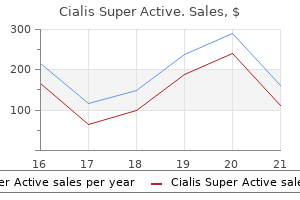
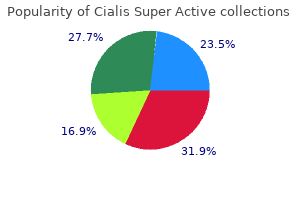
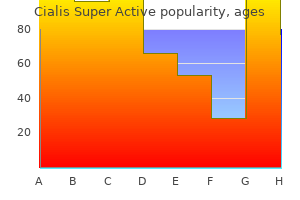
Cialis Super Active
Cialis Super Active dosages: 20 mg
Cialis Super Active packs: 10 caps, 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps

Cialis super active 20 mg purchase with mastercard
Patients with acute poliomyelitis present with fever erectile dysfunction drugs from canada cialis super active 20 mg purchase amex, headache erectile dysfunction caused by obesity cialis super active 20 mg discount online, myalgias, and gastrointestinal disturbance. Weakness, losing, and depressed reflexes start to appear during the first or second week of the sickness. The distribution of weak point typically is uneven, and the decrease extremities are most commonly concerned. The higher extremities, trunk, diaphragm, and bulbar muscular tissues are occasionally concerned. Strictly talking, this can be a disorder of the motor nerve and as such is discussed intimately in Chapter 29. Patients current with progressive, uneven weakness and losing that often affect the distal higher extremity muscle tissue first. Weakness is in the distribution of named motor nerves, usually with sparing of different nerves in the same myotome (clinical multifocal motor neuropathy). Occasional sufferers have weak point without losing, a discovering normally associated with pure demyelination. The disease is slowly progressive, with a male predilection, generally presenting before the fifth decade. Definite upper motor neuron signs are absent, though retained or inappropriately brisk reflexes for the diploma of weak spot and wasting may be seen. The characteristic discovering on motor nerve conduction research is that of conduction block, temporal dispersion, or both along the motor nerves. Other indicators of demyelination also could also be seen, including slowed conduction velocities, absent or impersistent F responses, and prolonged distal motor latencies. In the Goedee research, they determined that the optimum assessment was to inspect the bilateral median nerves within the forearms and upper arms combined with the bilateral trunks of the brachial plexus. In addition, antibody titers from the acute and convalescent phases might allow virus identification. Patients develop pain, fatigue, and weak point, typically most outstanding in the muscle groups beforehand affected by the poliomyelitis. However, muscle tissue that had been clinically normal might develop signs, reflecting the diffuse underlying nature of the earlier poliomyelitis. West Nile Encephalitis Over the previous a number of years, there have been an increasing number of reports of a "polio-like" syndrome associated with West Nile encephalitis. Jays, blackbirds, finches, warblers, sparrows, and crows appear to be most essential in maintaining the infection. Most infections in humans occur by the use of a mosquito bite, though instances have been reported following transplanted organs and infected blood merchandise. Because the disease is primarily spread to humans by mosquitoes, patients typically are affected in the summer and early fall. Fortunately, most infections with the West Nile virus are asymptomatic, with just one in 150 infections leading to neurologic involvement. After an incubation interval of several days, a nonspecific flulike illness develops, often with fever, headache, and joint and muscle ache. In some sufferers, there could also be further features suggestive of West Nile an infection, including retro-orbital pain, facial congestion, and rash. In patients with neurologic involvement, a mix of encephalitis, meningitis, and myelitis can happen. Other patterns of weakness are also seen, among them monoplegia, flaccid quadriplegia, bulbar weak point, and respiratory weak spot. In some sufferers, an acute segmental flaccid paralysis has been described as an preliminary presentation of West Nile virus, even in the absence of meningitis or encephalitis. Such cases have been initially attributed to Guillain-Barr� syndrome, although it now is clear that the weakness more likely is as a end result of of anterior horn cell illness. Rarely, patients have had irregular sensory conduction studies, suggesting involvement of the dorsal root ganglia or peripheral sensory nerve as nicely. The pattern of findings depends on when the examine is performed in relationship to the start of the sickness. Thus along with coxsackievirus, echovirus, and enterovirus, West Nile virus may be added to the list of infectious agents that can lead to an acute an infection of the anterior horn cells. Thus paralytic poliomyelitis is finest thought to be a scientific syndrome that can be brought on by quite lots of viruses, not simply the poliovirus. Experimental research have proven that retroviruses can induce a decrease motor neuron syndrome in mice and recommend a relationship between retroviruses and the pathogenesis of motor neuron disease. Although rare, an increasing variety of circumstances of poliomyelitis have been associated with this virus, either alone or in affiliation with encephalitis. Along with spastic paraparesis, sufferers usually have bladder dysfunction and minor sensory signs. The characteristic medical presentation is that of progressive, symmetric, proximal muscle weak point and atrophy, without upper motor neuron indicators. Among the varied types, probably the most extreme form happens in infancy (Werdnig-Hoffmann disease) and, if untreated, normally results in demise before the age of two. Others current in early childhood or throughout adolescence or maturity (Kugelberg-Welander disease) and have a much better prognosis. Although proximal muscle tissue are most regularly concerned, other anatomic variants have been described, including scapuloperoneal, facioscapulohumeral, and generalized varieties. It usually impacts solely males and has its onset between the third and fifth decades of life, followed by a gradual progression. Rare feminine carriers or these with two copies of the mutated gene (one on each X chromosome) could expertise cramps and fatigue. Some patients complain of exercise-induced muscle cramps and hand tremors several years earlier than weak spot develops. Proximal muscular tissues are affected first, followed by bulbar involvement, which may turn into marked. Dysarthria and dysphagia are associated with atrophy and weak spot of facial, jaw, and glossal muscle tissue. A classic and putting medical characteristic is the presence of facial fasciculations, most prominent across the mouth and chin. Fasciculations are present at relaxation, but they turn out to be extra outstanding with contraction and are best elicited by having the affected person whistle or blow out the cheeks. Sensory signs are rare, although some sensory loss may be current on examination. Although not universal, most sufferers have gynecomastia, and a few have other endocrine abnormalities, together with diabetes and infertility. Consequently, right analysis is important each for prognosis and for its worth in genetic counseling. Adult-Onset Hexosaminidase A Deficiency (Late-Onset Tay-Sachs Disease) Hexosaminidase A is a lysosomal enzyme essential within the metabolism of gangliosides. The adult-onset type of hexosaminidase A deficiency (also known as late-onset Tay-Sachs disease) is a uncommon, recessively inherited disorder, solely acknowledged in the late Nineteen Seventies. The adult-onset type is sort of different from the well-known quickly progressive childish type of hexosaminidase A deficiency, known as childish Tay-Sachs disease. An absolute deficiency of hexosaminidase A causes infantile Tay-Sachs disease, whereas a partial deficiency leads to the late-onset form.
Order 20 mg cialis super active with amex
The facial nerve is formed by the merging of the facial motor root and the adjoining nervus intermedius erectile dysfunction treatment by homeopathy purchase cialis super active 20 mg. Within the bony facial canal erectile dysfunction in diabetes patients cialis super active 20 mg online, a number of branches arise from and leave the main facial nerve. Parasympathetic fibers are given off to the higher and lesser petrosal nerves, bound for the pterygopalatine and otic ganglia. A small motor department arises next to innervate the stapedius muscle within the inside ear. The blue arrow signifies where fibers from the lingual nerve, a department of V3, join the chorda tympani fibers. After exiting the stylomastoid foramen, the facial nerve bifurcates into 5 major peripheral branches: temporal, zygomatic, buccal, mandibular, and cervical to provide the muscles of facial expression. Exiting from the lateral mid-pons, the trigeminal nerve divides into three main peripheral nerves-ophthalmic (V1), maxillary (V2), and mandibular (V3)-which arise from the trigeminal ganglion, positioned simply outdoors the brainstem on the petrous bone within the middle cranial fossa. The three branches of the trigeminal nerve-ophthalmic nerve (V1), maxillary nerve (V2), and mandibular nerve (V3)-supply sensation to the face and anterior scalp. Whereas the trigeminal ganglion contains cell bodies of the sensory fibers from each the principle sensory nucleus and the nucleus of the spinal tract of V, the cell bodies of proprioceptive sensory fibers from muscle spindles of trigeminal motor fibers are contained inside the mesencephalic nucleus of V within the midbrain. The three main peripheral nerve divisions of the trigeminal nerve are the ophthalmic (V 1), maxillary (V2), and mandibular (V3) nerves. Each nerve exits the cranium by way of a distinct opening: (1) the ophthalmic nerve by way of the superior orbital fissure, (2) the maxillary nerve via the foramen rotundum, and (3) the mandibular nerve by way of the foramen ovale. Each of the three main nerve branches accommodates sensory fibers, whereas motor fibers are carried solely in the mandibular nerve branches that supply innervation to the muscular tissues of mastication (masseter, temporalis, medial, and lateral pterygoid muscles) and to the anterior stomach of the digastric muscle, the mylohyoid, tensor veli palatini, and tensor tympani muscles. Unilateral facial nerve dysfunction can also be seen in affiliation with several disorders, mostly within the setting of diabetes. In addition, facial palsy occurs with herpes zoster involving the geniculate ganglion (Ramsay Hunt syndrome), lymphoma, leprosy, cerebellopontine angle tumors corresponding to acoustic neuroma, a quantity of sclerosis, stroke, and a number of different issues (Box 28. Bilateral facial weakness is much less common; it may be seen in Guillain- Barr� syndrome, Lyme illness, sarcoid, Melkersson-Rosenthal syndrome, tuberculous meningitis, and leptomeningeal lymphomatosis/carcinomatosis. Bifacial weak spot is also noted in some neuromuscular junction disorders and in varied muscular dystrophies. Either type of aberrant reinnervation may find yourself in synkinesis of facial movements. For example, closing the attention (orbicularis oculi) may be accompanied by movement of the lips (orbicularis oris). Clinically, these reinnervation abnormalities may differ from being very refined to very extreme. In essentially the most extreme case, synkinesis could lead to massive contractions on one facet of the face. As most individuals blink spontaneously each few seconds, synkinesis involving the orbicularis oculi and different facial muscle tissue can clinically appear similar to hemifacial spasm (see later), though the etiology is quite completely different. Aberrant reinnervation may also occur between the motor axons of the facial nerve and the parasympathetic axons. Thus, parasympathetic axons may innervate motor endplates, and, conversely, motor axons could innervate the parasympathetic endplates. This could result in lacrimation, salivation, and/or hemifacial sweating when the facial muscle tissue are activated. One can think about the embarrassing state of affairs whereby tears quite than saliva are produced while eating. The medical presentation of facial nerve palsy is dependent upon the situation, pathophysiology, and severity of the lesion. A central lesion (proximal to the facial nerve nuclei) causes contralateral weakness primarily of the lower facial musculature, with relative sparing of the orbicularis oculi and frontalis muscles, that are bilaterally innervated. Furthermore, with central lesions, there could additionally be facial movement throughout laughing or crying because the pathways that mediate responses to emotional stimuli are different from those that mediate voluntary facial movement. Peripheral lesions (at or distal to the facial nerve nuclei) trigger ipsilateral facial paralysis that impacts each the higher and decrease facial musculature, leading to an inability to wrinkle the forehead, close the attention, or smile. In addition, there may be dysfunction or absent style sensation over the anterior two-thirds of the tongue, relying on which branches are concerned as the nerve programs through the facial canal. The etiology is assumed to be inflammation of the facial nerve, which causes swelling and compression of the nerve within the facial canal. In most sufferers, the prognosis is great, with full restoration of function over a number of weeks to months. However, in additional severe instances, usually these related to important axonal loss, some permanent facial weak spot remains, or aberrant reinnervation may occur because the nerve regenerates. Aberrant reinnervation can take one of two types: (1) an axon that previously innervated a specific Hemifacial Spasm Hemifacial spasm is a chronic and infrequently progressive disorder normally related to chronic compression of or damage to the facial nerve. The disorder is characterised by involuntary contractions that have an effect on one or a number of muscles on one facet of the face. The spasms sometimes occur initially across the eye and later unfold to contain other ipsilateral facial muscle tissue. Although a quantity of uncommon causes of continual irritation are reported within the literature, the commonest etiology is an aberrant blood vessel mendacity involved with the facial nerve close to its exit zone from the brainstem. The spasms are thought to be generated by harm to some axons of the facial nerve with ephaptic transmission to different nearby axons. Surgical decompression of the blood vessel away from the facial nerve typically ends in full restoration. As famous earlier, large reinnervation and subsequent synkinesis of the facial muscular tissues could occur following an idiopathic facial palsy, leading to a sample almost identical clinically to hemifacial spasm. However, the underlying pathophysiology of hemifacial spasm (damage to the facial nerve with ephaptic transmission) differs from that of postparalytic facial syndrome (massive synkinesis that happens with spontaneous blinking, due to aberrant reinnervation of muscular tissues following idiopathic facial palsy). In addition, trigeminal neuropathy can be seen in affiliation with poisonous neuropathies, typically in isolation. Rarely, sufferers with local or metastatic most cancers current with isolated involvement of the mentalis branch of V3 (so-called "numb chin syndrome"). Isolated motor involvement of the trigeminal nerve is seen sometimes, often in affiliation with mass lesions or after surgery. The distribution of numbness is dependent upon the extent of nerve involvement and on which branches of the trigeminal nerve are concerned. Involvement of the motor branch causes issue chewing and deviation of the jaw to the contralateral aspect when opening the mouth. Stimulating three to four fingerbreadths lateral to the eye, recording the frontalis muscle; bilateral studies. Stimulating over the zygomatic bone just anterior to the ear, recording the nasalis muscle; bilateral studies. Stimulating over the angle of the jaw, recording the mentalis muscle; bilateral studies. Blink reflex research, stimulating the supraorbital nerve, recording orbicularis oculi muscles; bilateral studies. Needle electromyographic examination, examining muscular tissues from the most important branches, together with the frontalis (temporal branch), orbicularis oculi (zygomatic branch), orbicularis oris (buccal branch), and mentalis (mandibular branch). Blink reflex studies, stimulating the supraorbital nerve, recording the orbicularis oculi muscles; bilateral research.
Buy 20 mg cialis super active amex
It is seen at any age; nevertheless erectile dysfunction treatment in vijayawada cialis super active 20 mg purchase line, infants and youngsters aged 1 to 3 endure more severely than adults impotence drugs purchase cialis super active 20 mg line. For example, the chemotherapy medication used to treat some cancers may cause extreme anemia, or hepatitis can develop on account of a contaminated blood transfusion. A nosocomial infection seems 48 hours or more after hospital admission or inside 30 days after discharge. Sequela is a pathological situation that results from a prior disease, harm, or attack. Although a small percentage of overweight people are in a position to lose weight, a good smaller share are capable of preserve everlasting weight reduction. Obesity poses a severe danger for the event of hypertension and stroke, diabetes mellitus, gallbladder illness, and heart disease. Much media consideration relating to obesity has translated into more healthy choices out there at college cafeterias and eating places and a higher consciousness of meals decisions. Occupational therapists had been helpful in figuring out how Ian could probably be more productive in some kind of vocation. Only when the illness process is known are the most effective care and remedy potential. This was the third boat to go out that morning, and the primary two encountered no issues. Some of the passengers were trapped beneath deck within the overturned boat and tried to break through the glass obstacles to swim to the floor. Tonight they need to take the 2 boys, Jason and Kyle, to a baseball sport and their daughter, Miranda, to karate practice. Both Jayne and Brandon go away work a bit early to enable time to take the household to the local fast-food drive-through. Jayne and Miranda return to the baseball game as the coach is giving his successful gamers candy bars, soda, and chips. The family leaves for residence, and on the way, Miranda asks the boys to share their sweet and chips. Identify 5 groups of microorganisms, and provides an example of a illness caused by every. What is the leading cause of dying in the United States for those youthful than 35 Discuss malnourishment and vitamin/mineral deficiencies and the influence of poverty. The result of mineral deficiencies in the blood Discussion Qu estions/Personal Reflection 1. Nathan Zimmer lives in an area of northeastern Pennsylvania the place hydraulic fracturing for natural gas has elevated methane gas levels in his ingesting water. Sandi Smith lives in rural western Nebraska working outdoor a lot of the time managing her wheat farm. Some sufferers, though aware that their situation is perilous, get well their well being merely via contentment with the goodness of the doctor. Because he was a 7-year survivor of chronic lymphocytic leukemia, he was alert to signs which may sign a return of the illness. Jesse correctly made an appointment with his major care provider, who ordered blood checks. After a lot dialogue and agreement with the doctor, Jesse and Lexi decided to take their journey. During the holiday, Jesse and Lexi had been in a position to discuss remedy and what they hoped to do differently for this spherical of therapy. Congress) and the National Center for Health Statistics (part of the Centers for Disease Control and Prevention) indicate that over 38% of adults and 12% of kids in the United States are using some type of complementary and various drugs. Furthermore, Alan Mozes famous in a "Health Day" article in 2011 that health-care staff (doctors, nurses, their assistants, health technicians, and health-care administrators) are more apt to search some form of complementary medicine and/or therapy than the average inhabitants. The commonest complementary medical choices sought have been massage, yoga, acupuncture, Pilates, and natural medicines. Alternative can imply that one medical therapy is to be used instead of another. The authors use integrative to check with this model of care and complementary to refer to the therapies themselves. It should be famous that, more and more, integrative medication and alternative therapies actually do complement the extra conventional type of health care. The development of microscopy, bacterial cultures, radiography, vaccines, and antibiotics led medical science more into the germ concept of disease and away from the concept that a person had an important function to play in his or her own health. Medical colleges organized into varied departments, forcing students to focus their research on one organ at a time, impartial of all different organs. This terminology diverts attention away from the interrelatedness of all parts of the body as one entire particular person. This systembased method to drugs was coined allopathic drugs by the German physician and chemist Samuel Hahnemann (1755�1843), who questioned the inherent limitations of this form of treatment. Health was linked to concord, whereas disease was linked to disharmony or imbalance. Whether or not meant, his philosophy ultimately led to the separation of the "thoughts" from the "physique. There are a 26 Diseases of the Human Body variety of health-care points to tackle, nonetheless, as society advances towards such integration: 1. Controlling spiraling health-care costs ensuing from the necessity for and using increased expertise. Spending "little" to treat the cause for persistent disease but spending "much" when main sickness results. While progress has been made in a number of these areas, there still is a protracted method to go. Another technique of analysis considers the licensure of alternative practitioners. Although their number has tremendously elevated, not all are licensed or regulated of their apply by the states in which they work. Naturopaths are licensed in Alaska, Arizona, California, Connecticut, Hawaii, Idaho, Kansas, Maine, Minnesota, Montana, New Hampshire, Oregon, Utah, Vermont, and Washington. Many licensed practitioners incorporate a quantity of of the choice methods of therapy identified in their practices. Alternative Systems of Medical Practice There are a quantity of alternative medical systems to contemplate. Two of these alternative types are also classified as historic healing systems-Ayurveda and traditional Chinese drugs.
20 mg cialis super active cheap amex
The median and radial sensory amplitudes are regular erectile dysfunction rates cialis super active 20 mg effective, as are the latencies and conduction velocities erectile dysfunction doctors in orange county 20 mg cialis super active discount fast delivery. Next, non-ulnar C8�T1-innervated muscular tissues are sampled and are regular; likewise for the biceps, triceps, and low cervical paraspinal muscular tissues. There can be evidence of axonal loss in all ulnar-innervated hand and forearm muscles. Is this an odd case of persistent inflammatory demyelinating polyneuropathy solely affecting one nerve Calling a conduction block based mostly on this small quantity of amplitude drop would be diagnostically hazardous. With ultrasound, one can visualize the ulnar nerve from the wrist to the elbow and upper arm. The median nerve was imaged first on the wrist and was found to be completely normal in size, with regular echogenicity and fascicular structure. As the median nerve was followed to the forearm, antecubital fossa, and mid-arm, it remained completely regular. First, the nerve was recognized at the wrist, the place it was discovered to be enlarged at 15 mm2. From that time on, the nerve began to scale back in size in the mid-arm but was still markedly enlarged. This abnormal tissue seen between and inside the fascicles is a neural fibrolipoma, also referred to as a fibrolipomatous hamartoma among different names. This nerve tumor is benign and outcomes from growth of fibrous and adipose tissue around the nerve sheath and inside the nerve. Note the large enlargement in any respect locations (yellow arrows), particularly at the retrocondylar groove. Most importantly, note that the fascicles are nonetheless properly seen but with a large amount of hyperechoic tissue underneath the epineurium and between the fascicles. On ultrasound, it has the unmistakable look of an enlarged nerve (often dramatically enlarged) with hypoechoic fascicles and with extra tissue between the fascicles. Ultrasonography in sufferers with ulnar neuropathy at the elbow: comparison of cross-sectional area and swelling ratio with electrophysiological severity. Clinical, electrodiagnostic, and sonographic studies in ulnar neuropathy at the elbow. Position of the elbow in dedication of abnormal motor conduction of the ulnar nerve throughout the elbow. Practice parameter for electrodiagnostic studies in ulnar neuropathy on the elbow: American Academy of Electrodiagnostic Medicine, American Academy of Neurology, American Academy of Physical Medicine and Rehabilitation. Variations in anatomy of the ulnar nerve on the cubital tunnel: pitfalls in the prognosis of ulnar neuropathy at the elbow. Entrapment neuropathy of the ulnar nerve at its level of exit from the flexor carpi ulnaris muscle. Short phase incremental studies within the analysis of ulnar neuropathy at the elbow. Ulnar nerve lesions at the wrist: new approach for recording from the dorsal branch of the ulnar nerve. The analysis of suspected ulnar neuropathy at the elbow: normal conduction study values. Comparison of the flexed and prolonged elbow positions in localizing ulnar neuropathy on the elbow. Martin�Gruber anastomosis with anomalous superficial radial innervation to ulnar dorsum of hand: a pitfall when common variants coexist. Fibrolipomatous hamartoma of the proximal ulnar nerve associated with macrodactyly and macrodystrophia lipomatosa as an uncommon explanation for cubital tunnel syndrome. Ultrasonography in ulnar neuropathy at the elbow: relationships to scientific and electrophysiological findings. Sonographic incidence of ulnar nerve (sub)luxation and its related scientific and electrodiagnostic characteristics. The limitations of the dorsal ulnar cutaneous sensory response in patients with ulnar neuropathy at the elbow. Apparent conduction block in patients with ulnar neuropathy at the elbow and proximal Martin�Gruber anastomosis. Ultrasonographic swelling ratio within the diagnosis of ulnar neuropathy at the elbow. The differential analysis is limited and contains compression both exterior and inner to the wrist, the latter from varied structural lesions. Accordingly, neuromuscular ultrasound plays an necessary adjunctive function to electrodiagnostic research in the evaluation of those sufferers. The canal is shaped proximally by the pisiform bone and distally by the hook of the hamate. The floor is formed by a combination of the transverse carpal ligament and the adjoining hamate and triquetrum bones. After the hiatus, the superficial branch supplies sensation to the volar fifth and medial fourth digits and likewise provides motor innervation to the one remaining hypothenar muscle, the palmaris brevis. The deep palmar motor branch goes on to innervate the third and fourth lumbricals, the four dorsal and three palmar interossei, the adductor pollicis, and the deep head of the flexor pollicis brevis. Entrapment of the ulnar nerve at the wrist can take on several patterns: (1) pure motor affecting only the distal deep palmar motor department, distal to the hypothenar muscles; (2) pure motor affecting the proximal deep palmar department, including the hypothenar motor branches; (3) motor and sensory (proximal canal lesion); and barely (4) sensory affecting the superficial branch involving the sensory fibers to the volar fourth and fifth fingers. Patients present with painless weakness and atrophy of ulnar intrinsic hand muscle tissue. Because the ulnar-innervated adductor pollicis and deep head of the flexor pollicis brevis are within the thenar eminence, both the hypothenar and thenar eminences could additionally be wasted, if the lesion is in the proximal deep palmar motor branch. In addition, one other somewhat obscure signal, generally known as the "palmaris brevis sign," could additionally be seen in severe lesions of the deep palmar motor department. Remember that the palmar brevis is the one muscle equipped by the superficial department and is therefore spared in lesions of the deep department. When the palmaris brevis contracts, it ends in puckering of the skin along the proximal medial border of the hand. In more proximal lesions, the superficial department may also be affected, leading to sensory disturbance of the volar fifth and medial fourth digits. This is a vital scientific point to keep in mind when trying to discern if the ulnar nerve lesion is at the wrist or extra proximal. In addition, the proximal volar medial hand ought to be spared as a outcome of the palmar cutaneous department also arises simply proximal to the wrist. Rarely, an anomalous muscle or different mass lesions have been reported, together with ulnar artery aneurysms, lipomas, and different tumors.
Purchase 20 mg cialis super active overnight delivery
Examination subsequently reveals marked weakness in the distribution of both the deep and superficial peroneal nerves (ankle and toe dorsiflexion and ankle eversion erectile dysfunction effects on relationship cheap cialis super active 20 mg without prescription, respectively) erectile dysfunction weight loss cialis super active 20 mg order mastercard. This is doubtlessly a very important sign because it suggests weak spot of the tibialis posterior, a non-peroneal-innervated muscle. If foot inversion truly is weak, an isolated lesion of the peroneal nerve is excluded. Other tibial-innervated muscular tissues are regular, however, together with ankle and toe plantar flexors. In addition, the ankle reflex, mediated by the tibial and sciatic nerves, is regular and symmetric. The sensory examination is normal over the lateral foot, sole of the foot, and medial calf, representing the territories of the sural, plantar, and saphenous nerves, respectively. In addition, sensation over the proper lateral knee, the distribution of the lateral cutaneous nerve of the knee, is normal. Abnormalities found in any of those territories would suggest a lesion more proximal to the peroneal nerve. There is a well-demarcated loss of sensation to pinprick and temperature over the dorsum of the foot and the lateral calf. However, stimulating above the fibular neck in the lateral popliteal fossa demonstrates a marked decrease in amplitude with slowing of conduction velocity into the demyelinating vary (20 m/s). The F responses are absent on the best but are present and regular on the contralateral side. The superficial peroneal sensory response is obtained subsequent on the right and reveals a standard amplitude, in comparison with population norms. However, in contrast with the contralateral side, the responses are clearly asymmetric. On the involved right side, the sural response is normal and much larger than the superficial peroneal sensory response. Because the distally recorded superficial peroneal sensory response is considerably decrease in amplitude than that recorded on the contralateral facet, there must even be some axonal degeneration. However, comparison of the peroneal motor studies from aspect to aspect reveals little asymmetry, which means that the amount of axonal loss most likely is sort of mild. That muscle requires specific attention as a outcome of its major function is foot inversion, which can have been slightly weak on examination. Any abnormality in the tibialis posterior implies a extra widespread lesion beyond the peroneal nerve. An extra tibial-innervated muscle, the medial gastrocnemius, is sampled and found to be regular. Next, both the short and lengthy heads of the biceps femoris are sampled and found to be normal. Finally, a more proximal non-sciatic L5-innervated muscle, the gluteus medius, is sampled. This decrease can happen both from demyelination and conduction block or from disruption of axonal continuity. The time course depends on the length of the nerve between the muscle being studied and the location of injury. In peroneal neuropathy on the fibular neck associated with axonal loss, fibrillation potentials will occur in the peroneal-innervated muscular tissues in the calf solely after 2�3 weeks. Reinnervation following denervation generally takes many weeks and often months to happen. In this case, the affected person most likely developed a peroneal neuropathy from extended immobilization on the time of his surgery. It can be potential that his being thin could have predisposed him to this complication. How Does One Explain the Mild Weakness of Foot Inversion if the Lesion Is Purely Peroneal Although the diagnosis of a peroneal neuropathy at the fibular neck initially appeared doubtless from the historical past and examination, the potential of weak point of foot inversion put that clinical analysis in query. However, any vital weak spot ought to at all times counsel dysfunction of the tibialis posterior and thus suggest a extra proximal lesion. The electrophysiologic research has localized the lesion and accurately assessed its time course. Last and probably most essential is the evaluation of the underlying pathophysiology, both axonal loss or demyelination. It is well known that the variety of fibrillation potentials correlates poorly with the diploma of axonal loss. Determining the underlying pathophysiology is of special importance in assessing the prognosis. In basic, the prognosis for a demyelinating lesion is rather more favorable than that for an axonal loss lesion. In demyelination, the underlying axon stays intact, and the restore course of consists solely of remyelination. In distinction, recovery from axonal loss lesions requires regrowth of the terminal axon or collateral sprouting from adjoining unaffected axons. Each of these processes often is kind of sluggish (axonal regrowth happens at approximately 1 mm/day) and can be incomplete. A affected person with severe axonal loss in the peroneal nerve on the fibular neck doubtless would require many months and probably well over a 12 months to recuperate operate. In contrast, a patient with a demyelinating peroneal neuropathy could get well fully over 1�2 months. Such fast restoration, in fact, presumes that the cause for the peroneal neuropathy is no longer present, as is true within the case mentioned right here by which the peroneal neuropathy doubtless was because of extended compression on the fibular neck during the anesthesia and surgical procedure. Note that the tibialis anterior originates within the higher two-thirds of the lateral floor of the tibia (green arrow) and inserts into the medial cuneiform and first metatarsal bones of the foot (red arrows). Its major motion is to dorsiflex the foot but it also acts as a secondary foot inverter. However, patients with a foot drop from peroneal neuropathy could seem to have slight weak point of foot inversion for two reasons. This is just like testing finger abduction with the hand in a dropped wrist position. Ultrasound and neurophysiological correlation in widespread fibular nerve conduction block at fibular head. Diagnostic worth of high-resolution sonography in common fibular neuropathy at the fibular head. More frequent are lesions of the lumbar plexus or L2�L4 nerve roots, which may present with signs and indicators just like femoral neuropathy. Especially in milder instances, differentiating amongst these three forms of lesions may be fairly troublesome. In the pelvis, the nerve emerges from behind the psoas muscle to run laterally, deep to the iliac fascia above the iliacus muscle. Muscular branches are first given off to the psoas and then to the iliacus muscles (which distally merge to turn into the iliopsoas muscle) before the nerve runs beneath the inguinal ligament. The femoral nerve enters the thigh lateral to the femoral artery, beneath the inguinal ligament, dividing roughly four cm below the inguinal ligament into anterior and posterior divisions.
Cialis super active 20 mg generic
Note that if the medical examination suggests weakness past the radial distribution erectile dysfunction joliet cialis super active 20 mg purchase without a prescription, investigation for a more widespread neuropathy is indicated erectile dysfunction doctors buy 20 mg cialis super active free shipping, especially a search for conduction blocks along other motor nerves, which may indicate multifocal motor neuropathy with conduction block (see Chapter 29). At least one radial-innervated muscle proximal to the bifurcation of the primary radial nerve near the elbow however distal to the spiral groove. Itisdeepanddifficult � T to localize and sometimes is spared in posterior interosseous neuropathy. However, there are unique traits and limitations of sure muscular tissues, including: � A nconeus. The anconeus can basically be considered an extension of the medial head of the triceps. Thus, in severe or complete radial neuropathies on the spiral groove, each radial-innervated muscle within the forearm (which includes every wrist and finger extensor), in addition to the supinator and brachioradialis, may be completely denervated, and only the anconeus might be normal. Thus, these muscle tissue are very helpful in determining if the lesion is at the level of the posterior interosseous nerve, oraboveit,intheregionoftheelbow. Second, a lot of supination is subserved by the biceps muscle (the primary operate of the biceps is elbow flexion; its secondary perform is forearm supination). Third, the supinator and its relationship to the radial nerve are considerably akin to that of the pronator teres and the median nerve: the deep branch of the radial nerve runs through the supinator muscle at which level it is recognized as the posterior interosseousnerve. However,thebranchorbranches supplying the supinator originate from the deep radial motor department before it enters under the Arcade of Frohse. Lesions at that location could or could not have an effect on the innervation to the supinator (again, akin to the pronator teres being spared in some circumstances of pronator syndrome). Because of these limitations, the supinator is greatest averted, particularly since there are different muscular tissues (especially the brachioradialis and lengthy head of the extensor carpi radialis) that can be extra simply sampled which would possibly be beneath the spiral groove but proximal to the posterior interosseous nerve. If the lesion is at the axilla, the above muscles, as properly as the triceps and anconeus, shall be involved. A proximal lesion of the posterior wire will show additional abnormalities, including the deltoid (axillary nerve) and latissimus dorsi (thoracodorsal nerve). A C7 radiculopathy will present abnormalities of the cervical paraspinal muscle tissue and radial-innervated C7 muscles. As the radial nerve runs in close proximity to the humerus, it could commonly be injured from a fracture or as a complication of the next surgery, together with impingement by surgical hardware. One potential entrapment website is the house between the humerus and the sting of a surgical plate (red arrow). Asnotedear� E lier, several muscle tissue come off between the principle radial nerve on the spiral groove and the origin of the posterior interosseous nerve on the Arcade of Frohse, together with the lengthy head of the extensor carpi radialis and the brachioradialis. Thus, these muscle tissue are very useful in figuring out if the lesion is on the degree of the posterior interosseous nerve, or proximal to it, in the principle radial nerve in the area of the elbow. This is very essential as a result of if the needle is mistakenly positioned in the brief head of the extensor carpi radialis (also often identified as the extensor carpi radialis brevis), and found to be abnormal, the mistaken impression might come up of a lesion in the main radial nerve at or proximal to the elbow, whereas the lesion may very well be more distal, within the deep radial motor department. This is as a outcome of the short head of the extensor carpi radialis has a quantity of common anatomic variants: it could come up from the principle radial nerve within the elbow in addition to from the deep radial motor department, and barely from the proximal superficial radial nerve. One can see that if the quick head of the extensor carpi radialis on this case is provided by the deep radial motor branch somewhat than the principle radial nerve, the mistaken impression of a lesion of the primary radial nerve could probably be made. Thus, though the long head of the extensor carpi radialis can be routinely sampled, of the out there muscular tissues that can be sampled that are beneath the spiral groove but proximal to the bifurcation of the radial nerve just distal to the elbow, the brachioradialis is the best and has the fewest potential problems. Although the most common radial neuropathy occurs from exterior compression at the spiral groove, there are different inside structural lesions that may have an result on the radial nerve at varied sites along its course. In addition, fracture of the humerus and subsequent surgical open reduction and inside fixation can injure the radial nerve. Ultrasound can often answer several key questions in these circumstances: � I sthenerveincontinuity Neuromuscular ultrasound additionally performs an particularly essential position in the analysis of lesions of the deep branch of the radial nerve and the posterior interosseous nerve. To visualize the radial nerve, the patient is requested to lie supine with the elbow slightly bent and the hand pronated. The probe is placed within the short axis within the groove between the biceps and brachioradialis. At this location, the radial nerve is easily seen within the fascial airplane between the brachioradialis above and the brachialis muscle under. The nerve first runs in muscle, however as the probe approaches the mid-arm, the bony shadow of the humerus will appear. Moving more proximally and barely laterally, the radial nerve will come into contact with the surface of the humerus. The nerve then runs posterior, adjacent to the spiral groove, earlier than touring deep to the triceps within the upper arm. Once the radial nerve is adopted to the spiral groove, the probe is returned to the starting place in the groove between the brachioradialis and brachialis muscle after which moved distally. The supinator has a attribute arched shape and pattern as it surrounds the radius. If one rigorously rotates the probe 90�, the nerve can usually be seen in long axis view. However,asthenerveentersthesupinator,thereisoftena change in caliber: the nerve diameter decreases barely while its width will increase barely. Distal to the supinator, the posterior interosseous nerve runs between the deep and superficial layer of the forearm extensor muscles. Right, Same image with the radius in green, the posterior interosseous nerve in yellow, and the two heads of the supinator muscle in red. Bottom, Same image with the posterior interosseous nerve divided into a number of branches in yellow, and the 2 heads of the supinator muscle in purple. In addition to being a single round or oval fascicle, the posterior interosseous nerve may divide into two, three, or 4 fascicles aligned in a row between the two heads of the supinator. Bottom, Same picture with the posterior interosseous nerve in yellow, posterior interosseous artery in brilliant purple, superficial extensors in darkish purple, and deep extensors in mild blue. Distal to the supinator, the posterior interosseous nerve (white arrow) runs between the deep and superficial layers of the forearm extensor muscles. The nerve is commonly tough to visualize however accompanies the posterior interosseous artery, which helps locate the nerve. Back at the elbow, the superficial department can normally be followed down the forearm. As it approaches the wrist, the brachioradialis transitions from muscle to tendon. Near that time, the superficial radial nerve strikes extra superficially between the brachioradialis tendon above and the extensor carpi radialis longus beneath. Other lesions of the radial nerve within the upper arm are unusual, except there was a fracture, with or without surgical repair. As famous earlier, there are 5 potential sites of compression of the deep radial motor branch/posterior interosseous nerve, although some sites are more frequent than others.
Discount cialis super active 20 mg amex
A full examination of the pores and skin and oral mucosa could additionally be combined with a biopsy and direct immunofluorescence microscopy erectile dysfunction treatment yoga 20 mg cialis super active order free shipping. In nonscarring alopecia erectile dysfunction medications list cialis super active 20 mg purchase without prescription, spontaneous regrowth may occur, requiring no therapy in about 50% of cases. The oral treatment finasteride can stop the shrinkage of hair follicles and forestall hair loss. Complementary Therapy Advise shoppers to massage the scalp with their fingers daily. A mixture from one part rosemary oil and two Advise clients to not use harsh strategies to exfoliate the pores and skin, such as scrubbing, pumice stones, or selecting on the bumps. Prognosis With treatment prognosis is good, but if therapy is discontinued, keratosis pilaris will return. The commonest websites of these lesions are furry elements of the physique exposed to irritation, strain, friction, or moisture. Predisposing components embody diabetes mellitus, nephritis, hematologic malignancies, debilitation, and an infected wound elsewhere in the physique. Both furuncles and carbuncles are extra widespread in shoppers who live in sizzling climates. Signs and Symptoms Affected parts of pores and skin could additionally be extremely tender, painful, and swollen. The abscess may ultimately enlarge, soften, and open, discharging pus and necrotic materials. A referral to specialty retailers that fit wigs and toupees may be useful to those that are particularly sensitive about their baldness. Treatment the boil should by no means be squeezed, as a end result of doing so destroys the protecting wall that localizes the an infection. The contaminated area must be cleansed with cleaning soap and water, and sizzling, moist compresses ought to be applied. Complementary Therapy It could additionally be beneficial for purchasers to eat plenty of green, yellow, and orange vegetables. Encourage purchasers to increase fluid intake, particularly water with an added teaspoon of contemporary lemon juice. Oils from nutritional vitamins E and A, honey, and some zinc oxide may be useful as a topical utility. Tea tree oil has been used for centuries as an antiseptic, antibiotic, and antifungal agent. Etiology the lice feed on human blood and lay their eggs, or nits, in physique hair or clothing, and the eggs hatch, feed, and mature in 2 to 3 weeks. Pediculosis is extra widespread in people who live in overcrowded places with insufficient facilities. The parasite may be transmitted via contaminated clothing, hats, combs, bedsheets, and towels. There could additionally be gross excoriation of patches of pores and skin and pyoderma, an acute, pus-causing, inflammatory pores and skin illness. Treatment For scalp lice, permethrin cream rinse is rubbed into the hair for 10 minutes. A shampoo containing lindane or pyrethrin compounds with piperonyl butoxide may be used. Bedsheets, clothes, or soiled dressings that have drainage should be cleaned or disposed of properly. Complications from carbuncles could embrace bacteremia, a situation of bacteria in the blood. Prevention Prevention of furuncles and carbuncles includes good private hygiene and prevention of any infectious process. X Description Pediculosis is pores and skin infestation with lice, a parasitic insect affecting tens of millions of people annually. Complementary Therapy Substances that coat the lice, thereby trapping and suffocating them, additionally could additionally be used. After this utility, the nits and lice ought to be combed out with a small-toothed comb. Soaking the hair in an answer of equal components water and white vinegar after which wrapping the wet scalp in a towel for at least quarter-hour could assist facilitate removing. Prognosis the prognosis for pediculosis is excellent with treatment, however issues include severe pruritus, pyoderma, and dermatitis, which can be handled with antipruritics, systemic antibiotics, and topical corticosteroids. Prevention Prevention of pediculosis includes practicing good hygiene, avoiding contact with infested persons, and not sharing combs, brushes, or clothes. Etiology these lesions are brought on by impairment of the blood provide to the affected space as a outcome of persistent strain in opposition to the pores and skin floor. The condition is most regularly a consequence of extended immobilization and is commonly seen in debilitated, unconscious, or paralyzed individuals. Those with weak circulation, especially elderly persons, are at best danger for developing decubitus ulcers. Signs and Symptoms Early indicators of decubitus ulcer embrace shiny, reddened skin, usually appearing over a bony prominence (stage 1). If not treated shortly, the ulcer may turn into more serious when skin is swollen and exhibits a blister (stage 2). Diagnostic Procedures Visual examination of the lesion often is enough to establish the prognosis. Wound tradition and sensitivity testing may be carried out to isolate the causative organism if infection is suspected. Research is now being done using honey preparations, hyperbaric oxygen, and chemical substances to stimulate cell progress. Complementary Therapy Apply a paste made with vitamin E oil, zinc oxide, and goldenseal powder to the affected area. Daily baths with mild soaps containing aloe vera and exposure to adequate natural gentle may be useful. Instruct shoppers that it may be essential to pick off the nits with the fingernail, one by one. Because the situation spreads quickly, it could be very important start the remedy immediately and to inspect every member of the family every day for at least 2 weeks to verify for infestation. When she came residence from faculty yesterday, her mother seen that Karla was regularly scratching her head. When her mother requested her what was mistaken, Karla answered, "My head itches and feels crawly. It is essential to discuss with shoppers correct positioning when sitting or lying to greatest alleviate stress factors.
Cheap cialis super active 20 mg fast delivery
As it enters the forearm erectile dysfunction treatment washington dc cialis super active 20 mg on line, it runs first beneath the lacertus fibrosus erectile dysfunction supplements 20 mg cialis super active discount otc, a thick fibrous band that runs from the medial side of the biceps tendon after which over the proximal forearm flexor musculature. Just distal to the medial epicondyle, the brachial artery bifurcates into the radial and ulnar arteries. Just distal, the ulnar artery separates from the median nerve to run more medially the place it joins the ulnar nerve in the mid-forearm. Left, In the antecubital fossa, the median nerve travels adjacent to the brachial artery. As it enters the forearm, it runs first beneath the lacertus fibrosus, a thick fibrous band that runs from the medial side of the biceps tendon to the proximal forearm flexor musculature. In most people, the median nerve then runs between the 2 heads of the pronator teres. Right, Superficial head of the pronator teres sectioned to show the underlying median nerve. The pronator syndrome refers to signs that happen from compression of the median nerve at a quantity of potential websites of entrapment in the region of the antecubital fossa, together with: (1) lacertus fibrosus, (2) within the pronator teres muscle, and (3) the sublimis bridge. Rare instances of brachial artery puncture and subsequent hematoma formation have led to compartment syndromes and subsequent damage of the proximal median nerve. Injury to the median nerve within the antecubital fossa from a needle puncture, although rare, is the second most common nerve reported injured from phlebotomy. A complete excessive median neuropathy ends in a classic hand posture when the patient makes an attempt to make a grip: the affected person is unable to flex the thumb, index, and middle fingers. Rare individuals have a supracondylar bony spur from which a tendinous band (ligament of Struthers) runs to the medial epicondyle. Significantly, sensory disturbance in proximal median neuropathy is noted in the whole median territory, together with the thenar eminence, in addition to the thumb, index, middle, and lateral ring fingers. Sensory loss over the thenar eminence occurs because the palmar cutaneous branch, which innervates the thenar eminence, leaves the median nerve proximal to the carpal tunnel. The latter three entrapment websites usually are referred to collectively because the pronator syndrome. However, entrapment at any of these last three places normally produces an analogous clinical syndrome. The syndrome is characterized by ache in the volar forearm and paresthesias within the median-innervated digits, which are exacerbated by supination of the forearm and extension of the elbow. The radial pulse also may be attenuated with these maneuvers, because the brachial artery also runs with the median nerve underneath the ligament of Struthers. Pronator Syndrome Although uncommon, the pronator syndrome happens extra usually than entrapment on the ligament of Struthers. Pain may radiate proximally and infrequently is aggravated by utilizing the arm, especially with repeated pronation/supination actions. There could also be occasional paresthesias radiating into the median-innervated digits, with refined impairment of sensation in the median nerve distribution, together with the thenar eminence. The sole discovering of elevated ache with these maneuvers is especially unreliable except the pain is accompanied by median paresthesias. It carries deep sensory fibers to the wrist and interosseous membrane, nevertheless it carries no cutaneous sensory fibers. Clinically, patients current with the inability to flex the distal phalanx of the thumb, index, and center fingers, with weakness of pronation. Occasionally, the median fibers that cross over run within the anterior interosseous nerve as opposed Chapter 21 � Proximal Median Neuropathy 361 electrophysiology in true instances of proximal median entrapment often is regular or nonspecific, despite what one would possibly anticipate on theoretical grounds. Routine ulnar motor and sensory research also needs to be performed to exclude a coexistent polyneuropathy. Sensory nerve conductions of median-innervated digits ought to at all times be performed, recording probably the most symptomatic digit(s), especially if numbness or paresthesias have been observed on scientific examination. If values are borderline or simply slightly above the higher limits of regular, comparison with the contralateral aspect ought to be accomplished. If values are borderline or simply slightly above the upper limits of regular, a second median-versus-ulnar comparison study ought to be done to look for median neuropathy on the wrist. Lesions of the anterior interosseous nerve lead to weakness of the flexor pollicis longus, flexor digitorum profundus (to digits 2, 3, or both), and pronator quadratus. The thumb and index finger are unable to flex at the interphalangeal joints and the distal interphalangeal joints, respectively (arrows). For the entrapment syndromes in the region of the antecubital fossa, however, the differential prognosis is intensive as a outcome of the signs usually are imprecise. Median neuropathy at the carpal tunnel also could give rise to diagnostic confusion. Additionally, patients with cervical radiculopathy could current with radiating ache associated with paresthesias into the hand. In cervical radiculopathy, however, there often is a history of neck pain that radiates into the arm. Examination in cervical radiculopathy may reveal weak spot outside the median territory, as properly as decreased biceps, brachioradialis, or triceps reflexes. Median motor examine recording abductor pollicis brevis, stimulating wrist, antecubital fossa, and axilla 2. Ulnar motor study recording abductor digiti minimi, stimulating wrist, beneath groove, and above groove 3. Median sensory response, recording digit 2 or three, stimulating wrist (bilateral research suggested) 5. Median and ulnar palm-to-wrist blended nerve studies utilizing equivalent distances of 8 cm the next patterns suggest possible proximal median neuropathy: 1. Reduced median compound muscle action potential and/ or sensory nerve action potential amplitudes with distal latencies which are either regular or only slightly prolonged (never in the demyelinating range) and no vital slowing of the median palm-to-wrist latency in contrast with the ulnar 2. Either conduction block/temporal dispersion or marked conduction velocity slowing between the wrist and antecubital fossa, or between antecubital fossa and axilla, with normal or solely barely extended distal latencies on median motor research three. Although such findings can be anticipated on theoretical grounds, in reality they rarely happen. However, the critical a half of the research consists of careful examination of a quantity of median-innervated muscular tissues proximal to the carpal tunnel. If any of these muscles are irregular (evidence of denervation or reinnervation), the issue have to be proximal to the wrist. If any of the proximal median-innervated muscles are abnormal, other muscles innervated by the same Box 21. At least two median muscles proximal to the carpal tunnel, together with the pronator teres and one of the following: flexor pollicis longus, flexor carpi radialis, flexor digitorum sublimis If the abductor pollicis brevis is abnormal: 3. Although this will likely seem counterintuitive, remember that there are proximal lesions that spare some of the muscles distal to the lesion while affecting others. First, these syndromes are uncommon and controversial, so any further supportive data is helpful.