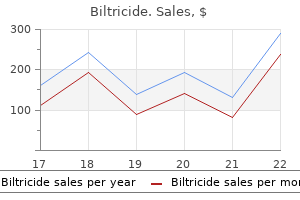
Biltricide
Biltricide dosages: 600 mg
Biltricide packs: 1 pills

600mg biltricide order otc
Pancreatic biopsy medications mobic 600mg biltricide fast delivery, if necessary treatment synonym cheap biltricide 600mg overnight delivery, reveals a lymphoplasmacytic inflammatory infiltrate with attribute IgG4 immuno staining, which can also be found in biopsy specimens of the maj or papilla, bile duct, and salivary glands, in type 1 auto immune pancreatitis. Imaging Plain movies present calcifications due to pancreaticolithiasis in 30% of affected sufferers. Occasionally, the findings elevate suspicion of pancreatic most cancers ("tumefactive continual pancreatitis"). Endoscopic ultrasonographic ("Rose mont") criteria for the prognosis of continual pancreatitis embrace hyperechoic foci with shadowing indicative of cal culi in the primary pancreatic duct and lobularity with honey combing of the pancreatic parenchyma. Characteristic imaging features of autoimmune pancreatitis embrace dif fuse enlargement of the pancreas, a peripheral rim of hypoattenuation, and irregular narrowing of the primary pancreatic duct. Sym ptoms and Signs Persistent or recurrent episodes of epigastric and left upper quadrant ache are typical. The ache leads to half from impaired inhibitory ache modulation by the central ner vous system. Other frequent complica tions embody typically brittle diabetes mellitus, pancreatic pseudocyst or abscess, cholestatic liver enzymes with or without jaundice, bile duct stricture, steatorrhea, malnutri tion, osteoporosis, and peptic ulcer. Pancreatic cancer develops in 4% of patients after 20 years; the chance could relate to tobacco and alcohol use. In patients with hereditary pancreatitis, the danger of pancreatic most cancers rises after age 50 years and reaches 19% by age 70 years (see Chapter 39). Treatment Correctable coexistent biliary tract illness must be treated surgically. Preferred brokers for ache are acet aminophen, nonsteroidal anti-inflammatory medication, and tramadol, together with pain-modifying agents corresponding to tricy clic antidepressants, selective serotonin reuptake inhibi tors, and gabapentin or pregabalin. Steatorrhea is treated with pancreatic supplements which are selected on the idea of their high lipase exercise (Table 1 6- 1 1). A complete dose of no less than 40,000 models of lipase in capsules is given with each meal (during and after the meal). Concurrent administration of a H 2 -receptor antagonist (eg, ranitidine, 1 5 0 mg orally twice daily), a proton pump inhibitor (eg, omeprazole, 20-60 mg orally daily), or sodium bicarbonate, 650 mg orally before and after meals, decreases the inactivation of lipase by acid and should thereby further decrease steatorrhea. In selected circumstances of alcoholic pancreatitis and in cystic fibrosis, enteric coated microencapsulated preparations might provide an advantage. However, in sufferers with cystic fibrosis, high dose pancreatic enzyme therapy has been related to strictures of the ascending colon. Pain secondary to idio pathic chronic pancreatitis could also be alleviated in some cases by means of pancreatic enzymes (not enteric coated) or octreotide, 200 meg subcutaneously thrice every day. Autoimmune pancreatitis is handled with prednisone forty mg/ day orally for 1 -2 months, followed by a taper of 5 mg every 2-4 weeks. Nonresponse or relapse occurs in 45% of kind 1 cases (particularly in these with concomitant IgG4 -associated cholangitis); rituximab is an efficient induction and maintenance agent, and azathio prine appears to reduce the risk of relapse. Endoscopic and Surgical Treatment Endoscopic remedy or surgical procedure may be indicated in persistent pancreatitis to deal with underlying biliary tract illness, guarantee free flow of bile into the duodenum, drain persistent pseu docysts, deal with different complications, remove obstruction of the pancreatic duct, try to relieve ache, or exclude pancreatic cancer. Distal bile duct obstruction may be relieved by endoscopic placement of a number of bile duct stents. In advanced instances, sub whole or total pancreatectomy may be thought of as a last resort but has variable efficacy and causes pancreatic insuf ficiency and diabetes mellitus. Perioperative administra tion of somatostatin or octreotide may scale back the danger of postoperative pancreatic fistulas. Endoscopic or surgical (including laparoscopic) drainage is indicated for symp tomatic pseudocysts and, in lots of instances, these over 6 em in diameter. Pancreatic ascites or pancreatico pleural fistulas due to a disrupted pancreatic duct could be managed by endoscopic placement of a stent across the disrupted duct. Pancreatic sphincterotomy or fragmenta tion of stones in the pancreatic duct by lithotripsy and endoscopic removing of stones from the duct might relieve pain in chosen patients. A single session of radiation therapy to the pancreas has been reported to relieve in any other case refractory ache. Medical management of hyper lipidemia, if current, can also prevent recurrent attacks of pancreatitis. In alcoholic pancreatitis, ache relief is most likely when a dilated pancreatic duct can be decompressed. In patients with disease not amenable to decompressive surgical procedure, dependancy to opioids is a frequent end result of treat ment. The high quality of life is poorer in patients with fixed pain than in these with intermittent pain. When to Refer All patients with chronic pancreatitis ought to be referred for diagnostic and therapeutic procedures. Prognosis Chronic pancreatitis often results in disability and reduced life expectancy; pancreatic most cancers is the primary reason for demise. Mortality, cancer, and comorbidities related to persistent pancreatitis: a Danish nationwide matched cohort study. Chronic pancreatitis pain pattern and severity are unbiased of belly imaging findings. Discomfort often occurs or worsens in the course of the premenstrual part of the cycle, at which period the cysts are most likely to enlarge. Fluctuations in size and speedy look or disappearance of a breast mass are common with this condition as are multiple or bilateral masses and serous nipple discharge. Patients will give a his tory of a transient lump within the breast or cyclic breast pain. Diagnostic Tests Mammography and ultrasonography should be used to evaluate a mass in a patient with fibrocystic condition. B ecause a mass because of fibrocystic condition is dif ficult to distinguish from carcinoma on the basis of scientific findings, suspicious lesions should be biopsied. General Considerations Fibrocystic situation is probably the most frequent lesion of the breast. There could additionally be an elevated threat in girls who drink alcohol, especially ladies between 1 8 and 22 years of age. The microscopic findings of fibrocystic situation embody cysts (gross and microscopic), papillomatosis, adenosis, fibrosis, and ductal epithelial hyperplasia. Although fibrocystic condition has typically been consid ered to enhance the chance of subsequent breast most cancers, only the variants with a element of epithelial proliferation (especially with atypia), papillomatosis, or elevated breast density on mammogram characterize true danger factors. Differential Diagnosis Pain, fluctuation in measurement, and multiplicity of lesions are the options most helpful in differentiating fibrocystic condi tion from carcinoma. If a dominant mass is current, the analysis of most cancers must be assumed until disproven by biopsy. Mammography could also be helpful, but the breast tissue in these younger ladies is normally too radiodense to allow a worthwhile research. Sonography is useful in differentiating a cystic mass from a strong mass, particularly in ladies with dense breasts. If no fluid is obtained by aspiration, if fluid is bloody, if a mass persists after aspira tion, or if at any time throughout follow-up a persistent or recurrent mass is noted, biopsy should be carried out.
Biltricide 600 mg safe
The dysfunction is normally sporadic treatment x time interaction 600mg biltricide trusted, however familial circumstances might occur and a variety of other genetic mutations or loci have been recognized medications for bipolar biltricide 600mg buy discount line. Symptoms and Signs Difficulty in swallowing, chewing, coughing, respiration, and talking (dysarthria) happen with bulbar involvement. The disorder is progressive, and amyotrophic lateral sclerosis is usually fatal inside 3-5 years; dying often outcomes from pulmonary infections. Patients with bulbar involvement typically have the poorest prognosis, while sufferers with primary lateral sclerosis often have a longer survival regardless of profound quadriparesis and spasticity. Progressive Bulbar Palsy Bulbar involvement predominates owing to disease pro cesses affecting primarily the motor nuclei of the cranial nerves. Pseudobulbar Palsy Bulbar involvement predominates in this variety additionally, but it is as a outcome of of bilateral corticobulbar disease and thus displays higher motor neuron dysfunction. Laboratory and Other Studies Electromyography may show modifications of continual partial denervation, with irregular spontaneous activity within the resting muscle and a reduction in the number of motor units underneath voluntary control. Motor conduction velocity is usually normal but may be barely decreased, and sensory conduction studies are additionally regular. The serum creatine kinase may be slightly elevated but never reaches the extraordinarily high values seen in a number of the muscular dystrophies. Progressive Spinal Muscular Atrophy that is characterized primarily by a lower motor neuron deficit in the limbs because of degeneration of the anterior horn cells within the spinal twine. Primary Lateral Sclerosis There is a purely upper motor neuron deficit in the limbs. Amyotrophic Lateral Sclerosis A combined higher and decrease motor neuron deficit is found in the limbs. This disorder is typically associated with cog nitive decline (in a sample in preserving with frontotemporal dementia), a pseudobulbar affect, or parkinsonism. Treatment Riluzole, 50 mg orally twice every day, which reduces the pre synaptic launch of glutamate, is the only treatment shown to improve short-term survival in amyotrophic lateral scle rosis in randomized trials. Noninvasive air flow a minimal of four hours per day in sufferers with a maximal inspiratory stress less than 60 em H 2 0 may delay survival. There is otherwise no specific remedy besides in patients with gammopathy, in whom plasmapheresis and immunosup pression could result in enchancment. Symptomatic and sup portive measures might include trials of anticholinergic drugs (such as trihexyphenidyl, amitriptyline, or atropine) or use of a transportable suction machine if drooling is bother some, braces or a walker to improve mobility, and physical remedy to stop contractures. Combination dextro methorphan/quinidine (20 mg/ 1 zero mg, one tablet orally a few times daily) could relieve signs of pseudobulbar affect. Behavioral modification (eg, exercising facial mus cles and encouraging frequent swallowing) or over-the counter decongestants can also help delicate drooling. Tracheostomy is typically performed if respiratory muscular tissues are severely affected; however, within the terminal phases of these issues, the focus of treatment ought to be on quality of life and actual istic expectations must be mentioned well prematurely. Motor and sensory conduction velocity may be measured in accessible segments of periph eral nerves. In axonal neuropathies, conduction velocity is normal or lowered only mildly and needle electromyogra phy provides proof of denervation in affected muscle tissue. In demyelinating neuropathies, conduction could additionally be slowed significantly in affected fibers, and in more severe cases, conduction is blocked completely, with out accompanying electro myographic indicators of denervation. General Considerations Diffuse polyneuropathies lead to a symmetric sensory, motor, or blended deficit, usually most marked distally. They embody the hereditary, metabolic, and toxic issues; idio pathic inflammatory polyneuropathy (Guillain-Barre syn drome); and the peripheral neuropathies which will occur as a nonmetastatic complication of malignant diseases. Multiple mononeuropathies counsel a patchy multifocal illness process similar to vasculopathy (eg, diabetes, arteritis), an infiltrative course of (eg, leprosy, sarcoidosis), radiation injury, or an immunologic disor der (eg, brachial plexopathy). When to Refer All sufferers (to exclude other treatable causes of symptoms and signs) must be referred. When to Admit Patients may must be admitted for initiation or titration of noninvasive ventilation, or for periods of elevated requirement of noninvasive ventilator assist during pul monary infections. Clinical Findings the trigger of polyneuropathy or mononeuritis multiplex is usually recommended by the historical past, mode of onset, and predominant clinical manifestations. The predominant patho logic characteristic may be axonal degeneration (axonal or neuro nal neuropathies) or paranodal or segmental demyelination. Cutane ous nerve biopsy might assist establish a exact diagnosis (eg, polyarteritis, amyloidosis). In about half of cases, no spe cific cause could be established; of these, slightly lower than half are subsequently discovered to be familial. There is often an autosomal dominant mode of inheritance, however occasional cases happen on a spo radic, recessive, or X-linked foundation. Clinical presentation could additionally be with foot deformities or gait disturbances in baby hood or early adult life. Slow progression results in the typi cal features of polyneuropathy, with distal weak spot and wasting that begin in the legs, a variable quantity of distal sensory loss, and depressed or absent tendon reflexes. Treatment Treatment is of the underlying cause, when possible, and is discussed under under the individual disorders. Physical remedy helps forestall contractures, and splints can major tain a weak extremity ready of helpful operate. To guard in opposition to burns, patients should check the temperature of water and sizzling surfaces with a portion of skin having normal sensation, measure water temperature with a ther mometer, and use cold water for laundry or decrease the temperature setting of their hot-water heaters. Shoes must be examined frequently during the day for grit or international obj ects in order to forestall pressure lesions. Patients with polyneuropathies or mononeuritis multi plex are subj ect to additional nerve damage at pressure factors and may subsequently avoid such conduct as leaning on elbows or sitting with crossed legs for lengthy periods. Neuropathic, burning pain could reply to simple anal gesics, such as aspirin or nonsteroidal anti-inflammatory agents, and to gabapentin (300 mg orally three times daily, titrated up to a most of 1 200 mg orally 3 times day by day as necessary). Opioids could additionally be essential for severe hyperpathia or ache induced by mini mal stimuli, however their use ought to be averted as much as attainable. [newline]Many patients experience episodic stabbing pains, which may respond to gabapentin, pregabalin (1 00 mg orally three times daily), carbamaze pine (start a hundred mg orally twice day by day, and titrate up to 400 mg orally twice daily), or tricyclic antidepressants (eg, amitrip tyline 1 0- 1 50 mg orally at bedtime daily). Postural hypotension is usually helped by put on ing waist-high elastic stockings and sleeping in a semierect place at evening. Fludrocortisone reduces postural hypo tension, but doses as excessive as 1 mg/day are typically nec essary for sufferers with diabetes and may result in recumbent hypertension. Erectile dysfunction and diarrhea are difficult to treat; a flaccid neuropathic bladder could reply to parasympathomi metic drugs such as bethanechol chloride, 10-50 mg three or 4 instances every day. Onset in infancy or childhood results in a progressive motor and sensory polyneuropathy with weak point, ataxia, sensory loss, and depressed or absent tendon reflexes. The periph eral nerves could also be palpably enlarged and are character ized pathologically by segmental demyelination, Schwann cell hyperplasia, and skinny myelin sheaths. The gait becomes ataxic, the hands turn into clumsy, and different indicators of cerebellar dysfunction develop accompanied by weak point of the legs and extensor plantar responses. Involvement of peripheral sensory fibers leads to sensory disturbances within the limbs and depressed tendon reflexes. In the central nervous system, changes are conspicuous within the posterior and lateral columns of the twine. Electrophysiologically, conduction velocity in motor fibers is regular or solely mildly reduced, but sensory motion potentials are small or absent. In the differential analysis for Friedreich ataxia are other spinocerebellar ataxias, a rising group of a minimal of 30 inherited disorders, each involving a special recognized gene.
Syndromes
- What drugs your child is taking. Include drugs, herbs, vitamins, or any other supplements you bought without a prescription.
- Depression
- Receiving a blood transfusion from a person who carries the parasite but does not have active Chagas disease
- Medicine to lower acetaminophen levels in the blood (N-acetylcysteine)
- Fluids through a vein (by IV)
- Total cholesterol: less than 200 mg/dL (lower numbers are desired)
- 7 - 12 months: 0.57* g/day
Buy generic biltricide 600 mg on line
The determination to provoke dialysis in sufferers with restricted life expectancy must be weighed in opposition to attainable deterioration in quality of life medicine 802 cheap 600 mg biltricide with mastercard. Diuretics symptoms nausea headache fatigue 600 mg biltricide buy free shipping, volume restriction, and opioids, as described in Chapter 5, could help lower the symptoms of volume overload. There is in all probability going little distinction in survival for well-matched peritoneal versus hemodialysis sufferers. Five-year Kaplan-Meier survival rates differ from 37% for patients with diabetes to 54% for sufferers with glomerulonephritis. Patients present process dialysis have a median life-expectancy of 3-5 years, but survival for as lengthy as 25 years could also be achieved depending on comorbidi ties. In addition to hypertension, physical exam ination might reveal an audible abdominal bruit on the affected facet. Unexplained hypertension in a girl younger than forty years is cause to display screen for this disorder. Chronic kidney disease and cardiovascular threat: epidemiology, mechanisms, and prevention. Clinical predictors of diagnostic testing utility within the initial evaluation of chronic kidney disease. Drug administration within the aged grownup with continual kidney disease: a review for the primary care physi cian. Role of sodium restriction and diuretic remedy for "resistant" hypertension in chronic kid ney illness. Practical approach to detection and management of persistent kidney illness for the primary care clinician. Imaging Abdominal ultrasound can reveal uneven kidney dimension when one renal artery is affected out of proportion to the opposite or small hyperechoic kidneys if each are affected. Doppler ultrasonography is very sensitive and particular (85% and 92% respectively in a meta-analysis of 88 studies) and relatively inexpensive. The sensitivities from numerous research vary from 77% to 98%, with less various specificities in a spread of 90-94%. Sensitivity is 77- 1 00%, although one research with explicit flaws showed a sensitivity of only 62%. Renal angiography is the gold normal for prognosis but extra invasive than the screening tests above. C0 2 subtrac tion angiography can be utilized instead of dye when the risk of dye nephropathy exists-eg, in diabetic patients with kidney injury. Lesions are most commonly found in the proximal third or ostial area of the renal artery. Fibromuscular dysplasia has a personality istic "beads-on-a-string" look on angiography. General Considerations Atherosclerotic ischemic renal illness accounts for most circumstances of renal artery stenosis. Approximately 5% of Americans with hypertension endure from renal artery stenosis. It happens mostly in these over 45 years of age with a historical past of atherosclerotic illness. A particular histologic pattern of glomerular harm results from this harm and could be seen on kidney biopsy. Options include medical administration, angio plasty with or with out stenting, and surgical bypass. However, blood pressure and serum creatinines are similar at 6 months of statement compared with each angio plasty and stents. Treatment of fibromuscular dysplasia with percutane ous transluminal angioplasty is commonly healing, which is in stark contrast to remedy for atherosclerotic causes. Renal artery stenosis: prevalence of, danger fac tors for, and administration of in-stent stenosis. In the "least severe" end of the nephritic spectrum, the findings of glomerular hematuria (ie, dysmorphic pink blood cells with a point of proteinuria) are characteristic. The nephritic syndrome, comprising glomerular hematuria, subnephrotic proteinuria (less than 3 g/day), edema, and elevated creati nine, falls within the mid-portion of the spectrum. Differentiating between a clinical presentation throughout the nephritic spectrum versus the nephrotic spec trum is necessary as a outcome of it helps slim the differential prognosis of the underlying glomerular illness (Tables 22-8 and 22-9). Glomerular diseases can also be categorised according to whether they cause only renal abnormalities (primary renal disease) or whether or not the renal abnormalities result from a systemic disease (secondary renal disease). Glomerulonephritis is a time period given to those illnesses that current in the nephritic spectrum and often signifies an inflammatory course of inflicting renal dysfunction. It may be acute, developing over days to weeks, with or without reso lution, or could additionally be more chronic and indolent with progres sive scarring. The presentation depends on the severity of the underlying irritation and the pattern of harm caused by the disease process. This is clinically mani fested by edema, first seen in regions of low tissue strain such because the periorbital and scrotal areas, and by hyperten sion. Heavy glomerular bleeding from inflammation may end in gross hematuria (smoky or cola-colored urine). General Considerations Postinfectious glomerulonephritis is most often because of infection with nephritogenic group A beta-hemolytic streptococci. It generally seems after pharyngitis or impetigo with onset 1 - three weeks after an infection (average 7- 1 0 days). These entities end in glomerular injury during active an infection, and are better termed "infection-related glomerulonephri tis" somewhat than postinfectious glomerulonephritis. Urinary microscopy reveals red blood cells which are misshapen or dysmorphic from traversing a broken glomerular filtration barrier. Important mor phologic information is gleaned from gentle, electron, and immunofluorescent microscopy. Symptoms and Signs Disease presentation can differ extensively throughout the nephritic spectrum from asymptomatic glomerular hematuria (espe cially in epidemic cases) to nephritic syndrome with hyper tension, oliguria, edema, and maybe gross glomerular hematuria (smokey-colored urine). Treatment General measures for all embody treatment of hypertension and of fluid overload if present. The inflam matory glomerular harm may require immunosuppressive agents (see specific diseases mentioned below). Glomerular hematuria and subnephrotic pro teinuria are current; extreme circumstances may reveal elevated serum creatinine and urinary red blood cell casts. Kidney biopsy reveals a diffuse proliferative pattern of injury on mild microscopy. Immunofluorescence demonstrates gran ular deposition of IgG and C3 within the mesangium and alongside the capillary basement membrane. When to Refer Any patient in whom a glomerulonephritis is suspected ought to be referred to a nephrologist. Treatment the underlying an infection must be identified and treated appropriately; in any other case, therapy for postinfectious glo merulonephritis is supportive.
600 mg biltricide with visa
In this way medications kidney damage cheap biltricide 600 mg amex, a subsequent elective one-stage sur gical operation can be carried out (if deemed necessary) during which the diseased phase of colon is removed and first colonic anastomosis carried out treatment 5th metatarsal fracture 600 mg biltricide buy with mastercard. Patients with continual illness leading to fistulas or colonic obstruction would require elective surgical resection. Indications for emergent surgical administration include generalized peritonitis, large undrainable abscesses, and scientific deterioration despite medical management and percutaneous drainage. Temporal trends within the incidence and natural historical past of diverticulitis: a population-based study. Routine colonoscopy after left-sided acute uncomplicated diverticulitis: a systematic review. Association between colonic diverticular dis ease and colorectal cancer: a nationwide population-based examine. American Gastroenterological Association Institute Guideline on the management of acute diverticulitis. For a full dialogue, see the section on Acute Lower Gastrointestinal Bleeding, above. Although most commonly sporadic, they might be inherited as part of a familial polyposis syndrome. Polyps could also be divided into four major pathologic teams: mucosal adenomatous polyps (tubular, tubulovillous, and villous), mucosal serrated polyps (hyperplastic, sessile ser rated polyps, and conventional serrated adenoma), mucosal nonneoplastic polyps (juvenile p olyps, hamartomas, inflammatory polyps), and submucosal lesions (lipomas, lymphoid aggregates, carcinoids, pneumatosis cystoides intestinalis). Of polyps eliminated at colonoscopy, over 70% are adenomatous; many of the the rest are serrated. Adenomatous polyps and serrated polyps have significant medical implications and shall be thought of additional under. Hyperplastic polyps situated in the proximal colon (ie, proximal to the splenic flexure) may be associ ated with an elevated prevalence of advanced neoplasia, particularly those bigger than 1 em. Symptoms and Signs Most patients with adenomatous and serrated polyps are completely asymptomatic. In a prospective comparative trial conducted in individuals at common threat for colorectal most cancers present process colonoscopy, the sensitivity for colorectal cancer for "Cologuard" was ninety two. Their significance is that over 95% of cases of adenocarcinoma of the colon are believed to arise from these lesions. Most adenomas are smaller than 1 em and have a low threat of turning into malignant; lower than 5% of these enlarge with time. Advanced lesions are believed to have a higher threat of harboring or progressing to malignancy. It has been estimated from longitudinal research that it takes a mean of 5 years for a medium sized polyp to develop from normal-appearing mucosa and 10 years for a gross cancer to arise. Most sessile serrated polyps and conventional serrated adenomas are believed to arise from hyperplastic polyps. It is believed that sessile serrated polyps and traditional ser rated adenomas harbor an elevated risk of colorectal cancer related or greater to that of adenomas. Both studies require bowel cleans ing with laxatives before the study and insertion of a rectal catheter for air insufflation during the examine. However, the accuracy for detection of polyps 5-9 mm in measurement is significantly decrease (sensitivity 50%). Endoscopic Tests Colonoscopy permits analysis of the complete colon and is the best technique of detecting and removing adenomatous and serrated p olyps. The latest era of capsule endoscopy of the colon has an 88% sensitivity and 82% specificity for detection of adeno mas larger than 6 mm compared with colonoscopy but only 29% sensitivity and 33% specificity for sessile serrated polyps. The bowel preparation required for the colon cap sule examine is more extensive than for colonoscopy and 1 0-30% of research could additionally be inadequate because of poor bowel preparation or failure to excrete the capsule. At this time, colonoscopy stays the best take a look at in most patients to detect colo rectal polyps. However, capsule endoscopy could also be thought of in patients with an incomplete colonoscopy or those who are unsuitable or unwilling to bear colonoscopy. Uptake of colon capsule endoscopy vs colonoscopy for screening relatives of patients with colorectal cancer. Endoscopic detection of proximal serrated lesions and pathologic identification of sessile serrated adeno mas/polyps vary on the idea of middle. Accuracy of capsule colonoscopy in detecting colorectal polyps in a screening population. Serrated polyps of the large gut: present understanding of prognosis, pathogenesis, and scientific man agement. Colonoscopic Polypectomy Most adenomatous and serrated polyps are amenable to colonoscopic elimination with biopsy forceps or snare cautery. Sessile polyps bigger than 2-3 em may be eliminated by snare cautery using quite a lot of strategies (eg, piecemeal or saline-lift assisted mucosal resection) or may require surgi cal resection. Patients with giant sessile polyps eliminated in piecemeal fashion ought to undergo repeated colonoscopy in 2-6 months to confirm complete polyp removing. Because the prognosis of those problems has important implications for therapy of affected members and for screening of relations, it is necessary to think about these issues in patients with a household historical past of colorectal most cancers that has affected multiple family member, those with a private or family history of colorectal cancer creating at an early age (50 years or younger), these with a personal or household historical past of a number of polyps (more than 20), and people with a personal or household historical past of multiple extracolonic malignancies. Postpolypectomy Surveillance Adenomas and serrated polyps can be present in 30-40% of patients when one other colonoscopy is performed within 3-5 years after the preliminary examination and polyp removal. Periodic colonoscopic surveillance is therefore recom mended to detect these "metachronous" lesions, which either could additionally be new or might have been missed through the preliminary examination. Most of those polyps are small, with out high-risk features and of little instant scientific signifi cance. The likelihood of detecting superior neoplasms at surveillance colonoscopy depends on the number, size, and histologic options of the polyps removed on preliminary (index) colonoscopy. Patients with 1 - 2 tubular adenomas smaller than 1 em (without villous options or high-grade dyspla sia) ought to have their next colonoscopy in 5 - 1 zero years. Patients with 3 - 1 0 adenomas, an adenoma larger than 1 em, or an adenoma with villous features or high-grade dysplasia ought to have their subsequent colonoscopy at three years. Patients with greater than 10 adenomas ought to have a repeat colonoscopy at 1 -2 years and may be thought of for evalu ation for a familial polyposis syndrome. Surveillance colo noscopy at 5 years is appropriate for patients with small (less than 1 em) serrated polyps with out cytologic dyspla sia; surveillance colonoscopy at three years should be consid ered for serrated polyps larger than 1 em and those with cytologic atypia. Pro p hylactic col ectomy recom mended to forestall otherwise i nevita ble colon cancer. Recent guidelines also advocate that genetic testing be consid ered in individuals with as few as 10 adenomas to exclude a analysis of attenuated disease. Treatment Once the diagnosis has been established, complete procto colectomy with ileoanal anastomosis or colectomy with ileorectal anastomosis is really helpful, often earlier than age 20 years. Ileorectal anastomosis affords superior bowel perform but has a 5% risk of development of rectal cancer, and for that purpose frequent sigmoidoscopy with fulgura tion of polyps is required. Upper endoscopic analysis of the stomach, duodenum, and periampullary area should be carried out every 1 - three years to look for adenomas or carci noma. Sulindac and celecoxib have been proven to decrease the number and dimension of polyps within the rectal stump however not the duodenum. Sym ptoms and Signs Colorectal polyps develop by a imply age of 1 5 years and most cancers at forty years. Unless prophylactic colectomy is per fashioned, colorectal cancer is inevitable by age 50 years.
Order biltricide 600mg overnight delivery
Patients who had cholestatic jaundice during preg nancy might develop it while taking contraception pills medicine 223 biltricide 600 mg for sale. The minipill is begun on the first day of a menstrual cycle after which taken continuously for as lengthy as contraception is desired medicine 93 948 biltricide 600 mg generic online. Advantages-The low dose of progestin and absence of estrogen make the minipill safe throughout lactation; it may increase the circulate of milk. Complications and contraindications Minipill customers usually have bleeding irregularities (eg, prolonged circulate, spot ting, or amenorrhea); such sufferers might have common being pregnant exams. Ectopic pregnancies are extra frequent, and complaints of stomach pain ought to be investigated with this in mind. Minor unwanted effects of mixture oral contraceptives corresponding to weight acquire and mild headache may occur with the minipill. Alterna tives, together with progestin only injections, implants, or intrauterine units, must be considered as first options instead of oral contraceptives. Minor facet effects-Nausea and dizziness could occur within the first few months of capsule use. Spotting or breakthrough bleeding between menstrual periods may occur, especially if a tablet is skipped or taken late; this can be helped by switching to a capsule of slightly greater efficiency (see part 3, above). A pregnancy check should be carried out if drugs have been skipped or if two or extra expected males strual durations are missed. There has been extensive worldwide expertise with this method over the past three decades. The medicine is given as a deep intramuscular injection of one hundred fifty mg each 3 months and has a contraceptive efficacy of ninety nine. Com mon unwanted effects embrace irregular bleeding, amenorrhea, weight acquire, and headache. Users commonly have irregular bleeding ini tially and subsequently develop amenorrhea. Both the American College of Obstetricians and Gynecologists and the Ameri can Academy of Pediatrics have recommended that adoles cents ought to be encouraged to think about long-acting reversible contraception strategies. In a big prospective study, a 75% reduction in unintended pregnancy was demonstrated with the usage of long-acting reversible contraception. Nexplanon, a radiopaque etonogestrel implant in combination with a next-generation applicator: three -year results of a noncomparative multicenter trial. The devices are highly efficient, with failure charges much like these achieved with surgical sterilization. I nsertion Insertion can be performed during or after the menses, at midcycle to stop implantation, or later in the cycle if the affected person has not become pregnant. Other Hormonal Methods A transdermal contraceptive patch containing 1 50 meg norelgestromin and 20 meg ethinyl estradiol and measur ing 20 cm 2 is on the market. The patch is applied to the decrease stomach, upper torso, or buttock once per week for three con secutive weeks, adopted by 1 week with out the patch. It seems that the typical steady-state focus of ethinyl estradiol with the patch is roughly 60% greater than with a 35 meg capsule. The mechanism of action, side effects, and efficacy are similar to those associated with oral contracep tives, though compliance may be higher. A contraceptive vaginal ring that releases 120 meg of etonogestrel and 15 meg of ethinyl estradiol daily is avail able. The ring is delicate and versatile and is placed within the higher vagina for three weeks, removed, and changed 1 week later. The efficacy, mechanism of motion, and systemic side effects are just like those related to oral contracep tives. Skin patch and vaginal ring versus combined oral contraceptives for contraception. She ought to be informed that any flu-like symptoms corresponding to fever, myalgia, headache, or nausea warrant imme diate medical attention for potential septic abortion. Diap hra g m & Cervica l Cap the diaphragm (with contraceptive jelly) is a secure and efficient contraceptive technique with options that make it acceptable to some ladies and never others. Failure charges range from 6% to 16%, depending on the motivation of the woman and the care with which the diaphragm is used. The advantages of this technique are that it has no systemic unwanted effects and offers significant safety in opposition to pelvic an infection and cervical dysplasia as properly as being pregnant. The disadvantages are that it should be inserted close to the time of coitus and that pressure from the rim predisposes some ladies to cystitis after intercourse. The cervical cap (with contraceptive jelly) is much like the diaphragm however fits snugly over the cervix solely (the diaphragm stretches from behind the cervix to behind the pubic symphysis). However, failure rates are 9% (perfect use) and 16% (typical use) in nullipa rous women and 26% (perfect use) and 32% (typical use) in parous women. The subsequent danger of pelvic infection seems to be primarily related to the chance of buying sexually transmitted infections. At the time of insertion, ladies with an elevated danger of sexually transmitted ailments should be screened for gonorrhea and Chlamydia. Contraceptive Foa m, Cream, F il m, Sponge, Jel ly, & Suppository these merchandise can be found without prescription, are straightforward to use, and are fairly effective, with typical failure charges of 1 0-22%. All contain the spermicide nonoxynol-9, which additionally has some virucidal and bactericidal exercise. The disadvantages of condoms are dulling of sensation and spillage of semen because of tearing, slipping, or leakage with detumescence of the penis. Two female condoms, one made from polyurethane and the opposite of synthetic nitrile, can be found in the United States. The reported failure charges vary from 5% to 2 1 %; the efficacy is comparable to that of the diaphragm. These are the only female-controlled method that gives vital safety from each pregnancy and sexually transmitted diseases. Ulipristal acetate prevents ovulation more effec tively than levonorgestrel: evaluation of pooled information from three randomized trials of emergency contraception regimens. The efficacy of intrauterine units for emer gency contraception: a systematic review of 35 years of expe rience. Abortion Since the legalization of abortion in the United States in 1 973, the associated maternal mortality rate has fallen mark edly, as a result of illegal and self-induced abortions have been replaced by safer medical procedures. Abortions in the first trimester of pregnancy are performed by vacuum aspira tion underneath native anesthesia or with medical regimens. Dila tion and evacuation, a variation of vacuum aspiration is mostly used within the second trimester. Techniques utilizing intra -amniotic instillation of hypertonic saline answer or numerous prostaglandins regimens, together with medical or osmotic dilators are occasionally used after 18 weeks. Sev eral medical abortion regimens utilizing mifepristone and a number of doses of misoprostol have been reported as being effective in the second trimester. Overall, legal abortion in the United States has a mortality price of less than 1: 1 00,000. Contraception Based on Awa reness of Ferti le Periods these methods are most effective when the couple restricts intercourse to the post-ovular phase of the cycle or makes use of a barrier methodology at different instances. Well-instructed, motivated couples might find a way to obtain low being pregnant charges with fertility awareness methods.
Biltricide 600mg discount visa
Clonidine given orally or transdermally medicine head biltricide 600mg buy otc, 1 00- 1 50 meg every day symptoms strep throat discount biltricide 600 mg without prescription, can also reduce the frequency of scorching flushes, however its use is limited by unwanted aspect effects, including dry mouth, drowsiness, and hypotension. There is a few proof that soy isoflavones may be effec tive in treating menopausal signs. Because little is known about opposed results, notably with long-term use, dietary supple ments ought to be used with caution. Natural Menopause Education and support from health suppliers, midlife dis cussion teams, and studying materials will help most ladies having issue adjusting to the menopause. Vasomotor symptoms-For ladies with average to severe vasomotor signs, estrogen or estrogen/proges tin regimens are the simplest approach to symptom reduction. Unless the affected person has undergone hysterectomy, a combi nation routine of an estrogen with a progestin corresponding to medroxyprogesterone, 1. There can be a patch obtainable con taining estradiol and the progestin levonorgestrel. Give estrogen on days 1 - 25 of every calendar month, with 5 - 1 zero mg of oral medroxyprogesterone acetate added on days 14-25. Withhold hormones from day 26 until the tip of the month, when the endometrium will be shed, produc ing a light, generally painless monthly interval. Vaginal atrophy-A vaginal ring containing 2 mg of estradiol could be left in place for three months and is suitable for long-term use. Short-term use of estrogen vaginal cream will relieve symptoms of atrophy, but because of variable absorption, remedy with both the vaginal ring or systemic hormone substitute is preferable. A low-dose estradiol pill (10 meg) is available and is inserted in the vagina day by day for 2 weeks and then twice a week for long-term use. A bland lubricant corresponding to unscented chilly cream or water-soluble gel can be helpful at the time of coitus. Although serum estrogen stage will increase associated with vaginal rings are lower than other routes of administration, it is strongly recommended that the ring be used with caution. Nonfat or low-fat milk merchandise, calcium fortified orange juice, green leafy vegetables, corn tortillas, and canned sardines or salmon consumed with the bones are good dietary sources. Vitamin D, at least 800 interna tional units/day from meals, daylight, or supplements, is important to enhance calcium absorption and keep bone mass. A daily program of energetic walking and exer cise to strengthen the arms and higher body helps maintain bone mass. Screening bone densitometry is really helpful for women beginning at age 65 (see Chapter 1). Women most in danger for osteoporotic fractures ought to consider bisphosphonates, raloxifene, or hormone substitute therapy. Risks of Hormone Therapy Double-blind, randomized, managed trials have shown no overall cardiovascular profit with estrogen-progestin alternative remedy in a bunch of postmenopausal girls with or with out established coronary illness. The examine additionally showed a small increase in the mixed threat of mild cognitive impairment and dementia with estrogen use in contrast with placebo, just like the estrogen-progestin arm. Surgical Menopause the abrupt hormonal lower resulting from oophorec tomy generally results in extreme vasomotor signs and rapid onset of dyspareunia and osteoporosis unless treated. If not contraindicated, estrogen alternative is generally started immediately after surgical procedure. The timing hypothesis for coronary coronary heart dis ease prevention with hormone remedy: past, current and future in perspective. Effects of vaginal estrogens on serum estradiol ranges in postmenopausal breast most cancers survivors and ladies susceptible to breast cancer taking an aromatase inhibitor or a selective estrogen receptor modulator. However, the dangers appear to be lower in ladies starting remedy at the time of menopause and higher in previously untreated women starting remedy lengthy after menopause. Therapy must be individualized as the chance profit profile varies with age and particular person threat factors. In the occasion of a desired pregnancy, prenatal care can begin early, and probably harmful medicines and activities corresponding to drug and alcohol use, smoking, and occupational chemical exposure could be halted. In the event of an unwanted preg nancy, counseling about adoption or termination of the pregnancy may be supplied at an early stage. Manifestations of Pregnancy the following signs and indicators are normally due to preg nancy, but none are diagnostic. A report of the time and frequency of coitus is useful for diagnosing and courting a pregnancy. Levels improve shortly after implantation, approximately double each forty eight hours (this rise can vary from 30% to 1 00% in regular pregnancies), reach a peak at 50-75 days, and fall to decrease ranges in the second and third trimesters. Pregnancy checks are performed on serum or urine and are accurate on the time of the missed period or shortly after it. Symptoms Amenorrhea, nausea and vomiting, breast tenderness and tingling, urinary frequency and urgency, "quickening" (per ception of first motion noted at concerning the 1 eighth week), weight achieve. Signs (in Weeks from Last Menstrual Period) Breast modifications (enlargement, vascular engorgement, colos trum) start to happen very early in pregnancy and continue till the postpartum period. Cyanosis of the vagina and cervical portio and softening of the cervix occur in in regards to the seventh week. Softening of the cervicouterine junction takes place within the eighth week, and generalized enlargement and diffuse softening of the corpus occurs after the eighth week. The uterine fundus is palpable above the pubic symphy sis by 1 2- 1 5 weeks from the final menstrual period and reaches the umbilicus by 20-22 weeks. Ultrasonography and a pregnancy take a look at will present correct prognosis in these circumstances. The onset of the final menstrual interval and its normality, attainable conception dates, bleeding after the last menstruation, medical history, all prior pregnan cies (duration, outcome, and complications), and symp toms of present being pregnant must be documented. Physical Examination Height, weight, and blood stress should be measured, and a basic bodily examination must be done, including a breast examination. Prenatal Visits Prenatal care should begin early and maintain a schedule of standard prenatal visits: 4-28 weeks, each 4 weeks; 28-36 weeks, each 2 weeks; 36 weeks on, weekly. Diet the affected person must be recommended to eat a balanced diet containing the main meals groups. Caffeine intake must be decreased to 0- 1 cup of cof payment, tea, or caffeinated cola day by day. The affected person must be advised to keep away from eating raw or uncommon meat as well as fish known to contain elevated lev els of mercury. Patients should be encouraged to eat recent fruits and vegetables (washed before eating). Sometimes compounding the above results on pregnancy consequence are the unbiased opposed results of illicit medicine. Cocaine use in pregnancy is related to an elevated threat of untimely rupture of membranes, preterm delivery, placental abruption, intrauterine progress restriction, neu robehavioral deficits, and sudden infant death syndrome. Similar opposed being pregnant results are related to amphetamine use, perhaps reflecting the vasoconstrictive potential of both amphetamines and cocaine. Adverse effects associated with opioid use embrace intrauterine development restriction, prematurity, and fetal dying.
Acrid Crowfoot (Buttercup). Biltricide.
- What is Buttercup?
- How does Buttercup work?
- Dosing considerations for Buttercup.
- Are there safety concerns?
- Arthritis, blisters, bronchitis, chronic skin problems, nerve pain, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96646
Cheap biltricide 600 mg mastercard
The prognosis partly is determined by the stage by which the lesions are encountered and the extent and severity of related organic illness conventional medicine buy biltricide 600mg fast delivery. A detailed history and repeated bodily examination can obviate the need for extensive laboratory testing treatment 34690 diagnosis biltricide 600 mg cheap with amex. Thyroid operate exams are useful, since hypothyroidism can produce a secondary fibromyalgia syndrome. The prognosis of fibromyalgia in all probability must be made hesitantly in a patient over age 50 and may by no means be invoked to clarify fever, weight loss, or another objec tive indicators. Hypophosphatemic states, corresponding to oncogenic osteomalacia, also wants to be included in the differential analysis of musculoskeletal pain unassociated with bodily findings. In distinction to fibromyalgia, oncogenic osteomalacia usually produces ache in just a few areas and is associated with a low serum phosphate degree. Cognitive behavioral remedy, together with applications that emphasize mindfulness meditation, is usually helpful. There is modest efficacy of amitriptyline, fluoxetine, duloxetine, milnacipran, chlorpromazine, cyclobenzaprine, pregaba lin, or gabapentin. Amitriptyline is initiated at a dosage of 10 mg orally at bedtime and gradually increased to 40-50 mg relying on efficacy and toxicity. Tramadol and acetaminophen combinations have ameliorated symptoms modestly in short-term trials. Hypertrophic pulmonary osteoarthropathy, which is characterised by the triad of polyarthritis, new onset of clubbing, and periosteal new bone formation, is associated with both malignant diseases (eg, lung and intrathoracic cancers) and nonma lignant ones (eg, cyanotic coronary heart illness, cirrhosis, and lung abscess). Cancer-associated polyarthritis is rare, has each oligoarticular and polyarticular forms, and should be con sidered when "seronegative rheumatoid arthritis" develops abruptly in an elderly affected person. Palmar fasciitis manifests as bilateral palmar swelling with finger contractures and will be the first indication of most cancers, notably ovarian carci noma. Palpable purpura due to leukocytoclastic vasculitis could be the presenting criticism in myeloproliferative problems. Hairy cell leukemia can be associated with medium-sized vessel vasculitis corresponding to polyarteritis nodosa. Acute leuke mia can produce j oint pains that are disproportionately extreme compared to the minimal swelling and heat which are present. Rheumatic manifestations of myelo dysplastic syndromes include cutaneous vasculitis, lupus-like syndromes, neuropathy, and episodic intense arthritis. Erythromelalgia, a painful warmth and redness of the extremities that (unlike Raynaud) improves with chilly publicity or with elevation of the extremity, is usually related to myeloproliferative ailments, particularly essential thrombocythemia. Inflammatory arthritis in sufferers with myelodysplastic syndromes: a multicenter retrospective research and literature evaluation of sixty eight circumstances. As normal muscle tone and pro tective reflexes are lost, secondary degenerative joint dis ease ensues, resulting in an enlarged, boggy, relatively painless j oint with extensive cartilage erosion, osteophyte formation, and multiple free joint our bodies. Radiographs can reveal putting osteolysis that mimics osteomyelitis or dramatic destruction of the joint with subluxation, frag mentation of bone, and bony sclerosis. Treatment is directed toward the first illness; mechanical devices are used to help in weight bearing and prevention of additional trauma. Charcot neuroarthropathy of the foot and ankle: diagnosis and administration methods. Periarticular pain with swelling and transient subcutaneous nodules may also occur. The knee and finger j oints are most commonly affected, but any peripheral j oint could also be concerned. Palindromic rheumatism must be distinguished from acute gouty arthritis and an atypical acute onset of rheumatoid arthritis. The most commonly affected sites are the proximal and distal femo ral heads, leading to hip or knee pain. Osteo necrosis of the jaw has been hardly ever related to use of bisphosphonate remedy, almost at all times when the bisphos phonate is used for treating metastatic most cancers or multiple myeloma rather than osteoporosis. Treatment entails avoidance of weight bearing on the affected joint for no much less than a quantity of weeks. For osteonecrosis of the hip, quite a lot of procedures designed to protect the femoral head have been developed for early illness, together with vascularized and nonvascular ized bone grafting procedures. Without a successful intervention of this nature, the natural history of avascular necrosis is often progres sion of the bony infarction to cortical collapse, resulting in significant joint dysfunction. Arachi donic acid metabolites, cytokines, and different mediators (such as chemoattractants) induce a late-phase inflamma tory response that seems several hours later in affected tissues when antigen exposure is steady (eg, pollen) or persistent. General Considerations Anaphylaxis is essentially the most critical and probably life threatening clinical manifestation of mast cell and basophil mediator launch. Anaphylaxis is defined clinically beneath the following circumstances: (1) an allergen exposure fol lowed by the acute onset of sickness involving skin or muco sal tissue and both respiratory compromise or hypotension (systolic blood strain less than 90 mm Hg or 30% lower than recognized baseline); (2) a possible allergen exposure fol lowed by the acute onset of two or more of the next conditions: pores and skin or mucosal tissue involvement, respiratory compromise, hypotension, and protracted gastrointestinal signs; or (3) a recognized allergen publicity followed by hypotension. IgE-dependent anaphylaxis is normally an acute syn drome initiated by a brand new allergen publicity after a prior silent exposure has sensitized the affected person with IgE antibod ies. The medical expression of allergic disease is determined by prior immunologic responsive ness, antigen exposure, and genetically influenced host factors similar to atopy. Atopic patients have a genetically aggregated predisposition to a restricted variety of disor ders: allergic rhinitis (Chapter 8), allergic asthma (Chapter 9), atopic dermatitis (Chapter 6), and IgE-mediated food allergic reactions. In addition, many mast cell and IgE dependent issues (eg, many drug and chemical sensi tivities, eosinophilic disorders, mast cell stability syndromes, continual urticaria) happen equally frequently in atopic and nonatopic persons. The timing of the onset of medical allergic syndromes after publicity to a suspected allergen serves as a helpful clini cal marker on which to base diagnosis and remedy. Reac tions will usually be both quick (generally occurring inside 60 minutes after preliminary exposure), or delayed, seem ing after many hours to days or weeks of antigen exposure. Symptoms and Signs Symptoms and indicators sometimes happen inside half-hour of initial exposure but may appear up to a number of hours later. These embody (in order of frequency): (1) pores and skin manifesta tions, sometimes urticaria but also flushing, blotchy rashes, and pruritus; (2) respiratory misery, together with wheezing, stridor, bronchospasm, and airway angioedema; (3) gastro intestinal signs, including cramping, emesis, and diar rhea (especially in meals allergy); and (4) hypotension, typically manifested as lightheadedness, dizziness, or syncope. The condition is potentially deadly, especially if untreated, and can affect each nonatopic and atopic persons. Within minutes after publicity to the allergen, a multivalent anti gen links adjacent IgE molecules, activating and degranu lating mast cells. Clinical manifestations could be explained by the consequences of launched mediators on track finish organs. Both preformed and newly generated mediators trigger vasodilation and permeability modifications, visceral easy muscle contraction, mucous secretory gland stimulation, B. Laboratory Findings Identification of anaphylaxis is medical as the necessity for treat ment is pressing. Elevated serum ranges of mast cell media tors, corresponding to tryptase and histamine, could also be detected shortly after a response providing assist to the prognosis. Referral to an allergy specialist is normal due to con cern for a future response and wish for applicable inter ventions and schooling. The constructive predic tive value of those exams is very depending on a suggestive temporal relationship to putative allergen publicity.
Buy cheap biltricide 600mg on line
Some sufferers have nonspecific complaints of continual con stipation medications known to cause pancreatitis generic 600 mg biltricide, belly ache medications used to treat fibromyalgia biltricide 600mg purchase with mastercard, or fluctuating bowel habits. It is unclear whether these signs are because of alterations within the colonic motility, visceral hypersensitivity, intestine microbi ota, or low-grade inflammation. Physical examination is usually normal however might reveal mild left decrease quadrant tenderness with a thickened, palpable sigmoid and descending colon. Patients in whom diverticulosis is discovered, particularly patients with signs or a historical past of difficult disease must be handled with a high-fiber food regimen or fiber supple ments (bran powder, l-2 tbsp twice daily; psyllium or methylcellulose) (see part on constipation). Retrospec tive research recommend that such therapy may lower the probability of subsequent complications. Recent advances in the therapy of colonic diver ticular illness and prevention of acute diverticulitis. Most sufferers with localized inflammation or an infection report delicate to moderate aching belly pain, normally in the left decrease quadrant. In many instances, symptoms are so delicate that the patient might not search medical consideration till a quantity of days after onset. Physical findings embody a low-grade fever, left decrease quadrant tenderness, and a palpable mass. Patients with free perforation present with a more dramatic picture of generalized stomach pain and peritoneal signs. Imaging In sufferers with delicate signs and a presumptive diagno sis of diverticulitis, empiric medical remedy is began with out additional imaging within the acute part. The pres ence of colonic diverticula and wall thickening, pericolic fats infiltration, abscess formation, or extraluminal air or distinction suggests diverticulitis. Endoscopy and colonogra phy are contraindicated in the course of the preliminary levels of an acute attack due to the risk of free perforation. Chronic irritation or an untreated abscess could result in fistula formation that will contain the bladder, ureter, vagina, uterus, bowel, and abdominal wall. Acute or chronic inflammation may lead to stricturing of the colon with partial or full obstruction. Sym ptoms and Signs Diverticulitis is outlined as macroscopic irritation of a diverticulum that may replicate a spectrum from inflamma tion alone, to microperforation with localized paracolic. Patients with mild symptoms and no peritoneal indicators may be managed initially as outpatients on a clear liquid diet. A 20 1 5 American Gastroenterological Association guideline suggests that antibiotics should be used selectively for uncomplicated illness. Reasonable regimens embrace amoxicillin and clavulanate potassium (875 mg/ 1 2 5 mg) twice day by day; or metronidazole, 500 mg 3 times day by day; plus either ciprofloxacin, 500 mg twice day by day, or trime thoprim-sulfamethoxazole, 1 60/800 mg twice daily orally, for 7- 1 zero days or till the affected person is afebrile for 3-5 days. Symptomatic enchancment usually occurs inside 3 days, at which era the diet could additionally be advanced. Patients with increasing pain, fever, or inability to tolerate oral fluids require hospitalization. Intravenous antibiotics must be given to cover anaerobic and gram-negative bacteria. Single-agent remedy with either a second-generation cephalosporin (eg, cefoxitin), piperacillin-tazobactam, or ticarcillin clavulanate appears to be as efficient as combina tion remedy (eg, metronidazole or clindamycin plus an aminoglycoside or third -generation cephalosporin [eg, ceftazidime, cefotaxime]). Intravenous antibiotics should be continued for 5-7 days, before changing to oral antibiotics. Prognosis Diverticulitis recurs in 1 0-30% of sufferers handled with medical management over 1 0-20 years. Nonetheless, colorectal most cancers might trigger symptoms that may be confused with diverticulitis. Presence of significant peridiverticular abscesses (4 em or larger) requiring possible percutaneous or surgical drainage. Patients with a localized stomach abscess four em in size or bigger are normally handled urgently with a percutaneous catheter drain placed by an interventional radiologist. This permits management of the infection and determination of the immediate infectious inflammatory pro cess. Adenomatous polyps of the duodenum and periampul lary area develop in over 90% of patients, resulting in a 5-8% lifetime threat of adenocarcinoma. Adenomas occur less regularly in the gastric antrum and small bowel and in those locations have a decrease risk of malignant transfor mation. Des maid tumors are domestically invasive fibromas, most com monly intra-abdominal, that may cause bowel obstruction, ischemia, or hemorrhage. H amartomatous Polyposis Synd romes Hamartomatous polyposis syndromes are rare and account for less than 0. Peutz-Jeghers syndrome is an autosomal dominant con dition characterised by hamartomatous polyps all through the gastrointestinal tract (most notably in the small intes tine) as properly as mucocutaneous pigmented macules on the lips, buccal mucosa, and pores and skin. The hamartomas may turn out to be large, resulting in bleeding, intussusception, or obstruction. Familial juvenile polyposis is also autosomal domi nant and is characterised by several (more than ten) juve nile hamartomatous polyps situated most commonly in the colon. There is an elevated threat (up to 50%) of adenocar cinoma because of synchronous adenomatous polyps or combined hamartomatous-adenomatous polyps. An increased price of malignancy is demonstrated in the thyroid, breast, and urogenital tract. Clinical Findings A thorough family most cancers history is crucial to determine households that could be affected with Lynch syndrome in order that appropriate genetic and colonoscopic screening may be offered. Owing to the constraints of genetic testing and the medical, psychological, and social implications that such testing might have, families should be evaluated first by a genetic counselor and give knowledgeable consent before genetic testing is carried out. Patients whose families meet any of the revised "Bethesda standards" have an increased probability of harbor ing a germline mutation in one of many mismatch repair genes and should be thought-about for genetic testing. The "Bethesda standards" are (1) colorectal cancer beneath age 50; (2) synchronous or metachronous colorectal or Lynch syn drome-associated tumor no matter age (endometrial, abdomen, ovary, pancreas, ureter and renal pelvis, biliary tract, brain); (3) colorectal most cancers with one or more first degree relatives with colorectal or Lynch syndrome-related cancer, with one of many cancers occurring before age 50; (4) colorectal cancer with two or extra second-degree relations with colorectal or Lynch syndrome-related cancer, regard less of age; (5) tumors with infiltrating lymphocytes, muci nous/signet ring differentiation, or medullary development pattern in patients youthful than 60 years. The Bethesda criteria establish roughly 70% of mutation-positive Lynch syndrome households however overlook 30%. For this cause, 2014 consensus, multisociety guide lines suggest that each one colorectal cancers ought to undergo testing for Lynch syndrome with both immunohisto chemistry or microsatellite instability. Universal testing has the best sensitivity for the diagnosis of Lynch syndrome and is cost-effective. Germline testing can be warranted in families with a powerful historical past consistent with Lynch syndrome when tumors from affected members are unavailable for evaluation. Affected individuals have a 22-75% lifetime danger of developing colorectal carcinoma and a 30-60% lifetime threat of endo metrial cancer, relying on the affected gene. Unlike people with familial adenomatous polyposis, sufferers with Lynch syndrome develop only a few adenomas, which can be flat and extra usually comprise villous features or excessive grade dysplasia.
Biltricide 600mg discount mastercard
The temporal artery is usually regular on bodily examination but may be nodular medicine misuse definition biltricide 600mg discount on-line, enlarged 300 medications for nclex biltricide 600 mg discount amex, tender, or pulseless. Blindness often results from the syndrome of anterior ischemic optic neuropathy, attributable to occlusive arteritis of the posterior ciliary department of the ophthalmic artery. The ischemic optic neuropathy of giant cell arteritis could produce no funduscopic findings for the first 24-48 hours after the onset of blindness. Asymmetry of pulses within the arms, a murmur of aortic regurgitation, or bruits heard close to the clavicle resulting from subclavian artery stenoses establish patients in whom big cell arteritis has affected the aorta or its maj or branches. Clinically evident large vessel involvement characterised mainly by aneurysm of the thoracic aorta or stenosis of the subclavian, vertebral, carotid, and basilar arteries-occurs in approximately 25% of sufferers with giant cell arteritis, sometimes years after the analysis. Subclinical massive artery disease is the rule: positron emis sion tomography scans reveal irritation within the aorta and its main branches in practically 85% of untreated sufferers. Forty percent of patients with large cell arteritis have non basic signs at presentation, chiefly respiratory tract problems (most incessantly dry cough), mononeuritis mul tiplex (most regularly with painful paralysis of a shoul der), or fever of unknown origin. Differential Diagnosis the differential prognosis of malaise, anemia, and striking acute section reactant elevations includes rheumatic diseases (such as rheumatoid arthritis, other systemic vasculitides, a number of myeloma, and other malignant disorders) and continual infections (such as bacterial endocarditis and osteomyelitis). Polymyalgia Rheu matica Patients with isolated polymyalgia rheumatica (ie, these not having "above the neck" signs of headache, j aw claudication, scalp tenderness, or visual symptoms) are treated with prednisone, 1 0-20 mg/ day orally. Usually after 2-4 weeks of treatment, slow tapering of the prednisone may be attempted. Most sufferers require some dose of pred nisone for no less than roughly 1 year; 6 months is too short generally. The addition of weekly methotrexate could improve the possibility of successfully tapering prednisone in some patients. Giant Cell Arteritis the urgency of early diagnosis and therapy in large cell arteritis relates to the prevention of blindness. Therefore, when a patient has signs and findings suggestive of temporal arteritis, therapy with prednisone (60 mg/day orally) must be initiated instantly and a temporal artery biopsy performed promptly. One study-too small and too prelimi nary to change the standard remedy suggestions talked about above-suggested that initiating treatment with intravenous pulse methylprednisolone might enhance the possibility that a patient with giant cell arteritis will achieve remission and be capable of taper off of prednisone. Retro spective studies recommend that low-dose aspirin (- eight 1 mg/day orally) could reduce the prospect of visual loss or stroke in sufferers with giant cell arteritis and must be added to prednisone within the initial treatment. Typically, a constructive biopsy exhibits inflammatory infiltrate in the media and adventitia with lymphocytes, histiocytes, plasma cells, and giant cells. An adequate biopsy specimen is crucial (at least 2 em in length is ideal), because the illness could also be segmental. Unilateral temporal artery biopsies are optimistic in roughly 80-85% of sufferers, however bilateral biopsies add incrementally to the yield (1 0- 1 5% in some research, less in others). Temporal artery biopsy is irregular in only 50% of patients with giant artery illness (eg, arm claudica tion and unequal upper extremity blood pressures). Prednisone should be continued in a dosage of 60 mg/ day orally for about 1 month earlier than tapering. Unfortunately, no extremely effective prednisone-sparing therapy has been identified. Methotrexate was modestly efficient in a single double-blind, placebo-controlled therapy trial however ineffective in one other. Thoracic aor tic aneurysms happen 17 occasions extra regularly in sufferers with large cell arteritis than in normal individuals and can outcome in aortic regurgitation, dissection, or rupture. The aneurysms can develop at any time but typically happen 7 years after the diagnosis of big cell arteritis is made. Rare in North America however more prevalent in the Far East, it primarily impacts ladies and usually has its onset in early maturity. Takayasu arteritis can present with nonspecific constitutional symptoms of malaise, fever, and weight loss or with manifestations of vascular damage (diminished pulses, unequal blood pres sures in the arms, bruits over carotids and subclavian arter ies, limb claudication, and hypertension). Corticosteroids (eg, oral prednisone, 1 mg/kg for 1 month, followed by a taper over several months to 1 0 mg daily) are the mainstays of therapy. The addition of methotrexate or mycophenolate mofetil to the prednisone could also be more practical than the prednisone alone. Takayasu arteritis has a continual relapsing and remitting course that requires ongoing monitoring and adjustment of therapy. Recent advances within the medical administration of Takayasu arteritis: an update on use of biological therapies. General Considerations Polyarteritis nodosa, described in 1 866, is acknowledged broadly as the first form of vasculitis reported in the medical literature. Currently, the term is reserved for necrotizing arteritis of medium-sized vessels that has a predilection for involving the skin, peripheral nerves, mes enteric vessels (including renal arteries), coronary heart, and brain, however polyarteritis nodosa can really involve nearly any organ. Polyarteritis nodosa is relatively rare, with a preva lence of about 30 per 1 million folks. Most instances of hepatitis B-associated disease happen within 6 months of hepatitis B an infection. A mutation in the gene for adenosine deaminase 2 has been recognized within the rare instances of familial polyarteritis. Laboratory Findings Most sufferers with polyarteritis nodosa have a slight anemia, and leukocytosis is common. A major challenge in making the prognosis of polyarteritis nodosa, nevertheless, is the absence of a disease-specific serologic test (eg, an autoantibody). Biopsy and Angiography the diagnosis of polyarteritis nodosa requires confirmation with either a tissue biopsy or an angiogram. Biopsies of symptomatic websites corresponding to pores and skin (from the sting of an ulcer or the middle of a nodule), nerve, or muscle have sensitivities of roughly 70%. The least invasive exams should normally be obtained first, however biopsy of an concerned organ is essential. If carried out by skilled clinicians, tissue biopsies nor mally have high benefit-risk ratios because of the impor tance of creating the analysis. Patients in whom polyarteritis nodosa is suspected-eg, on the premise of mesen teric ischemia or new-onset hypertension occurring in the setting of a systemic illness-may be identified by the angio graphic finding of aneurysmal dilations in the renal, mesen teric, or hepatic arteries. Angiography must be performed cautiously in patients with baseline renal dysfunction. Sym ptoms and Signs the clinical onset is usually insidious, with fever, malaise, weight loss, and other signs growing over weeks to months. Pain within the extremities is often a distinguished early feature brought on by arthralgia, myalgia (particularly affecting the calves), or neuropathy. The mixture of mononeuritis multiplex (with the most common discovering being foot-drop) and features of a systemic sickness is probably considered one of the earliest specific clues to the presence of an underly ing vasculitis. Polyarteritis nodosa is among the types of vasculitis most commonly related to vasculitic neuropathy. In polyarteritis nodosa, the everyday skin findings livedo reticularis, subcutaneous nodules, and skin ulcers replicate the involvement of deeper, medium-sized blood vessels. The most common cutaneous presentation is lower extremity ulcerations, usually occurring close to the malleoli.
Buy generic biltricide 600mg line
In immunocompromised and uncommon immunocompetent persons treatment 4 addiction biltricide 600 mg sale, cytomegalovirus medicine grinder 600 mg biltricide sale, Epstein Barr virus, and herpes simplex virus must be thought of within the differential analysis of hepatitis. Unidentified pathogens account for a small % age of instances of acute viral hepatitis. Laboratory proof of liver dysfunction could persist for a longer period, however most patients recover com pletely. Chronic hepatitis, characterised by elevated amino transferase levels for greater than 3-6 months, develops in 1 -2% of immunocompetent adults with acute hepatitis B however in as many as 90% of infected neonates and infants and a substantial proportion of immunocompromised adults. Patients with cirrhosis are at risk for hepatocellular carci noma at a price of 3-5% per year. Even in the absence of cirrhosis, patients with persistent hepatitis B-particularly these with energetic viral replication-are at increased threat for hepatocellular carcinoma. When to Refer Refer sufferers with acute hepatitis who require liver biopsy for analysis. An outbreak of hepatitis C in patients with immune deficiencies has occurred in some recipients of intravenous immune globulin. Hospital- and outpatient facility-acquired transmission has occurred via multidose vials of saline used to flush Portacaths; through reuse of disposable syringes; via drug "diversion" and tampering with injectable opioids by an infected well being care employee; by way of contamination of shared saline, radiopharmaceutical, and sclerosant vials; by way of inadequately disinfected endoscopy tools; and between hospital ized patients on a liver unit. Covert transmission during bloody fisticuffs has even been reported, and incarceration in jail is a threat issue, with a frequency of 26% in the United States. The incidence of recent cases of acute, symptomatic hepatitis C declined from 1 992 to 2005, however an increase was observed in persons aged 15 to 24 after 2002, as a end result of injection drug use. The incubation period for hepatitis C averages 6-7 weeks, and scientific sickness is commonly delicate, normally asymptomatic, and characterised by waxing and waning aminotransferase ele vations and a high rate (greater than 80%) of continual hepa titis. In pregnant sufferers with chronic hepatitis C, serum aminotransferase ranges incessantly normalize despite persistence of viremia, solely to enhance once more after delivery. Treatment In the past, treatment of patients with acute hepatitis C with peginterferon for 6-24 weeks was proven to apprecia bly decrease the danger of continual hepatitis. New oral direct-acting agents are actually supplanting interferon based mostly therapy (see Chronic Viral Hepatitis). These sufferers are in danger for decompensation and have a three fold increased risk of hepatocellular carcinoma. New cases are seen primarily in immigrants from endemic areas, including Africa, central Asia, Eastern Europe, and the Amazon region of Brazil. It is rare within the United States but ought to be considered in sufferers with acute hepatitis after a trip to an endemic space. In industrialized international locations, it may be spread by swine, and having a pet in the home and consuming undercooked organ meats are risk components. Reported extrahepatic manifestations embody arthritis; pancreatitis; monoclonal gammopathy; thrombocytope nia; and quite so much of neurologic problems, including Guillain-Barre syndrome and peripheral neuropathy. The danger of hepatic decompensation is elevated in sufferers with underlying continual liver disease. Nosocomial hepatitis C virus transmission from tampering with injectable anesthetic opioids. The total mortality price is less than 1 %, but the fee is reportedly larger in older individuals. Chronic hepatitis, which progresses very slowly in many instances, develops in as many as 85% of all individuals with acute hepatitis C. Patients with cir rhosis are at risk for hepatocellular carcinoma at a price of 3-5% per yr. Ful minant hepatic failure is characterised by the development of hepatic encephalopathy within 8 weeks after the onset of acute liver disease. Subfulmi nant hepatic failure occurs when these findings appear between 8 weeks and 6 months after the onset of acute liver disease and carries an equally poor prognosis. Acute-on persistent liver failure refers to acute deterioration in liver perform in an individual with preexisting continual liver illness. An estimated 1 600 cases of acute liver failure happen each year in the United States. Acetaminophen toxicity is the most common cause, accounting for a minimal of 45% of cases. Suicide makes an attempt account for 44% of instances of acet aminophen-induced hepatic failure, and unintentional overdoses ("therapeutic misadventures"), which are often a result of a decrease within the threshold toxic dose due to continual alcohol use or fasting and have been reported after weight reduction surgery, account for a minimum of 48%. Other causes embody idiosyncratic drug reactions (the second most typical trigger, with antituberculosis medicine, antiepileptics, and antibiotics implicated most commonly), viral hepatitis, poisonous mushrooms (Amanita phalloides), shock, hyper thermia or hypothermia, Budd-Chiari syndrome, malig nancy (most commonly lymphomas), Wilson illness, Reye syndrome, fatty liver of being pregnant and different issues of fatty acid oxidation, autoimmune hepatitis, parvovirus B 1 9 an infection and, hardly ever, grand mal seizures. Herbal and dietary supplements are thought to be contributory to acute liver failure in a considerable portion of cases, no matter trigger. Acute-on-chronic liver failure is often precipitated by an infection or an alcohol binge and alcoholic hepatitis. The decline of viral hepatitis as the prin cipal cause of acute liver failure is due to common vaccina tion of infants and youngsters in opposition to hepatitis B and the availability of the hepatitis A vaccine. Hepatitis C is a rare cause of acute liver failure within the United States, but acute hepatitis A or B superimposed on chronic hepatitis C could trigger fulminant hepatitis. Adrenal insufficiency and subclinical myocardial damage manifesting as an elevated serum troponin I degree usually complicate acute liver failure. Jaundice may be absent or minimal early, but laboratory checks show severe hepatocellular harm. In acetaminophen toxicity, serum aminotransferase elevations are sometimes towering (greater than 5000 units/L). In acute liver failure because of microvesicular steatosis (eg, fatty liver of pregnancy), serum aminotransferase elevations may be modest (less than 300 units/L). Over 10% of patients have an elevated serum amylase degree a minimal of thrice the upper restrict of normal, usually because of renal dysfunction. Treatment the treatment of acute liver failure is directed toward reaching metabolic and hemodynamic stability. Intravas cular volume should be preserved, but large-volume infu sions of hypotonic fluids ought to be avoided. To protect muscle mass and immune perform, enteral administration of protein, 1 - 1. Stress gastropathy prophylaxis with an H 2 -receptor blocker or proton pump inhibitor is recommended. Administration of acetylcysteine (140 mg/kg orally fol lowed by 70 mg/kg orally each four hours for a further 17 doses or 1 5 zero mg/kg in 5% dextrose intravenously over quarter-hour followed by 50 mg/kg over four hours after which 1 00 mg/kg over 16 hours) is indicated for acetaminophen toxicity up to 72 hours after ingestion. For large acet aminophen overdoses, treatment with intravenous acetyl cysteine could have to be prolonged in length till the serum aminotransferase levels are declining and serum acetaminophen ranges are undetectable. Treatment with acetylcysteine improves cerebral blood move and oxygen ation as well as transplant-free survival in sufferers with stage 1 or 2 encephalopathy because of fulminant hepatic fail ure of any cause. Nucleoside analogs are beneficial for patients with fulminant hepatitis B (see Chronic Viral Hepatitis), and intravenous acyclovir has shown benefit in these with herpes simplex virus hepa titis. Plasmapheresis mixed with D-penicillamine has been utilized in fulminant Wilson illness. Subclinical seizure exercise is widespread in sufferers with acute liver failure, but the value of prophylactic phenytoin is unsure.