antineoplastic and immunomodulatory properties. Lamivudine monotherapy for 1 yr offers satisfactory leads to kids with chronic hepatitis B. The medication is well tolerated, has minimal unwanted side effects and is simple to administer. The viral genotypic distribution in children usually parallels that reported regionally in adults. Enzyme immunoassay is limited by frequent false-positive outcomes, particularly in patients with elevated globulin ranges such as these with autoimmune hepatitis. Longer-acting pegylated inter ferons have been subsequently developed based mostly on the premise that extra sustained drug levels would end in higher antiviral exercise. Importantly, biochemical and virologic responses have been accompanied by significant histologic enchancment in all handled patients included in these trials, and interferon has been properly tolerated in kids.
Purchase 50 mg asendin with visa
It is necessary to create a spout that may discharge its irritative contents properly clear of the skin depression on period cheap 50 mg asendin fast delivery. In comparability with transverse colostomy depression test elderly 50 mg asendin cheap fast delivery, it produces predictable volumes of relatively inoffensive faecal effluent and is actually a defunctioning stoma to which an equipment can simply be connected. Split ileostomy, with separated stomas, fully defunctions the distal bowel and has been advocated in chosen instances of colitis. Split enterostomy has also been advocated to shield a decrease enteric anastomosis created within the presence of peritonitis. The distal reduce finish is both exteriorized as a mucous fistula or oversewn and glued to the parietal peritoneum to facilitate later retrieval. The 9Fr Feeding jejunostomy tube is brought out through the belly wall and the jejunum is stitched to the peritoneum around the tube. Make a transverse incision within the uncovered anterior rectus sheath, split the fibres of the rectus muscle and open the posterior sheath and peritoneum. Now exteriorize 6�8 cm of bowel, with its mesentery intact, through the round opening within the belly wall, leaving its end securely clamped. Make sure that the mesentery is neither twisted nor tight and that the tip of the ileum stays pink. Mucosa stitched to pores and skin Ileum stitched to aponeurosis Muscle Skin Peritoneum Tissue forceps Action 1 n Expose the upper jejunum, either laparoscopically or through a 3 n Some surgeons close the lateral space between the ileostomy and Feeding jejunostomy 2 n Insert a Vicryl purse-string suture on the antimesenteric border of the bowel. Make a tiny enterotomy in the centre of the pursestring and introduce a 9Fr feeding jejunostomy tube in to the lumen of the bowel. Take additional care when fashioning an ileostomy to cut back the incidence of these problems. Extraperitoneal course of ileum Purse-string suture closing lateral area Subcutaneous tissue 196. Two strategies of closing the lateral area are proven: a purse-string suture or taking the ileum along an extraperitoneal observe. Tissue forceps on each layer of the wound edge forestall retraction of the layers whereas the ileostomy is being fashioned. Now suture the edge of the ileum directly to the pores and skin, utilizing Vicryl mounted on a taper-cutting needle. Complete the circumferential sutures, producing a spout, which ought to project about 3 cm from the belly wall. Depending on the size of its mouth, the diverticulum can simply be transected across the neck using a linear stapler or excised with a portion of the antimesenteric border of the bowel. Local resection of the ileum with endto-end anastomosis could also be preferable in an advanced case. Attach an appropriate appliance, with flange and clip-on bag, to the skin over the stoma. Starting at the apex, squeeze the intussusceptum again along the intussuscipiens as if extracting toothpaste from the underside of the tube. Besides confirming the analysis, barium enema may cut back the intussusception completely or subtotally. Feed could start at 30 ml per hour on the primary postoperative day and be constructed up incrementally. The effluent might be very unfastened at first, but will steadily thicken as the ileum adapts. Consult the stomatherapist instantly, if she or he has not already seen the patient before operation. Make sure that the patient is competent and confident at managing the stoma before he leaves hospital. Deliver the affected segment from the stomach and gently compress it with a moist swab, earlier than resuming the squeeze. Increase oral fluids when the stoma commences to dis- 1 n Intussusception is rare and is type of all the time related to an un2 n Reduce the intussusception as far as potential then proceed to native resection of the affected segment of bowel with end-to-end anastomosis. Thrombosis might occur on arteriosclerotic plaques on the origin of the superior mesenteric artery, particularly if the patient is shocked. The superior mesenteric artery is an unusual website for peripheral embolism in sufferers with cardiac arrhythmia or a current myocardial infarction. Venous gangrene may result if the superior mesenteric or portal veins all of a sudden undergo thrombosis, for instance in extreme dehydration or disseminated intravascular coagulation. Lastly, non-occlusive mesenteric infarction could happen secondary to microcirculatory harm in critically sick patients. Although the diagnosis could also be troublesome to make, suspect it if unexplained lactic acidosis develops in a postoperative or critically ill patient. A retrospective analysis1 discovered that the probabilities of manufacturing surgical morbidity and mortality in the grownup inhabitants had been far higher when resecting incidental diverticula. Recovery is unlikely if the entire midgut is infarcted following occlusion of the superior mesenteric artery. If an in depth phase is affected, be as conservative as possible to avoid extreme short-bowel syndrome. Examine the aorta and its primary divisions to determine the extent of atherosclerosis. If the main intestinal vessels and their arcades are patent, the circulation is probably occluded at capillary degree. Take care to divide any adhesions that would partially hinder the distal intestine and result in recurrence of the fistula. It is much simpler to mobilize the caecum and establish the ileocolic artery than to expose the origin of the superior mesenteric artery itself. Pass a Fogarty catheter proximally in to the superior mesenteric artery and aorta to dislodge the clot, and attempt to set up free circulate. If the bowel regains its regular color, shut the arteriotomy with a venous patch. Otherwise think about side-to-side anastomosis between the ileocolic and proper common iliac arteries. The vast majority of exterior fistulas arise either from a leaking anastomosis or from operative damage to the intestine. Switch to complete parenteral vitamin which will scale back the amount of fistula discharge. There is some evidence that Octreotide one hundred fifty mg tds may scale back the time for fistulae to heal. Thereafter, by alternately using two atraumatic graspers, expose the entire length of the small bowel to the caecum, dividing any intervening adhesions with laparoscopic scissors. Laparoscopic examination of the bowel is helpful in determining whether or not bowel is viable or not. Diagnostic laparoscopy is secure and can be performed with minimal morbidity and mortality. It is especially useful in critically sick sufferers in whom you want to keep away from pointless laparotomy.
Cheap 50 mg asendin with visa
Transect the duodenum simply above the distal Payr clamp depression definition wikipedia buy asendin 50 mg without a prescription, guaranteeing that no gastric mucosa remains attached to the duodenum mood disorder teenager asendin 50 mg on-line. Divide the lesser omentum proximally, if attainable preserving an accessory hepatic artery if one is present. If the resection line cuts through tumour, the anastomotic line might break down throughout recovery from the operation. Activate the stapling device to staple and seal the duodenum and transect this with a scalpel utilized intently to the higher fringe of the stapler. It is sensible to invaginate and reinforce the everted staple line with a layer of sutures. Place a protracted straight stapling device across the abdomen on the proposed line of section and cut off the distal gastric specimen with a scalpel run alongside the distal edge of the stapler. Make a stab wound within the larger curve aspect of the posterior wall of the stomach 2 cm proximal to the staple line and an identical stab wound within the jejunum on the origin of the efferent loop. Cut midway throughout the stomach simply distal to the Payr clamp, transecting the lesser curve half of the abdomen. Oversew the clamp and contained crushed abdomen edge with a operating loose spiral stitch. This manoeuvre leaves just the larger curve half of the stomach to be united to a matched gap made in the jejunum. The anastomosis is accomplished in an analogous method to the creation of a fullwidth stoma. Four lines of staples could have united stomach to jejunum and the knife will have reduce a stoma between the centre rows of staples. Place tissue forceps on the ends of the inside and outer staple strains and separate the forceps to create an everted linear defect in the anastomosis. Place a short straight stapler across the everted lips of the defect, tighten and actuate it. Cut off the surplus tissue, take away the stapler and examine the road of closure rigorously, if needed reinforcing the entire anastomosis all round with sutures. Technical factors 1 n the within of the stomach and bowel are colonized with microorganisms. While fashioning anastomoses, isolate the interior of the bowel from the peritoneal cavity and wound edges by using separate towels, instruments and gloves. When the bowel is repaired, discard and exchange them with sterile gloves, towels and devices. Reach down and ach 2 cm above the proposed line of transection, from larger to lesser curve. Place a protracted non-crushing clamp throughout the stomach three cm distal to the twin clamp and parallel to it. Draw as a lot as the abdomen the first loop of jejunum, with afferent loop to lesser curve with no slack but not tight. Place the second of the dual clamps throughout this loop of bowel, occluding only the lumen and never the mesentery. Continue the all-coats stitch round on to the anterior wall and alongside it to completely encircle the anastomosis. Complete the seromuscular suture line on to the anterior wall to encircle the anastomosis. The antecolic valved gastrojejunal anastomosis, with afferent loop joined to lesser curve, is complete. The spleen could additionally be adherent to the diaphragm and the costal margin could additionally be narrow in an overweight affected person. In time of difficulty be sure that the sunshine, the exposure and the help are all optimal. Control severe bleeding with local strain whereas getting ready to decide up the bleeding level precisely with artery forceps. If the splenic capsule is torn, attempt to preserve the spleen by suture restore or packing with Surgicel. Splenectomy is undesirable because of the thrombotic, infective and immunological problems (but see Chapter 18). It may be troublesome and unsafe to dissect out and close the duodenum in the presence of in depth scarring and distortion from continual severe duodenal ulceration. The best choice is to rigorously pinch off the duodenum simply at the distal ulcer edge and carefully mobilize a adequate cuff of duodenum beyond to close safely, leaving the ulcer crater undisturbed. The second choice is to go away the duodenum attached to the ulcer and mobilize the anterolateral duodenal wall so that it can be sewn right down to the distal fibrotic edge of the ulcer crater, thus closing off the duodenum. Leave it connected to a closed drainage system for 10 days and, if the affected person is properly, progressively withdraw it. Its administration is finest carried out by skilled clinicians, endoscopists and surgeons acting as a group. Dedicated models obtain much better survival than these enterprise it as part of a common service. Aspirate all the blood from underneath the left cupola four n Make certain the duodenal stump is safely closed. Check the haemoglobin and haematocrit, and exclude clotting deficiencies if suspected. Remember that mortality is highest among the over-60s, these with large haemorrhage and shock, and those with critical associated disease. Access Make a generous higher stomach midline incision skirting the umbilicus, 20�25 cm long. Look for persevering with bleeding and the presence of seen vessels which indicate that the bleeding is likely to continue or recur. Haemostatic substances may be injected in association with local software of warmth. Assess 1 n As the abdomen is opened, blood which appears bluish through the bowel wall could also be seen in the small or large bowel. Dilated and congested veins on the viscera with a stiff cirrhotic liver make portal venous hypertension obvious. Therefore carry out a radical check of the decrease oesophagus, stomach and duodenum, remembering that there may be an unsuspected lesion within the small or large bowel. It could also be valuable first to have a large-bore gastric tube handed in order that the abdomen may be washed out if it incorporates blood or retained food. In applicable circumstances the radiologist might be able to embolize the feeding vessel. This makes it harmful to defer operation if bleeding is critical and never controllable.
Purchase asendin 50 mg overnight delivery
A lateral image of the pelvis should be obtained to outline whether the rectal pouch is above or below a line drawn from the pubis to the coccyx online depression test best 50mg asendin. A cleft of the taste bud could be simply missed until the child is examined carefully anxiety 8 year old asendin 50 mg generic without a prescription. In Pierre-Robin syndrome, cleft palate is related to retracted jaw (micrognathia) and huge tongue, with a tendency for glossoptosis. Bottle feeding may be tried with a soft nipple with rubber flange, which shut the cleft and help the baby in sucking. Diaphragmatic Hernia Diaphragmatic hernia happens due to failure of closure of the pleuroperitoneal membrane. This allows intestinal loops to ascend to the thorax that compress the growing lung and can end result in pulmonary hypoplasia. It requires careful consideration to important parameters, temperature and blood glucose levels as well as coordination with the receiving hospital. Counsel the parents and family before transport Communicate with referral facility. However, if referral of a neonate is unavoidable, efforts should be made to do the greatest possible job. Take the baby to the nearest referral facility (inform them in advance on cellphone or otherwise), by the shortest route, using the quickest attainable and reasonably priced mode of transport. The amount, dilution and mode of feeding ought to be famous if supplemental feeding is given. If poor weight gain persists regardless of all measures to improve breast milk output supple mentation can be thought of. Initially, semisolids must be suggested in accordance with the local cultural practices. Growth monitoring: Growth (including weight, head circumference, mid-arm circumference and length) should be monitored and plotted on an acceptable progress chart at each visit. Developmental assessment: Assessment of developmental milestones must be carried out in accordance with the corrected age. The milestones must be assessed in four domains - gross motor, nice motor, language and personal-social. Ongoing problems: Ongoing morbidities similar to diarrhea, pneumonia occur more incessantly in these babies and will require acceptable therapy. Neurological assessment: Muscle tone should be assessed, any asymmetry between the extremities should also be recorded. Eye evaluation: An ophthalmologist ought to evaluate the child for imaginative and prescient, squint, cataract and optic atrophy. Subjective visual evaluation could be made from medical clues as lack of ability to fixate eyes, roving eye actions and nystagmus. Hearing evaluation: High danger infants have higher incidence of average to profound listening to loss (2. These infants must be screened for hypoglycemia at 2, 6, 12, 24, forty eight and seventy two hr after start with reagent strips (dextrostix). The symptoms when present could also be of neuromuscular irritability: myoclonic jerks, jitteriness, exaggerated startle and seizures. Adequacy of breastfeeding must be assessed and small babies not in a position to suck successfully on the breast, ought to receive expressed breast milk by alternate strategies. The clinician should evaluate each medicine fastidiously, look at published information on the drug and advise the mother rigorously about the usage of drugs while breastfeeding. Maternal Medications and Fetal Hazards the danger by exogenous brokers to the fetus is most pronounced through the interval of embryogenesis and may result in abortion or congenital malformation. In the late part of being pregnant, these brokers solely cause organ dysfunction or disturbances of enzyme methods. The benefits of medicine to the mom should at all times be carefully weighed against the risk to the fetus. Early onset neonatal hypocalcemia: Commonly seen in preterms less than 32 weeks, infants of diabetic moms, perinatal asphyxia and maternal hyperparathyroidism. Late onset hypocalcemia: Neonates born to mothers with vitamin D deficiency, infants on anticonvulsant remedy or with malabsorption, those on cow milk feeding, or with hypoparathyroidism are vulnerable to late onset hypocalcemia. Clinical Presentation Early onset hypocalcemia is usually asymptomatic unlike the late onset hypocalcemia variety and is identified on Newborn Infants Table eight. Excess maternal glucose and amino acids provide the substrate for elevated synthesis of protein, lipids and glycogen in the fetus. Since insulin blocks induction of enzyme system, this will likely clarify lower manufacturing of surfactant. Reduced surfactant pool and the upper risk of preterm deliveries explains higher danger of respiratory misery syndrome in these babies. The following problems are prone to occur throughout pregnancy of a diabetic mother. Polycythemia, increased viscosity of blood and hyperbilirubinemia Management the infant must be screened for malformations and injuries. The neonate should be monitored for blood glucose ranges throughout first three days of life. The other morbidities corresponding to respiratory distress, hyerbilirubinemia should treated appropriately. Neonate ought to be screened for hypothyroidism utilizing either cord blood or on blood sample taken after seventy two hr of start. Note the massive size of the child with broad shoulders and torso and a relatively smaller head Tuberculosis If the mom has lively pulmonary tuberculosis that has been treated for less than 2 months before start or the prognosis of tuberculosis was made after delivery, the infant is in danger to purchase an infection from the mom. The toddler should be followed up in 4 weeks to examine the infant for growth and signs of congenital syphilis. Such infants should obtain hepatitis B vaccine inside 12 hr of start, which may stop perinatal transmission of hepatitis B virus considerably. Breastfeeding ought to then stop as quickly as a nutritionally adequate and safe food regimen without breast milk can be provided. There are two main elements of immunity: the innate immune sys tem and the adaptive immune response. Innate immunity is primitive, nonspecific, has no reminiscence and offers the primary line of defense in opposition to infections, while the adaptive immune system is extremely advanced, particular and has reminiscence, characterized by a fast rise in immune response when exposed once more to the microorganism. Innate Immune System the skin and mucous membranes provide an important mechanical barrier to an infection. Gastric acidity is an efficient physiologic barrier as only a few microorganisms can survive the low acidic pH in stomach. The complement system consists of multiple serum proteins circulating as inactive precursors.
Diseases
- Antisynthetase syndrome
- Cancer
- Acromesomelic dysplasia Brahimi Bacha type
- Microphthalmia microtia fetal akinesia
- Rutledge Friedman Harrod syndrome
- Oculopharyngeal muscular dystrophy
- Marden Walker syndrome
- Chemodectoma
- Epidermolysis bullosa, pretibial
- X-linked mental retardation type Martinez
Generic asendin 50mg without prescription
Once the stomach is opened depression symptoms boredom asendin 50mg sale, gently retract the stomach wall and divide any adhesions by blunt and sharp dissection anxiety physical symptoms 50 mg asendin cheap with mastercard, making use of tactile sensation and direct vision. If needed, change position or facet to get a greater view of the adherent buildings earlier than dissecting them out safely. However, exploration is still necessary in emergencies affecting the stomach where a transparent prognosis may not be obtainable because of the emergent nature and need to function without thorough investigation. Knowledge of exploratory laparotomy is, therefore, nonetheless important, particularly for surgeons in coaching. Prevention of adhesions 1 n Meticulous haemostasis, prevention of intra-peritoneal spillage of intestinal contents, minimal dealing with of bowel, use of powderfree gloves, glove cleansing using a 10% solution of povidoneiodine in a non-toxic detergent base and not closing the peritoneum have all been advocated to forestall adhesion formation. However, the incidence of intra-abdominal abscesses and anastomotic leaks was greater within the Seprafilm group compared to controls. A cheaper various is liberal irrigation with Ringer lactate solution, which has been reported to decrease adhesions in experimental animal fashions. However, such situations have gotten increasingly uncommon: one such example is small-bowel tumours, which had been traditionally confirmed at laparotomy however can now be identified on capsule endoscopy. Patients with recurrent adhesive small-bowel obstruction profit from adhesiolysis and restoration of the bowel anatomy. A cautious examination carried out with the stomach relaxed and a trial of native anaesthetic could assist. The features may change and at occasions you may make the choice to defer operation. Improvements in diagnostic Access 1 n the ideas governing incisions have been addressed firstly of this chapter and will be re-addressed in chapters dedicated to the relevant organs. Small-bowel, colon Pelvic viscera, lower ureter (extraperitoneal) Liver and biliary tract (right), spleen (left) Pancreas, liver, adrenals. The Goligher, Bookwalter order to cope with sudden findings or intra-operative difficulties. Proper and liberal use of retractors frees an assistant to be utilized in different essential steps. Tilt the patient away from the world of interest so that bowel falls away, giving a greater publicity. This is particularly necessary in laparoscopic surgery where a tilt of about 20 levels can make a fantastic difference. Lanz Pfannenstiel Thoraco-abdominal Right Left Assess 1 n Have the theatre nurse clear all unnecessary instruments from the 2 n Carry out a systematic examination of the stomach and its conoperative subject. It is really helpful that a set sequence is adopted in analyzing the abdominal viscera in order that no structure is missed. Whatever course you undertake, meticulously record the findings in the operation notes. Visceral contents which are usually sterile similar to bile, urine and gastric juice may turn into infected because of inflammation and obstruction. Before opening the bowel or different doubtlessly contaminated viscera, isolate the area from contact with the wound and other organs by using moist stomach swabs. Apply non-crushing clamps to occlude the lumen and ensure that an efficient suction apparatus is on the market to take away any contents that spill. Following closure of the viscus discard all devices and swabs used on opened bowel and alter gloves. It is, nonetheless, helpful to know the forms of bowel clamp and when they need to be used. Use the minimal variety of devices and the largest swabs, which ought to stay connected to massive clips mendacity outdoors the abdominal wound. Note the character and quantity of any free fluid, amassing some for chemical, cytological and microbiological examination. You might be able to dictate the findings to an observer for direct entry in to the operation notes. In situations the place further exploration of the stomach is futile, similar to in carcinomatosis peritonei, make a delicate seek for the first tumour and biopsy any seen metastatic lesions. Perform a palliative procedure similar to a stoma or entero-enteric bypass if essential. In elderly or sick patients control of the emergency condition takes precedence over the complete eradication of disease. If potential, use long-handled instruments on tissues and structures when extended use is anticipated. Although the first accountability of leaving a swab or an instrument in the stomach rests with you because the working surgeon, encourage the complete staff to take an active role in preventing it. The scrub nurse counts the instruments and swabs earlier than the process and before closure of the operative wound. He or she also counts any additional instruments, needles or swabs used during the process. If the scrub nurse reports a missing swab or instrument while closing the abdomen, perform a thorough search of the stomach and vicinity. If all else fails, perform an abdominal X-ray before waking the patient from the anaesthetic. Bacteria might enter from exterior through an open drain, particularly if nursing care is poor, or the drain might erode a vessel or a suture line, particularly whether it is left in for a very long time. When you have to use a drain it ought to be a closed drain, and if suction is to be used make use of a low-pressure system. Nonetheless, spillage of contaminated contents, such as faeces or infected bile, might lead to early septicaemia and late belly abscess. Place one drainage tube within the abscess cavity and one within the pelvis: gentle, wide-bore silicone tubes or sump drains are applicable. Irrigate with warmed (37 C) peritoneal dialysis fluid (Dialaflex 6 L) with added potassium at a rate of 50�200 ml/hour, relying on the extent of sepsis. A water-tight closure of the belly wound is crucial, so initially perfuse a small amount of dialysate (50 mL/hour) overnight until the peritoneum seals any defects. In the presence of threat components for poor therapeutic corresponding to a distended or overweight stomach; if the wound is infected or prone to turn into so; if the patient is malnourished, jaundiced or suffering from superior most cancers, consider using these sutures. When half the size of the wound is approximated, commence suturing from the opposite finish and tie the two sutured segments in the middle with a safe knot. This layer is usually not approximated but when it is extremely thick, 2/0 or 3/0 polyglactin (Vicryl) interrupted sutures may be used to obliterate the potential dead space. An inverted suture, beginning and ending in the depth of the wound buries the knot, giving a better end result. When the wound is contaminated, use staples or interrupted non-absorbable sutures such as 3/0 nylon or polypropylene.
50mg asendin with amex
Radionuclide Imaging Imaging of the kidney and urinary tract has been simplified by radionuclide methods anxiety or asthma discount 50mg asendin mastercard, which have changed conventional radiocontrast studies mood disorder with psychotic features code asendin 50mg buy fast delivery. Radionuclide procedures are noninvasive, extremely delicate and expose sufferers to much less radiation in comparison with radiocontrast studies. This is beneficial in detection and followup of renal parenchymal defects related to urinary tract infections. This impact is accentuated by administration of angiotensin converting enzyme inhibitors, thus rising its sensitivity in analysis of renal artery stenosis. Radionuclide cystography is sensitive for detecting vesicoureteric reflux with minimal radiation publicity. Diagnostic Evaluation A history of pain in the flank or suprapubic area, dysuria and edema must be obtained. Physical examination contains evaluation of progress and options of acute or chronic kidney disease similar to edema, hypertension, unexplained pallor, bony abnormalities and belly mass. In glomerular disease, urine exhibits dysmorphic pink cells, of different shapes, whereas in bleeding from renal pelvis or the decrease urinary tract, the pink cells maintain normal morphology. Hypercalciuria ought to be excluded by willpower of urinary calcium to creatinine ratio on one or more random samples. A plain X-ray film of the abdomen and stomach ultrasound is finished to exclude main renal and urinary tract anomalies and calculi. In a major proportion, delicate microscopic hematuria spontaneously disappears over a period of a number of years. The preliminary step in analysis makes an attempt to distinguish glomerular from nonglomerular causes of hematuria (see Table 16. Estimation of complement C3 is a crucial screening test for postinfectious glomerulonephritis. A biopsy can additionally be thought-about in youngsters exhibiting persistent microscopic hematuria for 2 or more years even within the absence of the above options. This procedure is critical to diagnose IgA Disorders of Kidney and Urinary Tract - I proteinuria, particularly if associated with hematuria, ought to be promptly evaluated. Normally the protein to creatinine ratio, within the first morning urine specimen, is under 0. Fanconi syndrome) consists of low molecular weight proteins, whereas heavy proteinuria (predominantly albumin) indicates glomerular illness. Important causes of asymptomatic proteinuria include orthostatic proteinuria, chronic glomerular illnesses, reflux nephropathy, renal hypoplasia and barely renal tubular problems (Table 16. In orthostatic (postural) proteinuria, protein is absent in urine specimen collected after overnight recumbence. Alport Syndrome this situation is inherited in an X-linked method, although autosomal transmission is understood. Ultrastructural examination of renal biopsy shows variable thickness of glomerular basement membrane with lengths of marked attenuation to areas of lamination. Therapy is supportive, including the use of angiotensin changing enzyme inhibitors. Small quantities of protein are filtered but almost completely reabsorbed by the proximal tubule. Massive proteinuria happens in minimal change nephrotic syndrome, in which glomeruli are regular or show gentle adjustments. Low salt food regimen and extended remedy with angiotensin converting enzyme inhibitors or angiotensin receptor blockers are efficient in decreasing glomerular proteinuria. The medical severity varies, relying on histological involvement, salt and water retention and glomerular filtration rate. Key investigations embrace renal function checks, urinalysis, serum complement C3 and titers of antistreptolysin. Streptococcal infection of the throat or pores and skin precedes the onset of nephritis by 1 to four weeks. Immunofluorescence shows granular deposits of IgG and complement (C3) along capillary walls. Electron microscopy shows deposits (humps) on the subepithelial side of the glomerular basement membrane. Subclinical episodes are extra widespread than overt illness, particularly during epidemics. While the degree of oliguria normally correlates with the illness severity, anuria is uncommon. Streptococci, staphylococci, pneumococci, meningococci, Treponema pallidum, Salmonella, leptospira Plasmodium malariae, P. Serologic evidence for streptococcal an infection is current in most patients with pharyngitis, though antibiotic therapy could blunt this response. Moderately severe proliferation and exudative changes with infiltration of neutrophils. Management Patients with gentle oliguria and regular blood stress can be managed at house. The ideas of administration of sufferers with extreme oliguria and acute kidney injury are discussed later. The intake of sodium, potassium and fluids ought to be restricted till blood levels of urea reduce and urine output will increase. Overhydration is a dangerous compli cation as it might improve hypertension and precipitate left ventricular failure. Patients with azoternia require correct measurement of urine output and day by day weight, and restriction of fluid intake to an quantity equal to insensible losses and 24 hr urine output. Beta-blockers and angiotensin changing enzyme inhibitors carry threat of hyperkalemia. Treatment, as outlined above, should be continued and ranges of blood urea and electrolytes monitored. Dialysis is required in youngsters with extreme renal failure and prolonged oligoanuria, fluid overload and life threatening electrolyte disturbances. The signs begin to resolve in the first week with loss of edema and fall in blood pressure. Gross hematuria and significant proteinuria disappear inside 2-weeks, although microscopic hematuria and slight proteinuria could persist for a quantity of months. These instances need shut followup over a number of years with periodic urinalyses and measurements of blood pressure. The consequence is expounded to histological severity and immediate establishment of remedy. Without appropriate deal with ment, patients are at risk for progressive renal failure. Mild renal involvement indicated by microscopic hematuria and mild proteinuria is widespread. Note purpuric rash over the decrease limbs biopsy reveals mesangial proliferation with mesangial deposition of IgA. In between these episodes, microscopic hematuria and gentle protei nuria might persist.
Buy asendin 50 mg with amex
After bilateral adrenalectomy patients want lifelong remedy with hydrocortisone and mineralocorticoids depression definition and description order asendin 50 mg on-line. The contralateral gland is usually suppressed after unilateral adrenalectomy and these sufferers also want remedy with hydrocortisone for so much of months mood disorder secondary to general medical condition buy asendin 50 mg online. Biochemical prognosis is confirmed by an elevated plasma aldosterone concentration and suppressed plasma renin exercise. Adrenal venous sampling is typically necessary to differentiate unilateral from bilateral disease. The goal of the treatment is to normalize aldosterone ranges and prevent mortality and morbidity caused by hypertension, low potassium, cardiovascular and renal harm. Unilateral adenomas should be handled with adrenalectomy, which corrects hypokalaemia in 98% and improves hypertension in 90% of patients. Patients with bilateral hyperplasia must be treated with mineralocorticoid receptor antagonists. Its main benefit is good access and exposure of the adrenal gland, which allows elimination of huge and malignant tumours. Potential disadvantages are significant trauma from the incision, together with rib excision within the open posterolateral strategy, and the necessity to reposition the patient if you plan bilateral adrenalectomy. Place the affected person in the lateral decubitus place with the affected aspect uppermost. Prepare the pores and skin of the chest and stomach to enable for either extension of the incision or conversion to an open process. Insert two or three additional ports in the posterior, center and anterior axillary strains. Be conscious of the spleen, colon, pancreas and splenic vein so as to keep away from damaging them. Make positive that whole gland is mobilized � the lower limb incessantly descends as far as the renal hilum. Be cautious to not damage the renal vessels, which may contribute an adjunct renal artery to the superior pole. Mobilize the remaining gland from the kidney, liver and posterior muscle tissue by dividing small arteries with a harmonic scalpel. Incise the deep fascia, allowSweep the pleura superiorly and posteriorly and equally sweep the peritoneum anteriorly, using gauze swabs. Divide latissimus dorsi and serratus posterior muscle tissue with chopping diathermy and incise the periosteum of the eleventh rib using a diathermy point. Strip the periosteum from the rib throughout its length, liberating the deep attachments to the rib with a gauze swab. Have your assistant retract the kidney inferiorly while you proceed carefully to bluntly dissect the fats above and medial to the kidney. Handle the gland gently to keep away from disruption and avoid damaging surrounding organs. As a rule, order a chest X-ray in the recovery ward to exclude a big pneumothorax. Endoscopic posterior (retroperitoneal) method 1 n the approach for left and right adrenalectomy is comparable. Take care to close the pleura if it was three n Introduce two additional ports (5 mm) close to the costal margins on either side of the port used for the zero or 30 digicam. Identify the kidney, retract it downwards and dissect perirenal fat until you see the sting of the adrenal. Division of the adrenal vein between clips or utilizing a vascular stapler greatly increases mobility of the gland. Its main disadvantage is restricted working house, which only allows resection of adrenals smaller than 6 cm. Excise the rib, carefully avoiding damage to the neurovascular bundle at the inferior margin of the rib. This strategy provides entry to each adrenals, permits extension of the incision in to the chest and safe management of main blood vessels if essential, resection of concerned organs and prolonged lymphadenectomy. The commonest causes for conversion are extreme bleeding, problem in mobilizing the mass as a result of its giant dimension, damage to surrounding organs or, especially early on the learning course, the length of operation. Complications after adrenalectomy (10�15%) may be the results of both suboptimal perioperative management of metabolic and cardiovascular abnormalities brought on by functioning adrenal lots or associated to the surgical process itself. This provides good entry to the adrenal and renal hilum and permits safe dissection of huge tumours. Open anterior approach 1 n Electrolyte 2 n Failure to cease medicines not required after surgical procedure. For massive and infiltrating tumours encircle the inferior vena cava with tapes placed below and above the liver to provide protected control in case of main haemorrhage or if its resection and graft replacement are indicated. Carefully dissect and retract and sensibly employ the harmonic scalpel, diathermy, clips or vascular stapler to stop this complication. Repair injuries detected throughout operation immediately � however the presentation of thermal damage to the bowel may be delayed by 24�48 hours. Remember to examine submit operatively potassium and cortisol levels as some patients can suppress cortisol manufacturing in contralateral gland. The three main websites for aneurysms are the abdominal aorta, femoral and popliteal arteries. Aneurysmal illness secondary to atherosclerosis is liable for appreciable morbidity and mortality in the developed world and the prevalence of abdominal aortic aneurysm is increasing. Infected (mycotic) aneurysms are a lot much less common than those attributable to degenerative disease. True mycotic aneurysms result from septic emboli of cardiac origin (endocarditis), which may result in multiple aneurysms at totally different websites. With an ageing inhabitants, microbial aneurysmal arteritis is seen more incessantly than true mycotic aneurysms; this outcomes from bacterial seeding in to diseased arterial intima with subsequent pseudoaneurysm formation, the commonest infecting organisms being the Salmonella species, Escherichia coli, Staphylococcus species and Klebsiella pneumoniae. However, all competent surgeons ought to be acquainted with the basic rules of arterial management, restore and reconstruction. Sudden occlusion of an otherwise normal main artery may threaten both the limb and the lifetime of the patient and warrants emergency intervention either by embolectomy or dissolution of the occlusion. The sections which comply with assume that the patient has already been critically evaluated and the necessity for operation established. This might end result from sharp or blunt trauma secondary to assault or road visitors accident. Iatrogenic injuries are becoming more prevalent as a consequence of percutaneous arterial entry for diagnostic procedures and treatments similar to coronary interventions. Challenging self-induced injuries are also seen as a result of intravenous drug addiction. The finest outcomes are achieved with a multidisciplinary approach by a team of specialised vascular anaesthetists, vascular surgeons, interventional radiologists and vascular scientists to optimize the care of vascular patients. In addition, services similar to cell-saver know-how to cut back blood transfusion, point-of-care coagulation testing, intra-operative 2 n Aneurysm.
Discount 50 mg asendin with amex
The treating doctor should advise patients and fogeys regarding prevention of endocarditis anxiety 68 theorist seesaa asendin 50mg lowest price. Culture negative 6 the selection of antibiotics should ideally be guided by culture results and organism sensitivity Disorders of Cardiovascular System - encouraged depression leads to generic 50mg asendin mastercard. Careful attention to prophylaxis on the longterm is useful in stopping relapses. Guidelines from American Heart Association: A guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Car diovascular Surgery and Anesthesia. The presentation could also be abrupt, with cardiovascular collapse, or insidious improvement of coronary heart failure. Examination exhibits cardiac enlargement, tachycardia, muffled coronary heart sounds and options of congestive cardiac failure. Digoxin ought to be used cautiously, preferably in half to three quarters of the usual dose. It is taken into account main cardio myopathy when the etiology is unknown, and secondary, if the myocardial illness is attributed to a systemic disease. Myocardial ailments are categorized clinically as (i) dilated, (ii) restrictive, and (iii) hypertrophic type of cardio myopathy. A important proportion of sufferers have correctible causes of left ventricular dysfunction that mimics dilated cardiomyopathy (Table 15. A prognosis of idiopathic dilated cardiomyopathy can solely be made after these causes are excluded. Echo cardiogram confirms dilated ventricular cavity with out hypertrophy of the free wall of the left ventricle or the septum. Beta-blockers management the center price, scale back vasoconstriction caused by catecholamines and upgrade beta-receptors. These agents are anticipated to stop or retard myocardial injury associated to excessive catecholamine levels. Though experience in kids is limited, it should be thought-about in presence of disproportionate tachycardia. Despite aggressive remedy, a couple of third of youngsters with cardiomyopathy continue to deteriorate with time and eventually become refractory. Intermittent (weekly or bi weekly) dopamine or dobutarnine infusions could additionally be used successfully in some sufferers. It is essential to think about numerous correctable circumstances that can masquerade as cardiomyopathy (Table 15. Echocardiography exhibits a large proper coronary artery and absence of the origin of left coronary artery from the aorta. The left coronary artery is seen to arise from the pul monary artery and exhibits move within the reverse path in the left anterior descending artery and the left circumflex artery. This circulate reversal results from collateral circulate in to the left coronary system from the proper coronary artery. The remedy is surgical and requires mobilization and translocating the origin from pulmonary artery to aorta. Restriction to ventri cular filling is normally related to either endomyo cardial fibrosis or endocardial fibroelastosis with a standard or smaller than normal left ventricle. Endomyocardial fibrosis was beforehand endemic in the state of Kerala and is now quite uncommon wherever within the country. Papillary muscles and chordae could additionally be tethered by the connective tissue, resulting in extreme mitral or tricuspid regurgitation. The echocardiographic diagnosis of anomalous left coronary artery from pulmonary artery was confirmed at surgery. The Patients with predominant left sided involvement have symptoms of dyspnea, orthopnea, hemoptysis and embolic phenomena. Cardiac output is low and there are features of pulmonary venous and arterial hypertension. With predominant right-sided involvement, sufferers present with fatigue, pedal edema and ascites. There is cardiomegaly with outstanding cardiac pulsations in the second, third and fourth left interspace from a dilated right ventricular outflow. Decortication or stripping of the endocardium with mitral valve replacement has been tried with variable success. Restrictive cardiomyopathy of different unusual varieties is characterised by a mixture of options of left and right-sided failure with a traditional sized coronary heart. Clinically, or even following cardiac catheterization, it might be difficult to distinguish it from constrictive pericarditis. However, youngsters with restrictive cardiomyopathy tend to have dominant left sided involvement and dispropor tionate pulmonary hypertension. Hypertrophic Cardiomyopathy Hypertrophic cardiomyopathy might occur (a) without outflow obstruction, or (b) with outflow obstruction. The free walls of the left and right ventricles are hypertrophied to a lesser extent. The ventricular septum bulges in to the left ventricle, and the malaligned anterior mitral valve leaflet causes obstruction within the left ventricular outflow throughout systole. The second sound may be normally cut up, single or paradoxically cut up, depending on the severity of the left ventricular outflow obstruction. The ejection systolic murmur increases in depth with maneuvers which improve the myocardial contractility or decrease the volume of the left ventricle. The murmur decrea ses in depth with procedures that improve left ventricular volume or decrease the myocardial contractility. Thus, sudden squatting tends to lower the intensity of the murmur whereas standing upright from sitting position by lowering the venous return tends to decrease the left ventricular dimension and increases the depth of the ejection systolic murmur. The electrocardiogram exhibits left ventricular hypertrophy, with or with out ischemic adjustments. Hypertrophic cardiomyopathy typically has an autosomal dominant sample of inheritance with a variable but excessive diploma of penetrance. Mutations in beta-myosin, troponin T and alpha-tropomyosin gene are believed to be res ponsible. Magnetic resonance imaging could assist determine myocardial fibrosis and not directly help in identifying patients vulnerable to sudden cardiac dying. Patients with hypertrophic obstructive cardiomyopathy ought to have a 24 hr Holter to document the presence of arrhythmias. Digitalis and different inotropic medicine as nicely as diuretics and nitrates are contraindicated in these patients. Beta-blockers decrease the myocardial contractility and thus lower the obstruction. Occasionally, the ache could also be felt over the neck and shoulder and will worsen on lying down. It could be heard anywhere over the precordium, is unrela ted to the respiratory cycle and increases on pressing the Table 15. The coronary heart sounds become muffled and evidence of peripheral congestion in the form of raised jugular venous stress, hepatomegaly and edema may develop.