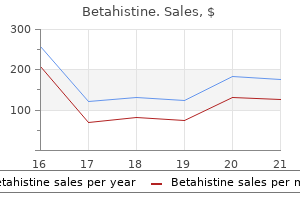
Betahistine
Betahistine dosages: 16 mg
Betahistine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

Buy betahistine 16 mg amex
Incision is revamped medial hindfoot medications held before dialysis buy betahistine 16mg without prescription, off weight-bearing floor medications adhd order betahistine 16 mg visa, ensuring not to disturb nerves. Cut the extensor hallucis and make an arthrotomy within the joint, releasing up the collateral ligaments. Use curettes to take away the articular cartilage and use a 2-mm drill bit to fenestrate both sides of the joint. Place a Kirschner wire from proximal to distal via the distal phalanx and out the tip of the toe slightly below the nail, leaving minimal wire inside the joint. Pass the tendon from lateral to medial via the hole and suture it again on to itself using nonabsorbable suture while holding the ankle in a neutral to slightly dorsiflexed position. Incision is made transversely over the interphalangeal joint to take away cartilage and harvest extensor hallucis longus tendon. Incision is made longitudinally over the first metatarsal, transferring the tendon to the neck, and a screw is positioned across the interphalangeal joint in lag mode. The drill should be angled barely medial to guarantee coming into the remaining calcaneus. The tendency is to take too little of a dorsal wedge, leaving the primary metatarsal plantarflexed and making the affected person prone to recurrence. The medial calcaneal department of the tibial nerve and the intrinsic musculature of the foot are at risk, so careful dissection is warranted. Patients are saved immobilized and non�weight-bearing for a total of eight weeks, and weight bearing is begun when bony therapeutic has occurred. Tarsometatarsal truncated-wedge arthrodesis for pes cavus and equinovarus deformity of the fore part of the foot. Early therapy while feet are flexible is suggested to forestall extra in depth procedures required for rigid deformities and problems from progressive arthrosis. In many cases a mixture of the first two varieties occurs, referred to as the pes equinocavovarus. The equinocavovarus foot describes a principally acquired foot deformity consisting of an increased arch of the foot (forefoot and midfoot equinus), a restricted dorsiflexion of the ankle joint (hind foot equinus), and a hindfoot varus. A concomitant forefoot and midfoot adductus, supinatus, or pronatus can happen, relying on the underlying pathology. In the lower extremity deformity was extra superior and unequally developed on both side. The toes and ankle joint could be freely moved in all instructions except that of eversion, owing to full paralysis of the peronei muscles. The different muscular tissues of the lower extremity had been able to inflicting powerful actions. This ends in an overbalance of the extrinsic extensor muscles in comparison to the intrinsic extensor muscles. At the identical time the lengthy toe flexors pull the top phalangeal bone into plantarflexion. Relative overactivity of the posterior tibial muscle forces the hindfoot into varus position. The pressure of the lengthy toe flexors (increased flexion of the metatarsophalangeal joints) is antagonized by increased exercise of the long peroneal muscle (peroneus longus) that also pulls the first metatarsal bone into plantarflexion. An acquired horizontal place of the talus ensuing from hindfoot supination could cause a limited dorsiflexion. The restricted ankle dorsiflexion in pes equinocavovarus might cause a genu recurvatum. Another consequence is toe strolling with excessive load transfer to the metatarsophalangeal joints and a lowered stance part of gait. Pronation in the subtalar joint is inhibited, probably inflicting impingement between the medial malleolus and the talus, much like the impingement in extreme clubfoot deformity. Another consequence is the medialization of the navicular, which migrates towards the medial malleolus to cause further bony impingement. The examiner inspects the medial side of the foot, evaluating for elevated heel, elevated medial arch, plantarflexion of the first metatarsal bone, and claw toe deformity of the primary column of the foot. The examiner inspects the lateral aspect of the foot, evaluating for posterior shift of the lateral malleolus, convexity of the lateral border of the foot, prominent foundation of the fifth metatarsal bone, and outstanding head of the talus on the lateral dorsum of the foot. The examiner inspects the plantar facet of the foot, evaluating for convex lateral border of the foot and distinguished basis of the fifth metatarsal bone, increased weight bearing of the heads of the primary and fifth metatarsal bones, increased pores and skin wheal (in severe cases, the heads of all metatarsal bones are involved), and hindfoot equinus (lack of weight bearing on the heel). The examiner inspects the ventral facet of the foot, evaluating for lateral prominence of the talar head, convex lateral border of the foot, forefoot adduction, and clawing of the primary through fifth toes. This check is essential for detecting equinus deformity and differentiating between the involvement of gastrocnemius and soleus muscle tissue. There is a medial shift of the talonavicular joint and in some circumstances the calcaneocuboid joint. It is used to identify the imbalance of the major stress factors of the foot as a result of the deformity. I,J 3D Foot and Gait Analysis (Heidelberg Foot Model) this objective and computer-assisted methodology records movements between single segments of the foot in all three planes (sagittal, frontal, transverse) throughout walking. After processing by devoted software program, attribute segment actions in all three planes could be visualized. Left: elevated medial arch; center: elevated subtalar inversion; proper: increased forefoot adduction. Possible nonoperative therapy methods are: Orthopaedic arch assist (reduced head of the primary metatarsal bone and smooth bedding) Orthopaedic footwear Positioning the patient is positioned supine on the operating table. After the Steindler process, the tendon transfers are ready (split posterior tibialis transfer,19 modified Jones procedure4). Depending on the severity of deformity, an arthrodesis of the Chopart joint or triple arthrodesis could additionally be required. In instances of dorsal impingement of the talus on the tibia with restricted dorsiflexion or extreme hindfoot equinus, we suggest adding a modified Lambrinudi process. To appropriate hindfoot equinus, an intramuscular lengthening of the calf muscular tissues or an open or percutaneous Achilles tendon lengthening is carried out. In instances of extreme equinus tested in knee flexion and extension proximal or distal Achilles tendon lengthening (open or percutaneous) is taken into account. In mildly concerned cases intramuscular calf muscle lengthening is done (eg, Baumann procedure23). In our arms, this method represents step one in the remedy of pes equinocavovarus. It is a straightforward method for correcting flexible forefoot and midfoot cavus deformity. Carefully divide the subcutaneous tissue and retract it with Langenbeck retractors. Sharply transect the aponeurosis as well as the origin of the short flexor digitorum muscle with the sturdy preparation scissors. Furthermore, it eliminates the perform of the posterior tibial muscle on the hindfoot place. Tension the tendon using an Overholt clamp and launch it at its insertion point with the scalpel as distally as potential. Make one other pores and skin incision (3 cm) at the distal medial calf, three to 4 fingerbreadths proximally to the ankle, instantly behind the posterior edge of the tibia.
Discount 16 mg betahistine amex
Midline posterior subperiosteal publicity of C1 and C2 laminae is carried out with cautious attention to dissect from midline laterally at C1 to prevent damage to the vertebral artery medicine xl3 order 16mg betahistine with amex. The ligamentum flavum between C1 and the occiput and in addition between C1 and C2 is sharply divided new medicine 16 mg betahistine discount amex. Although Brooks originally described use of two doubled 20-gauge chrome steel wires handed beneath all sides of the arch of C1 followed by C2 with the help of a no. After the cables are handed with a loop at the finish, two full-thickness rectangular bone grafts measuring approximately 1. The sides of every graft are beveled to match within the interval between the C1 and C2 laminae and placed on each side. We use a suture for this system when the Gallie graft is employed in conjunction with Magerl transarticular fixation, as a end result of the Gallie configuration is relied on for maintenance of graft position, not for mechanical stability. The small grooves are placed on the superior and inferior edges of the graft to hold the sutures in place. This is common into an H shape, and the cancellous side is placed dealing with down on the decorticated posterior parts of C1�2. Careful preoperative planning will guide choice of the appropriate process to scale back the danger of damage. In the event of damage to a vertebral artery during a Magerl procedure, a short screw could also be positioned to comprise the bleeding. An various fixation method should be employed, such as a Brooks or Gallie procedure. Gentle tamponade of the venous sinuses, along with utility of hemostatic brokers, is recommended. Once the surgical instruments are removed along with the strain from the retractors, the bleeding is often is controlled with ease. Supplemental wiring with the Magerl, Goel, and C2 laminar screw methods provides no vital mechanical advantage. However, a suture configuration of an identical nature will hold the graft surfaces in correct apposition to the decorticated host bone, possibly enhancing the fusion rates. It could additionally be indicated for revision procedures, patients with incompetent posterior C�1 arches, or certain fracture patterns, or for high-risk hosts. The type of collar used and duration of wear should be in accordance with surgeon judgment about host bone, security of fixation, anticipated affected person compliance, etc. Rheumatoid arthritis of the cervical backbone: a long-term evaluation with predictors of paralysis and restoration. Anatomic relationship of the inner carotid artery to the c1 vertebra: a case report of the cervical reconstruction for chordoma and pilot study to assess the risk of screw fixation of the atlas. Constructs incorporating intralaminar C2 screws provide inflexible stability for atlantoaxial fixation. Primary posterior fusion of C1-2 in odontoid fractures: indications, techniques, and outcomes of transarticular screw fixation. Morphologic concerns of C2 isthmus dimensions for the placement of transarticular screws. McGuire and Harkey13 confirmed strong fusion in eight sufferers utilizing a transfect screw approach. Fielding and associates5 achieved fusion in forty five of 46 sufferers with fractures using the Gallie approach. Brooks and Jenkins2 used a C1�2 sublaminar wiring method to obtain fusion in 14 out of 15 patients. Harms 9 reported fusion in all 37 sufferers with C1 lateral mass and C2 pedicle minipolyaxial screw and rod construct. Cost-effectiveness: the Goel C1�2 articular mass technique has been popularized by Harms, and is offered as much less dangerous than the Magerl method with respect to the vertebral artery. The annulus fibrosus converts these masses to hoop stresses, thereby containing the nuclear materials. The endplates allow diffusion of nutrition into, and waste products out of, the nucleus. Together, they allow for the three fundamental spinal segmental functions: mobility, stability, and safety of the close by neurologic buildings. With early or intermediate disc degeneration (natural getting older with or without minor repetitive trauma), the endplates fail to enable adequate diffusion, the nucleus fails to substitute degraded proteoglycans, and annular support weakens (failure of crosslinking, growth of clefts). A mixture of herniation, nerve root compression, and an inflammatory interface is required for nerve root dysfunction and related radiculopathy and sciatica. The nerve roots travel within the frequent dural sac (the cauda equina) after which exit at each level. The first floor is the disc stage, the second floor is the foraminal level, and the third flooring is the pedicle stage. Plain radiographs could present disc area narrowing, early formation of osteophytes, or a "sciatic scoliosis. They also permit glorious delineation of bony anomalies which will show very important to preoperative planning and intraoperative localization, corresponding to transitional lumbosacral articulations or spina bifida occulta. Progressive (ie, worsening) neurologic deficit: the earlier the higher prognostically Relative indications Failure of conservative measures larger than 6 weeks to 3 months Multiply recurrent sciatica Significant neurologic deficit In every case, the properly knowledgeable patient should clearly perceive the current finest proof: long-term (5-year) outcomes are related between surgery and nonoperative remedy, however surgery can afford more rapid resolution of signs. The space of root compression can be described relative to the nerve root anatomy (eg, at the shoulder of the traversing root, in the axilla of the exiting root). Approach the interlaminar window method is used in about 90% of lumbar disc herniations requiring surgical procedure. It is acceptable for herniations throughout the central canal or subarticular zones from L1 to S1 and for herniations within the foramen at L5�S1. The intertransverse window approach is used in about 10% of lumbar disc herniations requiring surgery. It is acceptable for herniations inside the foraminal and extraforaminal zones from L1 to L5. For each step in the procedure, incision, excision, and retraction of tissues ought to be minimized. The objective is to get the job done fully and safely with minimal trauma to tissues indirectly concerned in the pathologic process. Some hip and knee flexion will decrease lumbar lordosis and facilitate an strategy through the interlaminar window. The stomach have to be free to lower intra-abdominal stress and venous backflow by way of the plexus of Batson into the spinal canal. The subcutaneous tissues are then gently and bluntly mobilized and retracted to enable visualization of the dorsolumbar fascia. From right here, certainly one of two home windows of approach shall be undertaken based mostly on the situation of the disc herniation: the interlaminar window or the intertransverse window. A Cobb elevator is used to gently elevate the muscle (multifidus) from the spinous processes to the midportion of the facet joint laterally.
Diseases
- Fumaric aciduria
- Swyer James and McLeod Syndrome
- Short stature microcephaly seizures deafness
- Dilated cardiomyopathy
- Landouzy Dejerine muscular dystrophy
- Cogan syndrome
- Polymorphous low-grade adenocarcinoma
- Amnesia, childhood
- Syringocystadenoma papilliferum
Discount betahistine 16mg with mastercard
The smaller saws make it simpler to resect prominences with precision medicine show betahistine 16 mg line, and easily morselize massive bone fragments to be evacuated from the joint medications rights betahistine 16 mg buy overnight delivery. A rasp for last preparation of cut bony surfaces A 90-degree angled curette, particularly to separate bone from the posterior capsule A toothed lamina spreader to distract the joint and aid in realignment of preoperative ankle deformity. A lamina spreader positioned on the concave side of the joint also assists in realignment. A toothless lamina spreader to judiciously distract the ankle to improve exposure even after getting ready the surfaces of the tibia and talus Large fluoroscopic scanner Fluoroscopy confirms proper alignment of the slicing guide to the ankle. The leg holder maintains the leg in position relative to the alignment guides and reference drill. With the leg holder, the big scanner is important to straddle the leg and leg holder. Fluoroscopy through the working desk is important, so a little fluoroscopy unit is inadequate. Subtle changes to the alignment guides relative to the ankle enable fine-tuning for the reference drill trajectory. Positioning Supine Plantar aspect of operated foot at end of operating desk Foot and ankle well balanced with toes directed to the ceiling A bolster underneath the ipsilateral hip prevents undesired exterior rotation of the hip. However, using a thigh tourniquet with a popliteal block typically requires a supplemental femoral nerve block (patient quickly forfeits knee extension within the instant postoperative period) or basic anesthesia. Noninvasive vascular research and potential vascular surgical procedure consultation if necessary the surgeon should inspect the ankle for prior scars or surgical approaches that must be thought-about in planning the surgical method for total ankle arthroplasty. The surgeon should understand the medical and radiographic alignment of the lower extremity, ankle, and foot. At no point ought to direct tension be positioned on the pores and skin margins; we perform deep, full-thickness retraction as soon as possible to limit the danger of skin complications. Identify the deep neurovascular bundle (anterior tibial� dorsalis pedis artery and deep peroneal nerve) and thoroughly retract it laterally all through the remainder of the procedure. Perform an anterior capsulotomy and elevate the tibial and dorsal talar periosteum to about 6 to eight cm proxi- mal to the tibial plafond and talonavicular joint, respectively. Remove anterior tibial and talar osteophytes to facilitate publicity and avoid interference with the instrumentation. Varus malalignment We routinely perform a complete medial release for moderate to extreme varus malalignment. The idea is just like balancing the varus knee for whole knee arthroplasty and was well described by Bonnin et al. We routinely subperiosteally raise a continuous delicate tissue sleeve from the distal medial tibia to the medial talus. The superficial deltoid (medial collateral) ligament is elevated however left intact proximally and attached distally. The launch of these fibers is full when the posterior tibial tendon can be visualized. The deep deltoid (medial collateral) ligament may be peeled off the medial malleolus to stability the ankle appropriately. In our experience, with an appropriate medial release, optimum bony resection and metallic part alignment, and proper sizing of the polyethylene, a lateral ligament reconstruction is seldom essential. This marks a major change from our initial practices in rebalancing the varus ankle. Often, valgus malalignment is secondary to lateral ankle joint collapse and a few medial (deltoid) ligament attenuation. While the latter portion of this statement appears counterintuitive, it has been our expertise in treating many sufferers with end-stage ankle arthritis and valgus malalignment. Moreover, lateral launch in such situations could result in paradoxical lateral instability! In this varus ankle a whole medial peel of the deltoid ligament has been carried out and the ankle may be opened up with the lamina spreader. There was a big ossicle at the tip of the fibula representing an old avulsion fracture containing the anterior talofibular ligament. Hence, the bone was eliminated (C) and a Brostrom ligament reconstruction was performed (D). In this view the lamina spreader has been placed laterally on the concave side, and now the talus is orthogonal to the tibia and the alignment guide. If the foot and ankle are secured first, it might be tough to position the lamina spreader successfully. Proper rotation We use a small straight osteotome within the medial gutter as a reference. The foot is rotated till the osteotome is parallel with the leg holder foot plate. Coronal airplane alignment In the mediolateral plane, heart the heel over the place to begin for the reference drill. This place also needs to be in line with the tibial shaft axis in order that minimal changes shall be essential. Sagittal airplane alignment We use the lateral alignment guides to grossly set this alignment. In our experience, correct heel position, optimum tibial alignment, and best rotation could make the foot seem internally rotated relative to the lower leg. Fluoroscopic view being obtained of leg holder with cannula and drill in place to ensure appropriate assembly of leg holder. Gelpi retractor holding deep tissue apart with lamina spreader on concave medial aspect of varus ankle. Overhead view of lamina spreader in place and deep Gelpi retractor holding deep tissue apart. Foot pedals are used to management tilting of the desk to get the alignment sites exactly parallel to one another. Subtle changes to the alignment guides relative to the ankle to enable fine-tuning for the reference drill trajectory may be made with the foot pedal. Reference drill Make a horizontally oriented 1-cm incision within the plantar foot, immediately within the opening within the foot frame for passing the reference drill. Avoid holding the frame while inserting this information as this could permit the drill to bend, achieving a different trajectory than the information. Since the trajectory may change when the drill hits the plantar medial calcaneus, we typically begin the drill in reverse and "peck drill" (tap drill) to gradually penetrate the plantar calcaneal cortex with out veering from the planned trajectory. Since drilling may shift the frame barely, fluoroscopic confirmation of correct alignment must be re-established, after which proper alignment of the reference drill may be confirmed. Confirm applicable reference drill position fluoroscopically in both the coronal and sagittal planes. Position the slicing block in roughly the correct position through the use of the reference drill information to estimate its position. The place of the slicing block ought to be finalized provided that proper alignment has been confirmed fluoroscopically with the alignment guides.
16 mg betahistine buy overnight delivery
Perform this cautiously schedule 6 medications discount betahistine 16 mg line, although treatment gout 16 mg betahistine purchase with mastercard, as a variety of the talar dome blood provide travels although the deltoid department off the posterior tibial artery. Tibiotalar joint reduction, with neutral dorsiflexion�plantarflexion, slight hindfoot valgus, and second metatarsal rotated to anterior tibial crest. If the talus fails to translate posteriorly within the ankle mortise, then the posterior malleolus could need to be weakened to allow the talus to cut back beneath the tibial axis. In my expertise, including a supplemental anterior plate to an ankle arthrodesis construct provides appreciable stability. He lacks some plantarflexion; time will inform what effect it will have on the hindfoot articulations which are making an attempt to compensate. The talus is once more in a physiologic relationship with the tibia, bettering his biomechanics despite ankle arthrodesis. Medial screw positioned first from the medial tibia to the talar dome, positioned by way of a medial stab incision. Traditional posterior-to-anterior screw, placed by way of a posterolateral stab incision (care have to be maintained to avoid damage to the sural nerve). Postoperative weight-bearing radiographs of example affected person with traditional screw fixation and supplemental anterior plate. Preoperative radiographs of patient present process double anterior plating arthrodesis method. Lateral anterior plate utilized and secured to talus and proximal compression gadget in place. Intraoperative fluoroscopic views of ankle of a different patient present process dual anterior plating, with provisional fixation and lateral plate in place. While the locking plate creates axial compression, a gentle but desirable valgus second may be launched because the lateral plate is getting used for compression. To get hold of optimum compression, provisional fixation is removed earlier than compression is utilized but after the screws are locked into the talar neck and the compression gadget is secured proximally. Since compression has already been carried out, this medial plate, which is also precontoured, serves to statically lock the arthrodesis. Standard wound closure I routinely close the capsule, extensor retinaculum, subcutaneous layer, and skin (to a tensionless closure). The deep neurovascular bundle, extensor tendons, and superficial peroneal nerve have to be protected during closure. Intraoperative fluoroscopic views of two screws placed via the plate into the posterior talus for added stability. Intraoperative fluoroscopic views of different patient with supplemental screw to anterior plating. Lateral view (note damaged guide pin; it is essential to follow the precise trajectory of the guide pin with cannulated screw systems). In some circumstances, I actually have performed a staged arthrodesis, with initial d�bridement and antibiotic bead place- ment. The external fixator may be positioned at that preliminary procedure or on the definitive procedure when the antibiotic beads are eliminated and the joint is reduced and compressed with the exterior fixator. Preoperative radiographs of example patient for ankle arthrodesis with exterior fixation; patient has failed ankle arthrodesis with internal fixation. The external rotation malunion of the distal tibia creates extreme external rotation of the foot relative to the tibial axis. Forty-five-year-old patient with posttraumatic arthritis and deformity of the ankle, failing to respond to a prior try at ankle arthrodesis. A standard anterior approach is simply too dangerous and, in my view, would depart an insufficient pores and skin bridge to the prior incision. I additionally switched the lamina spreader to the medial wound in order that I could put together the rest of the joint by way of the lateral incision. However, that is more essential with inner fixation; with exterior fixation such malrotation might still be corrected postoperatively with external fixator frame adjustment. Medial incision is getting used for joint preparation whereas joint is being distracted by lamina spreader positioned by way of lateral incision. Ankle could be manually reduced to a physiologic position with the second metatarsal aligned to the anterior tibial shaft axis. Joint reduction Neutral dorsiflexion�plantarflexion Slight hindfoot valgus Correct malrotation Align second metatarsal with the anterior tibial crest. I routinely shut the injuries at this level because once the exterior fixator is in place, suturing is especially tedious. However, if you favor to delay the wound closure till the external fixator is in place, one or two struts can simply be reflected to permit enough entry to the wound or wounds. Foot plate I suspend the foot plate ("horseshoe") from a transverse forefoot wire. Before tensioning the thin wires, I shut the horseshoe-shaped foot plate anteriorly. Having two foot plate elements affords less interference between the struts (that will connect the proximal ring block to the foot plate) and the skinny wires to be passed through the foot from the foot plate. These two wires both need to be built up from a single foot plate or linked to the proximal part of a two-ring foot plate set-up. Foot plate suspended from forefoot wire and calcaneal wires being passed to stabilize the hindfoot. The ring has been closed on the foot frame so that rigidity in all wires can be successfully maintained. Closing the highest ring allows the foot frame to be closed even without putting a half-ring on the anterior portion of the "horseshoe. Without talar wires compression would be positioned not solely on the tibiotalar joint but additionally on the subtalar joint. A perhaps more subtle (but not more complicated) development of the foot plate is to distract between the two components of the foot plate, so that the subtalar joint is distracted while the tibiotalar joint is compressed. Adding struts to be used for compression between the proximal ring block and the foot frame. Ankle with neutral dorsiflexion�plantarflexion and plantar foot is distal to most distal ring�plate. If adjustments need to be made, the pc program could also be used to run an effective correction right now. However, on the operating table, the struts could merely be loosened, a gross guide adjustment could be made (with the provisional fixation removed), and the struts once more secured. Final verify to make certain that all bolts and connections are steady Sterile dressings on the wound Sterile dressings on the wires and half-pins Pin irritation usually occurs because of pores and skin motion or tension about the half-pins or skinny wires. I routinely place thick dressings around the skinny wires and half-pins, creating average stress from the dressing on the skin instantly adjoining to the halfpin or wire and thereby stabilizing the pores and skin. Optimal place is impartial dorsiflexion�plantarflexion, slight hindfoot valgus, and the second metatarsal aligned with the anterior tibial crest. Internal fixation for ankle arthrodesis might be contraindicated; nonetheless, arthrodesis is still potential with exterior fixation. Internal and external fixation could stabilize the joint, but satisfactory joint preparation for arthrodesis is important for fusion to happen.
Betahistine 16mg buy on-line
Working reminiscence depends on declarative reminiscence representations to provide semantic that means and context medicine 72 hours betahistine 16mg proven. During working memory tasks medicine checker generic 16mg betahistine, cortical perceptual areas associated with representations of declarative reminiscence turn out to be activated and show increased synchrony with prefrontal regions. Long-Term Potentiation, Synaptic Tagging, and the Consolidation Model of Memory the consolidation speculation of memory was first proposed by M�ller and Pilzecker in 1900. This effect, called retroactive interference, is temporally graded such that the susceptibility of the reminiscence is greatest instantly after studying and decreases with time. M�ller and Pilzecker proposed that the reminiscence hint should initially exist in a fragile state, however subsequently becomes secure through the method of consolidation. Within the framework of the synaptic plasticity and memory hypothesis, which states that activity-induced synaptic plasticity is each necessary and adequate for the information storage underlying memory,155 encoding therefore implies that some type of synaptic plasticity has been initiated. An quick practical expression of change in synaptic energy seen in mobile fashions can occur within the absence of any structural change in dendritic spines. The perpetuation of these preliminary changes in synaptic strength via structural and functional reworking represents the neural correlate of memory consolidation. The preliminary description reported that high-frequency stimulation of the perforant path (connecting entorhinal cortex to hippocampus) caused a sustained enhance in synaptic transmission in the dentate gyrus. Nonetheless, certain principles are important and related to anesthesia research and can be acknowledged succinctly. This nondeterminism is in preserving with true memory habits, which in a number of contexts is influenced by occasions preceding and following encoding. In 2000, Nader and colleagues169 reported that an old reminiscence for auditory fear conditioning, which might usually not be delicate to protein inhibitors, may be made newly delicate whether it is retrieved. The implication was that retrieval of a memory renders it transiently plastic, after which it restabilizes. This course of is termed reconsolidation and has been subsequently demonstrated in multiple settings and species, together with in human behavioral paradigms. Certainly, most pharmacologic agents-including anesthetic drugs-that inhibit consolidation would be rational candidates for comparable effects on reconsolidation. A cooperative relationship between and synchrony exists such that the part of oscillations are coupled to the amplitude (phase-amplitude coupling) or section (phase-phase coupling) of the slower oscillation. However, the putative candidates can be dramatically narrowed by appreciating that memoryrelated processes are constrained to operating within a specific time area and in a specific neuroanatomic location. A important emphasis of current research in people is therefore the drive to outline the temporal and neuroanatomic characteristics of anesthetic amnesia exactly, as a end result of these traits richly inform and dismiss hypotheses concerning underlying mechanisms. Studies within the early Nineteen Seventies discovered no retrograde amnesia with the administration of thiopental (6 mg/kg) and methohexital (4 mg/ kg). Similarly, memory is normal for word lists learned in the preoperative holding area or working room instantly before induction,a hundred ninety and for pictures considered instantly earlier than propofol induction. A recent study197 described an experiment in which volunteer subjects learned a word list and were then immediately administered a steady-state infusion of both propofol (0. Memory for the phrases was tested at a quantity of intervals throughout a time domain spanning from 20 minutes to 24 hours after encoding. In distinction to finding retrograde amnesia, propofol subjects paradoxically retained extra materials than did placebo subjects. Phase synchronization of these oscillations, which coordinates the excitability of associated neurons, is a basic neural mechanism. It helps neural communication by creating transient and dynamic associations between completely different practical brain areas. For example, a major body of evidence supports the hypothesis that -phase (40 Hz) synchronization binds the regions serving the assorted attributes of a conscious perception. Here, vital interest has centered on -phase (4 to eight Hz) synchronization, which in distinction to undergoes section reset in response to a stimulus. The discovering of retrograde facilitation and failure to identify retrograde amnesia strongly recommend that the mechanism of anesthetic amnesia is restricted to induction processes within the consolidation cascade. To illustrate: if a drug had a direct impact on a course of occurring tc minutes after encoding, the impact can be to block consolidation for an event that occurred tc minutes in the past, creating a transparent retrograde amnesia window. The strongest counterargument to the induction hypothesis has instructed a direct function for downstream protein transcription processes,205 but the temporal window in which this might occur remains undefined. A simplified version of the Wickelgren Power Law was applied in a big human volunteer examine to characterize the amnestic effects of a number of intravenous anesthetic medicine. A given memory state mt is thus a function of two variables that can theoretically be modulated independently. The energy of the mathematical modeling method is that it enables characterization in phrases of each encoding failure (decreased) and consolidation failure (increased). The two-parameter power decay operate accurately describes the temporal course of amnesia for subjects receiving propofol (0. In contrast, dexmedetomidine-a extremely selective 2A-adrenoceptor agonist that causes a widespread decrease in noradrenergic tone throughout cortical and subcortical structures-archetypally conserves consolidation, however results in reminiscence impairment due to a failure of data to be strongly encoded. Mathematical Modeling of Anesthetic Amnesia Attempts to model mathematically what happens to memory over time date again to the late nineteenth century, when Ebbinghaus128 demonstrated that memory decay is characterized by a rapid preliminary decline, followed by a more gradual loss. The most complete version of the Wickelgren Power Law is as follows: Neuroimaging Studies of Cortical Encoding Processes A small variety of useful neuroimaging research have evaluated the effect of anesthetics on cortical regional activation during memory encoding. Interpretation of this study in context of memory perform is troublesome, as a result of the experimental task was not memory-related. Further evidence for the relationships amongst arousal, attention, and encoding come from the mathematical modeling research described earlier. The examine design provided strong behavioral affirmation that encoding had occurred; subsequently, the hippocampal attenuation likely corresponded to a failure of consolidation processes. Dexmedetomidine attenuates the subsequent-memory effect-that is, dynamics of hippocampal activation become less predictive of subsequent memory, but the overall degree of hippocampal exercise appears preserved. In distinction to propofol, the explanation supplied here is that upstream cortical actions of dexmedetomidine weaken encoding, with attenuated hippocampal dynamics reflecting a downstream impact. Hippocampal attenuation throughout encoding has additionally been correlated with amnesia for face-name pairs for the benzodiazepine lorazepam and the cholinergic antagonist scopolamine. Attention is critical for the successful establishment of declarative memory,213 with distinct networks required for sustaining an alert state, orienting to targets, and for exerting govt management of thought. The dominant impact on attention for most anesthetic medicine is that of decreasing arousal, which of course progresses to profound sedation and unconsciousness as dose is elevated. There is a significant improve in hippocampus-rhinal spontaneous coherence within the band, however minimal modifications in other bands: the pattern is toward a slight lack of spontaneous coherence in the (4 to 8 Hz), (8 to 12 Hz), 1 (12 to 20 Hz), and a pair of (20 to 32 Hz) bands, and a slight enhance in the band. Hippocampal coherence dynamics, particularly within the and bands, are of critical importance to reminiscence perform, but interpretation of rest information have to be limited. This is especially true for coherence, for which the function in reminiscence seems to involve section reset in response to a stimulus.
Syndromes
- Vision impairment or blindness (with the early-onset forms of the disease)
- Avoid asthma triggers
- A bone projecting through the skin
- Inserting a tube into the belly to remove large volumes of fluid (called a paracentesis)
- Have you ever had this kind of itch before? What caused it then?
- Breathing difficulty
- What other symptoms do you have?
Generic betahistine 16mg without a prescription
Reported at the International Society for the Study of the Lumbar Spine Annual Meeting medicine vs nursing buy 16mg betahistine visa, 2006 symptoms vitamin b12 deficiency 16 mg betahistine order otc. Full-length posteroanterior and lateral radiographs are obtained in cases of spinal deformity to assess for world steadiness (coronal or sagittal). Lateral bending views can help determine the pliability of the curve and ranges for fusion. A basic evaluation as to whether a pedicle is instrumentable may be gained by inspecting its size on an anteroposterior radiograph of the pedicle. Pedicle width and length and starting factors can be decided from the axial picture. The arms are positioned at ninety levels or much less of abduction to minimize the likelihood of rotator cuff impingement. The arms are allowed to grasp down barely in a forward-flexed place about 10 levels. Degenerative Spondylolisthesis Iatrogenic instability Discogenic again pain Pseudarthroses Adult deformity Curve progression Table 1 Region Size Pedicle Morphology Lumbar Width decreases moving cephalad. General Points Narrowest in mediolateral dimension Horizontal angulation Angulation is medial at all levels except T12. Vertical angulation Angulation increases progressively to T2, then barely decreases. There is a big increase in superior angulation between L1 (2 degrees) and T12 (10 degrees). Proper placement of the chest and iliac pads allows for optimum restoration of sagittal alignment through gravity. Table 2 Region Proximal thoracic (T1�T3) Midthoracic (T4�T9) Distal thoracic (T10�T12) Lumbar Sacral Pedicle Screw Starting Points Starting Point Junction of the midpoint of the transverse course of and the lateral pars Junction of the proximal transverse process and the lateral third of the superior articular process Junction of the midpoint of the transverse process and the lateral pars Junction of the midpoint of the transverse course of and a couple of mm lateral to the pars At the inferolateral aspect of the L5�S1 side joint Approach Two approaches are used: the midline approach and the paraspinal method. The actual pedicle place to begin may vary significantly from the generally quoted "norms" in plenty of patients. In both the decrease (T10�12) and upper (T1�3) thoracic backbone, the entry level is on the junction of the bisected transverse course of and the lateral fringe of the pars interarticularis. In the lumbar spine, the entry level is at the midpoint of the transverse process and a pair of mm lateral to the pars interarticularis. The drill is advanced under fluoroscopic steering into the vertebral body to an ultimate depth of 35 to 40 mm within the lumbosacral spine, 25 to 30 mm in the lower and upper thoracic spine, and 30 to 35 mm in the midthoracic backbone. When resistance is met (cortex), the drill fails to advance, and consequently the angle is adjusted. This approach allows the instrument to search the right path within cancellous bone quite than being pushed forcefully via a cortical wall. The process is analogous to feeding a guidewire into a vein throughout central line placement: the thought is to present guidance, not pressure, to the instrument as it navigates a path throughout the cortical margins of the bone. For the S1 pedicle, the drill is directed 25 degrees medially and 10 levels inferiorly towards the sacral promontory. Bone ought to be encountered on the base of the tract as properly as alongside all 4 partitions of the pedicle. Medial and lateral cortical breaching is commonest because the pedicle is narrowest in this aircraft. A medial pedicle breach is most likely to occur at a depth between 15 and 20 mm ventral to the transverse process, which is the depth at which the spinal canal is encountered in most levels. However, if the start web site is simply too lateral, a lateral breach may happen extra superficially. A Kirschner wire is then positioned into the pedicle while the remaining pedicle tracts are cannulated. In common, pedicles are tapped 1 mm smaller than the diameter of the screw to be used to optimize screw buy. After tapping, the ball-tipped probe is again advanced via the pedicle tract to confirm that the pedicle cortices and anterior vertebral body are intact. The wound is copiously irrigated earlier than decortication to preserve the native bone graft generated with high-speed burring. Using a high-speed burr, the transverse process, the pars interarticularis, and the lateral wall of the aspect joint of each degree to be fused are decorticated. With the ball-tipped probe inserted in the pedicle path, a hemostat marks the length probe inserted. Once the bone graft has been placed, the Kirschner wires function figuring out landmarks for pedicle screw cannulation. Care is taken to advance the screw slowly in the identical angulation famous with the Kirschner wire in place. Modern pelvic fixation is most simply achieved by way of modular iliac screw placement. After dissection of the posterior superior iliac backbone, a place to begin is recognized 1. A burr or rongeur is used to create a recessed defect such that the iliac screw head will lie recessed throughout the posterior superior iliac spine. A gearshift is then inserted into the beginning point and advanced between the internal and outer tables of the pelvis, with the medial point of the probe scraping alongside the medial wall. The cortex of the medial wall is thicker than the lateral, and thus lateral violations are extra doubtless than medial violations. One, two, or three cross-links can be utilized, relying on the size of the assemble. If multiple cross-connectors are used, they want to be spread as far apart as possible from one another for maximal assemble rigidity. A claw figuration is composed of two hooks directed toward one another, separated by one or two ranges. It is useful to resect sufficient of the side in order that the lateral edge of the spinal canal is identified in order that it can be prevented throughout implant placement. They should be used with caution as a portion of the implant is positioned inside the spinal canal. Generally, placing two laminar hooks into the canal on the identical stage (eg, two downgoing hooks or two upgoing hooks on the same lamina) should be avoided to reduce implant volume in the canal until canal volume is capacious. The ligamentum flavum is dissected off the lamina, and the laminar floor receiving the hook is ready with a Kerrison rongeur so the hook might be flush in opposition to the bone. Although weaker than sublaminar or pedicle hooks, they keep away from violation of the spinal canal. Fluoroscopy can be used to establish correct pedicle starting factors when affected person anatomy is distorted. Too medial a starting point for pedicle screw entry might injure the supra-adjacent facet joint. A 1% infection price has been noted for discectomies, a 6% an infection fee for discectomies and fusion. Pseudarthrosis (nonunion rates, particularly crossing the lumbosacral junction) the incidence of nonunion after posterior lateral intertransverse fusion ranges from 3% to 25%. A wide range of fusion rates throughout the lumbosacral junction has been reported (22% to 89%).
Betahistine 16 mg purchase with visa
Chronic subluxation and dislocation are generally finest identified by testing the ankle by way of a variety of movement of inversion and plantarflexion to most eversion and dorsiflexion with resistance medications used to treat anxiety generic betahistine 16mg visa. Successful outcomes of nonoperative management vary from 14% in a study by Eckert and Davis4 to up to medications not to be crushed betahistine 16mg order visa 56% as reported by McClennan,9 whereas other investigators have also reported variable outcomes in small case collection. For sufferers with persistent subluxation, nonoperative treatment has not been proven to assist; normally pain and signs recur as quickly as the short-leg solid is eliminated. In addition, more athletic, higher-demand patients are likely to demand more dependable therapy and want to proceed with operative repair. The affected person is positioned in an oblique lateral position using a beanbag or large assist beneath the ipsilateral hip. An examination beneath anesthesia with provocative maneuvers such because the anterior drawer and rotary subluxation test could identify associated instability and locking or popping of the unstable peroneal tendons. Preoperative Planning Routine ankle radiographs are important to determine or rule out a rim fracture of the distal fibula, which occurs in 15% to 50% of all cases of peroneal subluxation. The retinaculum often is lifted off its fibular attachment, thus allowing the peroneal tendons to subluxate. Elevation of an anterior-based periosteal flap (outlined by dots) from the fibular groove has been completed. The tendons are relocated, after a groove-deepening process, into the recreated groove. If a shallow or convex fibular groove is current, we usually carry out a groove-deepening procedure. After the flap is raised, a groove-deepening process could also be carried out when indicated. Range the ankle to consider the gentle tissue restore, being certain that the tendons are free to move throughout the reconstructed peroneal tendon sheath. Close the pores and skin in usual style, and place the leg into acceptable dressings and splints with compressive bandages. Peroneal tendon dislocations predispose the tendons to longitudinal split tears as the tendon repeatedly subluxates around the posterolateral fibula. With peroneal tendons decreased, a "new gliding surface" and pocket of displaced superior peroneal retinaculum is evident. Trap door lowered in deepened fibular groove, with impactor being used to recess the bone and deepen the groove maximally. Peroneal tendons remaining decreased, even with out repair of the superior peroneal retinaculum. If not, then deepen the groove further with a larger-diameter drill bit and perform additional impaction of the posterior fibular floor. With tendons reduced, the pseudogroove is seen, with the displaced and attenuated superior peroneal retinaculum. Using a tamp longitudinally to shield the gliding floor of the posterior fibula during its impaction. The flap ought to preserve its continuity, anteriorly, with the fibrocartilage ridge. Flap-to-tendon adhesions Peroneal tendon tears Avoid overtightening the peroneal tendon sheath reconstruction. No issues with tendon-to-flap adhesions have been reported; nonetheless, early vary of motion starting at four weeks minimizes any probability of adhesions developing. Successful peroneal tendon discount with persistent signs secondary to peroneal tendon tears may result in a poor outcome. After four weeks the cast is eliminated and the patient is given a removable stiff-ankle rocker-bottom boot and remains non�weight-bearing for an additional 2 weeks while starting physical therapy with ankle range-of-motion workouts. At the end of 6 weeks the patient is progressed to weight bearing as tolerated in the brace, after which the affected person is weaned from the stiff-ankle boot and is started with ankle strengthening with inversion and eversion workout routines. The editor and coauthors of this chapter wish to acknowledge the contribution of Dr. Subluxation of peroneal tendons: case treated by rerouting tendons under calcaneofibular ligament. Superior peroneal retinaculoplasty: a surgical technique for peroneal subluxation. Often tendon injuries coexist with subluxation and dislocation and have to be handled simultaneously. If tendon pathology similar to a tear or degeneration is present and left untreated, ache may persist after surgical procedure no matter how properly the surgery was performed. Stenosing flexor tenosynovitis: Overtightening of the peroneal tendon sheath is pointless; the tendons simply have to remain reduced posterior to the fibula. Sural and superficial peroneal nerve injury Chapter 124 Repair of Dislocating Peroneal Tendons: Perspective 2 Florian Nickisch, Scott B. The acute damage usually remains unrecognized or is misdiagnosed as an ankle sprain. Untreated or misdiagnosed acute damage predisposes a affected person to recurrent peroneal dislocation, potential peroneal tendon tear, or chronic dislocation. Both buildings become tendinous before crossing the ankle joint and stay in a standard sheath. As they course distally the tendon of the peroneus brevis lies towards the posterior floor of the distal fibula, anterior and medial to the tendon of the peroneus longus. Distal to the fibula every tendon enters a definite tendon sheath, separated by the peroneal tubercle. The posterior surface of the distal fibula is covered by a layer of fibrocartilage to permit smooth gliding of the peroneal tendons. Note the vertical orientation of a portion of the superior peroneal retinaculum that corresponds to the orientation of the calcaneofibular ligament. In this case, practical rehabilitation leads to upkeep of tendon discount and complete recovery in about 50% of cases. Often a history of an inversion�supination sprain and attainable lateral ankle instability is reported. Localized tenderness over the posterior ridge of the fibula ought to raise suspicion for development of the injury to a peroneal tendon cut up tear. Tendon subluxation sometimes presents as snapping or popping and pain with eversion against resistance. The peroneal tunnel compression check consists of getting the patient carry out this movement whereas palpating the posterior border of the fibula. Chronic dislocation of the tendons is characterised by a palpable ridge over the lateral distal fibula typically associated with chronic swelling. Significant weakness of active eversion with out much pain ought to increase suspicion for a complete tear of the peroneal tendons. Peroneal dislocation may also happen as a sequela to severe calcaneal fractures with lateral displacement of the calcaneus.
Betahistine 16 mg lowest price
These may be assessed pathologically for polymorphonucleocytes per high-power area medicine purchase betahistine 16mg otc, as properly as for the presence of bacteria and poly debris medicine 5113 v generic betahistine 16mg visa. In instances of suspected or documented infection, consultation with the infectious illness group is suggested to decide the suitable microbiologic and chemotherapeutic elements of the following management. The approach is versatile as a end result of it may be used for both tibiotalar or tibiotalocalcaneal arthrodesis, with the only distinction being the size of the fixation device. Many different implant sizes can be used for this method, various from small- to large-fragment fixation, locking or nonlocking constructs, and fixed-angle or straight plates. The prone position also allows for the easiest medical dedication of hindfoot position earlier than fusion, and it affords entry to the posterior iliac crest for maximal quantities of bone graft procurement. This acts to compress the fusion mass beneath the load of weight bearing, facilitating a extra rapid return to ambulation. A rigorously contoured, anatomic polymethylmethacrylate antibiotic spacer impregnated with tobramycin and vancomycin can simply be inserted and removed by way of the identical approach to preserve alignment and soft tissue pressure between levels. Symptom manufacturing from the subtalar joint have to be rigorously assessed preoperatively (but can be assessed visually intraoperatively) to decide any potential need for adding subtalar fusion to an isolated tibiotalar arthrodesis. Surrounding bone quality and stock must also be a vital factor in making this willpower, particularly on the talar facet. Preoperatively, two-stage office-based or fluoroscopically guided diagnostic differential injections of the talocalcaneal and subtalar joints with native analgesic are nicely suited for this objective. A tourniquet ought to be positioned in regards to the thigh, and the ipsilateral posterior iliac crest should be squared off with preliminary drapes in anticipation of bone graft procurement. Imaging may be useful at times to establish this position ideally, though we prefer merely centering this over the ankle within the midline. No pores and skin retraction is used, and retractors are used only once the deeper tissues are encountered. The paratenon of the Achilles and the superficial fascia are first carefully opened with the intention of later closure and separation from overlying pores and skin and subcutaneous tissues in the rare occasion of wound breakdown. A Z-plasty of the Achilles is performed longitudinally to allow entry to the deep posterior compartment. Incising the fascia over the superficial posterior compartment can ease pressure and improve retractability of the gastrocnemius and soleus throughout publicity. The inferiormost edge of the peroneals could be removed subperiosteally from the distal fibula as wanted to gain access to the ankle joint in addition to to expose larger quantities of direct bleeding bone for surface-area healing of the fusion mass. Although not needed, this permits incorporation of the fibula in the fusion mass when desired. Use of a femoral distractor, or, alternatively, an exterior fixator with medial pins within the tibia and the calcaneus will facilitate distraction of the joint for easy implant removal within the occasion of sentimental tissue contracture. Once the ankle implants have been removed, any fibrous membrane or different particles inside the joint may be excised and the remnant viable bone stock (defect void) and quality could be assessed to plan alignment, bone graft requirements, and implant measurement for the reconstruction. Only healthy, bleeding bone should be left behind amidst a viable soft tissue envelope. At this point, the subtalar joint also needs to be inspected-and fused, if deemed essential by virtue of its integrity or the remaining out there bone stock for fixation. These ought to be taken ideally before antibiotic prophylaxis is given, and we suggest taking three samples for pathology and three for microbiology, all with separate devices, from separate sites, labeled with separate identifiers, and placed in separate sterile containers. Under no circumstances should the skin be touched when performing this task, for worry of inadvertent contamination. Since cultures are often not yet indicative of an infecting organism, both vancomycin and tobramycin must be included in the spacer for each gram-negative and grampositive protection. The infected patient is handled with adjunctive antibiotics for 6 to eight weeks, and infrequently an exterior fixator is added for extra assist (in lieu of a splint or cast). Before second-stage surgical procedure, the blood work ought to have returned to normal and the ankle should be reaspirated to verify eradication of infection. All incisions should also have healed uneventfully and be deemed capable of tolerating additional surgical procedure. At the time of staged reconstruction, the same posterior incision is used, and during exposure a stat Gram stain and frozen sections are taken to quantify white blood cells per high-power subject. If these values are within regular limits, the procedure then continues as outlined for main fusion within the aseptic affected person as indicated under. Occasionally this consists of choice of measurement or form (eg, tricortical, trapezoidal, cancellous only). Bone graft blocks are taken from the posterior iliac crest with a sagittal noticed and osteotomes, and thereafter are fashioned to match and bridge the resected ankle gap. Generally, tricortical grafts are most amenable to this assemble and can be easily contoured into appropriate place to maintain alignment. Once these are taken, the cancellous graft between the remaining internal and outer desk of the pelvis can be harvested for packing the remaining joint space. In all these circumstances the cancellous bone graft must be mixed with tobramycin and vancomycin powder before being packed into all remaining articular interstices after hardware implantation. Typically, this alignment includes 0 degrees of ankle flexion with 5 degrees of hindfoot valgus and external rotation appropriate to the alternative facet. Hence, as quickly as proper length and place are established clinically and radiographically, one or two eighth-inch Steinmann pins are positioned via the calcaneus from instantly inferiorly, and run into the midtibia to keep this alignment. Predrilling a trough for the blade of the plate is usually unnecessary when doing a tibiotalocalcaneal fusion because of the gentle cancellous bone found inside the calcaneus. In this case, the beginning position and angle of insertion are far more necessary. In the less common circumstance of having sufficient talar bone to merely fuse only the ankle primarily, a precut trough is advisable earlier than the blade plate is introduced into the denser talus bone. Once the blade plate is totally seated, the place of the limb clinically and radiographically ought to be reassessed. The remaining compressive screw fixation construct for the plate can then performed in routine fashion, together with the use of the articulating tensioning device where relevant. Often, several screws can be used to cross several joints not solely to enact a neutralization plate assemble but additionally to allow some articular compression throughout the fusion mass as properly. A Hemovac drain must be placed right now earlier than the overlying fascia, subcutaneous tissue, and pores and skin are closed. Steri-Strips should be utilized throughout the incision site to distribute stress optimally at this stage, and away from the incision itself. To this end, these ought to be uncut, and benzoin must be avoided to decrease blister formation. A meticulously padded Jones dressing, posterior splinting, and taped suction drainage help to avoid edema, hematoma, and pressure sore formation. While the patient recovers in bed or rests in a supine position, no pressure should be permitted beneath the lower leg, ankle, and foot. Hence, this space must be "suspended in midair" by putting pillows or blankets underneath the proximal calf, knee, and thigh to keep away from strain on the incision. The affected person ought to remain strictly non�weight-bearing for the primary 2 weeks postoperatively. After the posterior skin wound has healed and sutures have been eliminated, cast immobilization with partial weight bearing is allowed until week 6. Placing the plate posteriorly across the ankle creates a pressure band phenomenon through the gait cycle, serving to to compress the fusion website with weight bearing.
Betahistine 16mg order visa
The posterior longitudinal ligament (dashed yellow line) tends to be thicker and better defined centrally; it thins out laterally symptoms strep throat generic betahistine 16mg line. Thus medicine you can order online betahistine 16 mg cheap with amex, care have to be taken to hug the posterior floor of the uncinate to avoid injury to the exiting root. Depending on whether the concerned construction is the spinal cord or the nerve root, patients can current with symptoms of myelopathy, radiculopathy, or both. On examination, sufferers with radiculopathy may have motor, sensory, or reflex adjustments alongside the affected nerve root distribution. Patients could categorical exacerbation of radicular ache with specific head positions (ie, head positions that slender the scale of the neural foramen, such as neck extension with rotation to the affected extremity). The Spurling sign could be very helpful in differentiating cervical radiculopathy from extraspinal causes, such as cubital or carpal tunnel syndromes, as copy of symptoms ought to happen only with a cervical source of compression. In particular, radiculopathies involving numerous nerve roots, such as C5, C6, or C7, can all produce periscapular pain, not uncommonly in the absence of radiating ache down the arm. If doubtful as to the offending stage, a selective nerve root block can be performed for diagnostic functions. Another benefit to the microscope is that the view obtained by the assistant is identical as that of the operating surgeon. Positioning the patient is positioned with a bump under the scapula and the occiput on a foam doughnut to forestall stress necrosis. The quantity of extension tolerated preoperatively without extreme ache or neurologic signs is recreated. Approach A normal Smith-Robinson approach to the anterior cervical backbone is used for many circumstances from C2 to T2. Nonsurgical treatment usually includes bodily therapy, traction, pain medication, cervical collars, and epidural injections. When utilizing the microscope, it must be angled properly to present a parallel view of the disc house to facilitate decompression and endplate preparation. Endplate preparation should proceed in a parallel trend (dotted red lines) (A) centered on the disc house to obtain a rectangular space for graft insertion. Parallel, broad preparation of the disc house additionally makes decompression easier to carry out and ensures that the decompression is centered on the disc house (C). In distinction, the superior endplate of the caudal vertebra is flatter and requires much less preparation. To perform a safe but complete and adequate neural decompression, high-quality illumination and magnification are important. An important maneuver to facilitate disc area visualization and neural decompression is to take away the anterior portion of the inferior endplate of the superior vertebral body (the anterior lip). This floor is nearly at all times concave, with the anterior portion overhanging the disc house, thus preventing direct visualization of the posterior disc space. Use of the burr to fashion the endplates, alternating with use of the curettes and pituitary rongeur to remove cartilage and disc material, is carried out. Upslopes of uncinate Use of Distraction: Pins, Tongs, and Spreaders Intervertebral physique distraction pins can be positioned to gently distract the disc space and enhance visualization. Generally, this is carried out after an preliminary superficial discectomy, which permits higher disc space mobilization with the pins. If the disc space is fused in an overdistracted place, postoperative neck pain could result. The discectomy ought to start lateral (red lines) to the medial border of the uncinates. The upslope of the uncinate is clearly defined with curettes and Kerrison rongeurs till these borders are unquestionably identified. Having a wide discectomy allows for placement of bigger grafts or supplemental grafts within the uncinate areas. Creating parallel disc spaces facilitates graft�host bone contact, securing an intimate fit, in addition to permitting for wide decompression of spurs arising from the posterior disc space. More bone than traditional was faraway from the inferior portion of C6 due to the extensive spondylotic bar causing spinal cord compression along the floor of the canal on this patient. Because higher preparation of the inferior endplate on the cephalad vertebra is important, the surgeon ought to place the upper Caspar pin (C5) further away from the endplate (eg, in the midbody of C5 or more cephalad), while being cognizant of not entering the adjacent disc space above. The Caspar pins are positioned in the midline to keep away from compromising later screw fixation throughout plating. To achieve parallel distraction, the pins must be placed parallel to the disc house. If the ideas (ie, the leading ends) converge, relative kyphosis of the disc house happens with placement of the Caspar pin spreader and distraction; if the tips diverge, relative segmental lordosis occurs with placement of the Caspar pin spreader and distraction. An further benefit of the Caspar pins is that they help to retract the gentle tissues in a cephalad�caudal course without using a secondary set of retractor blades. Alternatively, a small laminar spreader can be utilized in the contralateral disc space as a substitute of Caspar pins to provide distraction. Thus, to obtain intimate contact of bone graft with each endplates, an oblong area is created by parallel decortication of the endplates. This usually requires higher preparation of the inferior endplate of the cephalad stage versus the superior endplate of the inferior stage. It is essential to not take away an excessive amount of bone off the inferior endplate of the cephalad level, nonetheless, as doing so limits the bone out there within the vertebra to accommodate a plate and screws. The creation of a parallel rectangular space within the disc space permits insertion of a graft appropriately sized to match the bigger top present at the heart of the disc space. Both endplates ought to be completely denuded of cartilage and decorticated to reveal bleeding bony surfaces to enhance the chance of profitable fusion. If major endplate resection is carried out during corpectomy, important settling or pistoning of the graft could occur (see Chap. The burr is used to thin down bone in the lateral facet of the canal (arrow) until only a thin shell is left. It is crucial to hug the posterior margin of the uncinate throughout this move to keep away from injuring the basis underneath, which exits the canal ventrolaterally at a few 45-degree angle. Instead, the surgeon ought to use the burr to skinny the uncus till the instrument can simply be handed into the foramen. Constant irrigation is carried out to prevent thermal harm and to clear away bone particles. If visualization is sufficient, continued thinning of the osteophyte can progress until only a thin shell of bone is left. The nerve root exits the spinal canal at roughly a 45degree angle, ventrolaterally. Foraminotomy is full when a micro nerve hook or curette can easily be passed into the foramen anterior to the exiting root without resistance. The uncinates outline the safe zone for the vertebral artery and the efficient zone for the decompression. It is crucial to define and preserve orientation with each uncinates at all times throughout anterior cervical surgical procedure. When curetting disc material on this space, a vertebral artery laceration might happen if the curette strays lateral to the lateral border of the uncinate. In many cases, a graft height of two to 3 mm more than that measured on the preoperative lateral movie would be the optimum alternative.
Betahistine 16 mg on line
This has been proven within the literature to be extremely successful for return to operate and discount or elimination of signs in appropriately selected sufferers symptoms magnesium deficiency buy 16 mg betahistine overnight delivery. When a affected person has misplaced dependable lateral delicate tissue structures by advantage of repetitive injury or previous failed procedures symptoms emphysema cheap betahistine 16 mg on line, an anatomic free graft lateral ligament reconstruction provides a very good alternative. Anatomic reconstruction coupled with the preservation of native peroneal tendon perform offers an optimum environment for return to function. No important variations were noted between operated and contralateral ankles with respect to vary of movement or uniaxial balancing. All patients were rated to have good or glorious outcomes with goal enchancment in talar tilt measurements (13 levels pre- vs 3 degrees postoperatively) and anterior drawer testing (on common, 10 mm pre- vs 5 mm postoperatively). Addition of tenodesis or interference screw fixation adds the benefit of with the flexibility to promote range of movement earlier with much less concern for graft loosening. In patients with insufficient local tissue, an augmentation is required to rebuild or reinforce the lateral ligaments. Depending on the severity of the sprain, one to three of the lateral ligaments are injured. Especially in dorsal extension, the talus is locked between the medial and lateral malleolus. There is some proof that special anatomic variations improve the risk of growing persistent ankle instability after an harm. Within the group of orthoses, semirigid, warped types present the best diploma of stability. The degree of incapacity skilled by the affected person depends upon the diploma of instability and the physical calls for. The examiner ought to examine the vary of movement of the ankle joint with a stretched and a bent knee to rule out a shortening of the gastrocnemius or soleus muscle (or both). Medial ankle stability is checked in a plantarflexed place of the ankle to keep away from a locking of the talus in the joint, which might mimic ligamentous stability. Insufficiency of the fibulocalcaneus ligament usually affects the stability of the subtalar joint. The stability is checked in dorsiflexion of the ankle to lock the talus within the upper ankle joint. Effusion may be palpated ventral, however smaller amounts of fluid are troublesome to detect. There are completely different options of tendon grafts, every with certain advantages and drawbacks. Tenodesis: the major drawback of tenodesis procedures (eg, Evans or Watson-Jones) is that they usually end up in persistent pain14,15 together with an increasing lack of stability over time. A native tendon that can easily be harvested with a minimal of donor site morbidity is the plantaris longus tendon. A technique has to be discussed with the affected person as to the means to proceed in this case. An option is to change to a method utilizing another transplant (eg, the gracilis or semitendinosus tendon). Examinations performed underneath anesthesia include range of motion of the ankle joint and the ankle stress tests to confirm the earlier results, with out an active stabilization of the ankle joint by the patient. Lateral approach with a 6- to 8-cm cut from the fibula toward the base of the fifth metatarsal. When the muscular fascia is break up, the soleus and the gastrocnemius may be bluntly separated. The tendon construction found medially between the 2 muscles is the plantaris longus tendon, which might simply be harvested with a tendon stripper. The plantaris longus tendon usually is way easier to identify at this location than on the medial facet of the calcaneus. After a longitudinal incision of the fascia, the plantaris longus tendon is discovered proper between the soleus and gastrocnemius muscle. The end of the plantaris longus is bolstered with a 0 nonabsorbable suture and stored in a moist compress. With a small Weber forceps, connect the ventral holes and flatten the sharp edges surrounding them. Drill another two holes at the lateral aspect of the neck of the talus with a diameter of three. In quite a couple of circumstances, remnants of the unique ligaments could be discovered at this location. Retract the peroneal tendons, and have the assistant place the hindfoot in most pronation. Drill two holes and connect them, 13 mm from the joint line of the subtalar joint, just like the approach mentioned earlier than. When bringing the transplant under tension, the foot ought to be in a impartial place. If there are parts of the transplant left, they can be utilized to augment the reconstructed ligaments and held in place with side-to-side sutures. If the plantaris longus tendon is too brief for the entire routing, use a single layer, where the native tissue is finest. Fracture of the bony bridges between the drill holes may be managed with anchors or with a transosseous suture of the graft. After 2 weeks they get an ankle brace for one more four weeks with full weight bearing in normal footwear. In addition, physiotherapy with active stabilization is began in the third week. Especially athletic sufferers profit from anatomic restore of the ligaments, which seems to produce extra dependable and significantly better results than tenodesis. Anatomic reconstruction of the lateral ligaments of the ankle using a plantaris tendon graft within the therapy of chronic ankle joint instability. Surgical treatment of continual lateral instability of the ankle joint: a new procedure. Ankle sensorimotor management and eversion power after acute ankle inversion injuries. Long-term consequence of anatomical reconstruction versus tenodesis for the remedy of persistent anterolateral instability of the ankle joint: a multicenter study. The medial longitudinal arch as a attainable risk factor for ankle sprains: a potential research in eighty three female infantry recruits. Tenodeses destroy the kinematic coupling of the ankle joint advanced: a three-dimensional in vitro analysis of joint movement. Reconstruction of the lateral ligaments of the ankle using a regional periosteal flap.