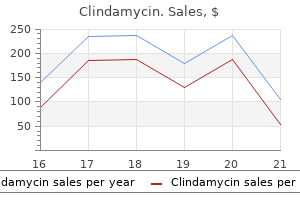
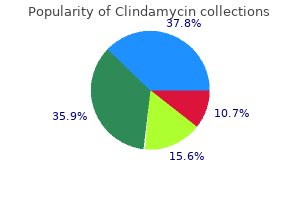
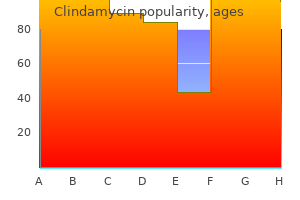
Clindamycin
Clindamycin dosages: 300 mg, 150 mg
Clindamycin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Discount clindamycin 150 mg overnight delivery
Prodromal signs corresponding to pain typically are famous by patients who sustain pathologic fractures through bone lesions antimicrobial coatings order clindamycin 150 mg online, but often the fracture is the occasion that results in bacteria binary fission clindamycin 300 mg with mastercard the diagnosis. Other benign etiologies embody fractures that occur secondary to preexisting stress fractures, fractures by way of bone weakened by osteomyelitis, and fractures round orthopaedic implants, or fractures that happen after implant removal. Primary bone malignancies, such as osteogenic sarcoma and Ewing sarcoma, and bone metastases lesions from another site of malignancy, are rare etiologies of pathologic fractures in children. For many systemic situations, the prognosis could additionally be already identified to the affected person and family, but typically a pathologic fracture is the primary sign of systemic disease. Because radiological bone adjustments could additionally be refined, the prognosis may be easily missed on radiographs. A description of all the diagnoses that are associated with pathologic fractures is beyond the scope of this chapter and is well described in other chapters throughout this e-book. If a malignancy is suspected, however, urgent biopsy of the lesion may be essential to verify the prognosis and to expeditiously information remedy. Typically, a biopsy, done on the time of fracture therapy as a frozen part, is required to affirm the analysis. Careful preoperative planning is needed to correctly execute the biopsy, ensure management of bleeding, fully excise the lesion, graft the remaining defect, and fixate the fracture. In one series of patients, closed treatment of the fracture is effective for most patients and few required later bone grafting (111). Another research reported that, in all sufferers with fractures of the decrease extremity via one of these lesions, 50% or extra of the transverse cortical diameter of the fractured bone was crammed by the lesion (110). Because of this, patients with large lesions and their families should be endorsed relating to the chance of fracture and the use prophylactic curettage and grafting to forestall it. One of the greatest fears of any orthopaedic surgeon is lacking the analysis of a malignant bone tumor. Identification of a malignant pathologic fracture is critical so that correct evaluation and treatment could be initiated expeditiously, and to present the best alternative for limb salvage. Preoperative staging and cautious biopsy planning that takes into account future reconstructive procedures that will be utilized for limb salvage are important to improve the chance for a successful consequence. Limb-sparing surgery, even after pathological fracture, is possible if adequate margins are obtained (113). In one multivariate evaluation, pathological fractures via malignancies independently predict worse survival for these patients with osteosarcoma, but not for chondrosarcoma and Ewing sarcoma (114). Spontaneous resolution of the cyst, however, is unusual, and subsequently further treatment may be needed to deal with the cyst (106) with bone grafting. A transverse cyst diameter of >85% (106) or cortical thickness <5 mm have been proposed (108) as indications for bone grafting either after pathologic fracture therapeutic or after incidental prognosis of these lesions. It is recognized in 1 in 20,000 youngsters and sometimes presents as a fracture or multiple fractures (120). The diagnosis can be troublesome to make at occasions, particularly when seen in an infant with multiple fractures, as a outcome of youngster abuse must also be considered. Some kids with milder varieties will not be diagnosed till later in life, and a history of a number of fractures over time may be the solely clue to recommend the prognosis. This weakened bone is primarily a result of disuse because of limited or full lack of ambulatory ability however can also be related to poor nutritional consumption. For kids with myelodysplasia, 41% of those with a thoracic stage of motor perform sustain fractures, whereas solely 13% of patients with lower lumbar or sacral deficits (133) accomplish that. Children with neuromuscular illnesses are at risk for pathologic fractures during regular daily actions, however the fracture risk is elevated after extended immobilization from fracture care or reconstructive surgical procedures. Fracture care ideally permits for fast mobilization, permitting early weight bearing for people who walk or can switch, or permitting switch to a chair for nonambulatory sufferers. Increased muscle tone, limb deformities from contracture, insensate pores and skin, or lack of ability to communicate about skin irritation are factors that make forged immobilization tough. Proper limb positioning, acceptable padding, and surveillance of the pores and skin by solid adjustments during the course of immobilization lessen the danger of solid issues. Frequent turning to stop skin breakdown over the sacrum and different prominences, aggressive pulmonary care to forestall pneumonia, and medical management of muscle spasms are different considerations for this group of sufferers once they require solid immobilization for fracture. While many of those fractures are effectively treated with out internal fixation, surgical stabilization could also be needed depending on the fracture type. After fracture therapeutic, bodily remedy is usually prescribed to velocity return to prefracture function. Every year, 1% to 16% of kids are bodily abused and 1 in 10 is uncared for or psychologically abused (141). Child mortality rates have been reported to be as high as 7%, however statistics are difficult to interpret because youngster abuse as a explanation for dying is believed to be underreported (143). Child abuse and maltreatment can have a devastating impact on the mental health of the recipient child, leading to a high incidence of drug and alcohol abuse and high-risk sexual and criminal conduct, which persist into adulthood. In the United States in 2006, it was estimated that 905,000 youngsters had been victims of maltreatment. The actual incidence of abuse and neglect is estimated to be a lot higher than the number reported to authorities. In 2006, the rate of child victimization of the age group of birth to 1 year was twice the general average. Approximately 40% of child victims had been maltreated by their moms appearing alone, one other 17. Victims abused by such nonparental perpetrators as an unmarried partner of a mother or father, authorized guardian, or foster father or mother accounted for 10% of the entire cases. Soft-tissue injuries, corresponding to bruising and skin lesions, are the commonest physical findings related to baby abuse, whereas head and belly accidents are the most typical causes of death (146). The clinician should evaluate all youngsters who sustain fractures with a high stage of suspicion for child abuse, and physicians are each ethically and legally bound to report all circumstances of suspected child abuse. Children with disabilities could additionally be at greater risk for abuse (147), but it have to be remembered that in addition they often undergo from osteopenia which can predispose them to pathologic fractures. Differentiating abuse fractures from fractures that occur accidentally due to pathologic bone, similar to these seen in kids with osteogenesis imperfect, may be very troublesome. The doctor should always be aware that any baby, no matter age, socioeconomic status, bodily or intellectual disabilities, or previous history, could also be a victim of child abuse. Some particular fracture patterns must be straightforward to recognize as being inflicted by abusive trauma. The discovering of multiple rib fractures in children three years or youthful had a positive predictive value of 100% when kids with an outlined historical past of accident or disease have been excluded (149). Half the abused sufferers in one study (150) had a single fracture, and the commonest fracture type was a transverse fracture. Age is amongst the most important components in differentiating unintended from abusive trauma (151, 152). For instance, single diaphyseal spiral fractures of the tibia or femur are common unintended injuries in toddlers, however are suspicious if the kid is preambulatory (151). In one study, the overall proportion of abuse was 11% in youngsters beneath three years with an isolated femur fracture which increased to 17% in kids younger than 1 12 months. There is a few debate as to which fracture patterns are commonest in child abuse and Skeletal Surveys. This fracture could presumably be in keeping with unintended harm if there have been a documented historical past of great trauma (a fall or auto accident).
Syndromes
- Guillain Barre syndrome or other diseases that inflame nerves
- Breathing problems
- Low blood pressure
- Ulcerative colitis
- Blood thinners may be used to prevent blood clots.
- Do you feel anxious or stressed, especially before you start breathing rapidly?
- Upper GI
- MRI of the head
Cheap clindamycin 300 mg without a prescription
Vascular etiology of limb defects: the subclavian artery supply disruption sequence bacteria that causes strep throat trusted clindamycin 150 mg. Coping when a baby has a incapacity: exploring the impression of parent-to parent support antibiotic 24 hours not contagious generic 150 mg clindamycin. Physical attractiveness as a correlate of peer standing and social competence in preschool children. Effects of stress, social support, and self-esteem on depression in kids with limb deficiencies. Correlates of perceived physical appearance in kids with congenital/acquired limb deficiencies. The morphology, pure history, and treatment of proximal femoral focal deficiency. Congenital short femur: clinical, genetic and epidemiological comparison of the naturally occurring condition with that brought on by thalidomide. Congenital longitudinal deficiency of the fibula: follow-up of therapy by Syme amputation. Amputation in children: a follow-up of 74 children whose lower extremities have been amputated. The autologous stump plasty: remedy for bony overgrowth in the juvenile amputees. Tumors of the top of the fibula: good function after resection with out ligament reconstruction in 6 patients. Outcomes of lengthening short lower-extremity amputation stumps with planar fixators. A randomised double blind trial of the effect of pre-emptive epidural ketamine on persistent ache after lower limb amputation. The impact of intra-neural local anaesthetic infusion on ache following major lower limb amputation. Gabapentin in phantom limb ache administration in kids and young adults: report of seven circumstances. Congenital abnormalities of the femur and related decrease extremity malformations: classification and therapy. Congenital ball-and-socket ankle joints and related lower-extremity malformations. Syme amputation; an analysis of the physical and psychological operate in younger patients. Amputation and prosthesis as definitive therapy in congenital absence of the fibular. Congenital absence of the fibula: treatment by Syme amputation - indications and technique. The pure historical past and management of congenital brief tibia with dysplasia or absence of the fibula. The Ilizarov methodology for correction of advanced deformities: psychological and useful outcomes. Fibular hemimelia; comparability of consequence measurements after amputation and lengthening. Malleolus externus plasty for joint reconstruction in fibular aplasia: preliminary report of a new approach. Congenital deficiency of the tibia: a report on 22 circumstances J Pediatr Orthop B 1998;7:298. Congenital absence of the tibia: transplantation of head of fibula: arthrodesis at the ankle joint. Construction of a knee joint in congenital total absence of the tibia (paraxial hemimelia tibia). Failure of centralization of the fibula for congenital longitudinal deficiency of the tibia. Congenital diastasis of the inferior tibiofibular joint: a evaluate of the literature and report of two circumstances. Wedge-shaped distal tibial epiphysis within the pathogenesis of equinovalgus deformity of the foot and ankle in tibial lengthening for fibular hemimelia. Natural historical past and treatment of instability of the hip in proximal femoral focal deficiency. Growth patterns after lengthening of congenitally short lower limbs in younger children. Complex congenital anomalies of the lower extremities: femoral bifurcation, tibial hemimelia, and diastasis of the ankle. Treatment of longitudinal deficiency affecting the femur: comparing affected person mobility and satisfaction outcomes of Syme amputation against extension prosthesis. Rotation-plasty for congenital defects of the femur: making use of the ankle of the shortened limb to management the knee joint of a prosthesis. Van Nes rotational osteotomy for treatment of proximal femoral focal deficiency and congenital brief femur. Quality of life in survivors with a van Ness-Borggreve rotationplasty after bone tumour resection. Malignant tumor of the distal part of the femur of the proximal part of the tibia: endoprosthetic replacement of rotationplasty. Morphologic characteristics of acetabular dysplasia in proximal femoral focal deficiency. Early conservative and operative therapy to achieve early regular progress in proximal femoral focal deficiency. Resection, rotationplasty, and femoropelvic arthrodesis in severe congenital femoral deficiency. Impact of prostheses on perform and quality of life for kids with unilateral congenital belowthe-elbow deficiency. Prosthetic gadgets for youngsters with bilateral higher limb deficiencies: when and if, pros and cons. A long-term evaluation of children with congenital and acquired higher limb deficiency. The Krukenberg procedure: a surgical option for the remedy of double hand amputees in Sierra Leone. The worth of the Krukenberg operation and its indication regardless of fashionable prosthesis of the hand. Lengthening of congenital below-elbow amputation stumps by the Ilizarov technique. Does socket configuration affect the position of the femur in above-knee amputation? The influence of four-bar linkage knees on prosthetic swing-phase flooring clearance. Gait evaluation and vitality price of beneath knee amputees carrying six completely different prosthetic ft. Comparison of vitality value and gait efficiency during ambulation in below-knee amputees utilizing totally different prosthetic feet - a preliminary report. It is estimated that roughly 30 million kids and youth between the ages of 6 and 21 years have interaction in sports activities programs that are held outside of college, and 7.
Clindamycin 150 mg order on line
Surgical therapy with typical transphyseal tunnels has been described (180 antimicrobial treatment buy cheap clindamycin 300 mg, 181) antibiotics root canal clindamycin 150 mg cheap visa. Eight Tanner stage 1 and nine Tanner stage 2 patients have been adopted for a mean of forty four months. Surgical Technique Anterior Cruciate Ligament Reconstruction with the Iliotibial Band. For prepubescent children, Tanner 1 or 2, a physeal-sparing reconstruction is beneficial (179). The operative extremity is prepped and draped from the extent of the foot to the extent of a tourniquet positioned at the thigh. C: A full-length clamp is placed into the over-the-top position arthroscopically and pushed through the posterior capsule. E: the graft is pulled under the intermeniscal ligament and delivered into the distal incision. The clamp is then spread according to the fibers of the tendon to start the posterior break up within the tendon. A meniscotome is used to extend the 2 parallel incisions proximally in line with the fibers of the tendon. The incisions ought to be continued as proximally as possible to maximize graft length. The tendon is separated from the underlying joint capsule and lateral femoral condyle. The capsule on this area is skinny, however an effort ought to be made to maintain the integrity of the capsule to forestall fluid extravasation during later arthroscopy. The graft is left attached to Gerdy tubercle distally and tucked beneath the pores and skin for the arthroscopic portion of the case. A restricted notchplasty is carried out to assist in visualization and identification of the over-the-top position on the distal femur. Excessive dissection ought to be averted to stop damage to the perichondral ring of the distal femoral physis during notchplasty. A full-length clamp is positioned via the anteromedial portal and into the over-the-top position. An additional 3-cm incision is made on the anteromedial facet of the proximal tibial. The incision have to be distal to the tibial physis and medial to the tibial tubercle apophysis. Under arthroscopic visualization, a rasp is then handed alongside the periosteum and into the knee joint proximally. Using the rasp, a groove is then made in the tibial epiphysis to facilitate graft passage under the ligament and to translate the graft posteriorly so as to obtain a extra anatomic position of the graft. With the knee in ninety degrees of flexion, rigidity is utilized to the graft, and the proximal facet of the graft is sutured to the periosteum of lateral femoral condyle. This varieties the extra-articular part of the reconstruction and helps to restrict rotation of the tibia. Periosteal flaps are raised medially and laterally so as to accommodate the diameter of the graft. Care is taken to avoid extreme dissection laterally as this risks damage to the tibial tubercle apophysis. With the knee in 20 to 30 degrees of flexion, distal tension is utilized to the graft. Flexion is progressively increased to 90 degrees from weeks 2 to 6, after which movement is unrestricted. Touchdown weight bearing in full extension is recommended for 6 weeks postoperatively. Jogging is instituted at three months with return to slicing sports activities at 6 months pending clearance. Clinical follow-up with evaluation for leg-length discrepancy or angular deformity is done yearly for no much less than 2 years. These sufferers are usually Tanner stage three with pigmented axilla and pubic hair for boys. For males, the bone age is from 14 years till skeletal maturity and for females 13 years until skeletal maturity. Adolescents nearing skeletal maturity (Tanner 5) can be treated as adults with conventional tunnels and bone plugs if desired. It can be useful to palpate the insertion of the hamstrings previous to prepping and draping the affected person. Typically, the superior border of the medial hamstrings is 3 cm under the joint line. A vertical incision is made, and dissection is carried right down to the Sartorius fascia. Blunt dissection is used to separate the Sartorius fascia from the subcutaneous tissue. The gracilis and semitendinosus must be palpated just below the Sartorius fascia. A right-angled clamp or Metzenbaum scissors are used to outline the superior and inferior borders of the hamstrings tendons. A clamp could also be handed deep to the tendons in order to apply distal traction on the tendons which will assist free the tendons from the Sartorius fascia. The gracilis tendon is then dissected distally and launched from its insertion on the tibia. Care must be taken to maintain a pick-up or clamp on the tendon to stop proximal retraction after release. Distal traction is again utilized to the tendons individually and any adhesions are launched. Special attention ought to be paid to adhesions from the semitendinosus to the medial head of the gastrocnemius. Modified Transphyseal Anterior Cruciate Ligament Reconstruction with Hamstrings Autograft. The leading sutures of the endobutton are handed by way of the tibial and femoral tunnels. Excess muscle is faraway from the proximal ends of the tendons and whipstitches are placed. The tendons are then folded over a closed-loop Endobutton to kind a quadrupled graft, positioned beneath tension, and lined with a moist sponge. A diagnostic arthroscopy is performed using normal anteromedial and anterolateral portals.
Effective clindamycin 300 mg
Bracing for decrease extremity stress fractures could embody boot or solid immobilization or off-the-counter orthotics for four to 6 weeks to enable adequate bone deposition to happen infection specialist discount 300 mg clindamycin otc. Continued rehabilitation and prevention contains advancement to strengthening infection vaginal discharge clindamycin 300 mg order, flexibility workouts and coaching, as properly as instruction regarding already addressed elements in the workup together with dietary influences, graduated training regimen will increase, and an awareness of coaching surfaces. There are some anatomical areas which are susceptible to extended symptoms or in some circumstances nonunion including the femoral neck, tibial diaphysis, medial malleolus, and tarsal navicular (366). Femoral shaft stress fractures are at low danger of nonunion or displacement and may be managed with activity modification. Surgical remedy is subsequently beneficial and is mostly performed with cannulated compression screws. For tibial stress fractures, the posterior medial compression facet stress fracture is the most common. This is a low-risk stress fracture and most heal with four to 6 weeks of pneumatic boot immobilization. The tibial anterior rigidity side fracture is much less widespread; however in this hypovascular area, callus is generally not formed and patients are at risk for delayed union or nonunion (378). In the case of delayed union, a patellar tendon-bearing cast or industrial orthosis ought to be employed for four to 6 months before surgical procedure is considered. If nonunion exists within the skeletally mature adolescent, options to deal with the nonunion include the use of an intramedullary nail with or with out bone grafting and fibular osteotomy (379). In the skeletally immature individual with a diaphyseal tibial stress fracture that fails to heal after 6 months of nonoperative therapy, operative treatment is indicated. Excision of the fibrous nonunion and autogenous bone grafting from the iliac crest with attainable fibular osteotomy has been employed successfully on this uncommon situation (379). For medial malleolus stress fractures, the fracture line tends to traverse in an oblique method from the intersection of the medial malleolus and the tibial plafond. Nonoperative administration together with restricted weight bearing as well as casting or bracing has a better failure fee than other low-risk fractures. Operative intervention therefore may be performed to facilitate early healing and restoration. In the case of nonunion of tarsal navicular stress fractures, really helpful remedy includes excision of the nonunion website and autogenous bone grafting. In the case of fifth metatarsal fracture nonunion, recommended therapy includes intramedullary screw fixation with or without bone grafting. While the best concern for a young athlete is the timeliness of return to sports, the treating physician must assess multiple variables. Return to play ought to be guided by factors indicative of healing and harm prevention including the cessation of ache, radiographic proof of a healed fracture, elimination of inciting causes and instruction relating to coaching strategies, and a graduated exercise program. Sever calcaneal apophysitis is a self-limited inflammatory situation of the os calcis in rising youngsters. The typical baby with Sever disease is from 9 to 14 years of age and concerned in working sports (380). The condition is bilateral generally and presents as diffuse ache and tenderness over the prominence of the heel somewhat than completely on the plantar aspect as is seen in plantar fasciitis (381). With relaxation, exercise modification, and passage of time, the situation all the time resolves (380, 382, 383). Cast immobilization may rarely be needed for the affected person with severe, incapacitating signs (383). Repetitive stress in the upper extremity could result in a specific stress reaction within the physis. Radiographically, the stress reaction is noted as a radiolucency and irregularity on the metaphyseal aspect of the physis, just like the radiolucency seen within the medial side of the proximal tibia in adolescent tibia vara and in the femoral neck in patients with slipped capital femoral epiphysis. The same research discovered an elevated incidence of optimistic ulnar variance in the wrists of nonelite gymnasts (384). The speculation of the examine was that repetitive compressive forces to the distal radius led to untimely progress arrest resulting in a constructive ulnar variance. Positive ulnar variance has been associated with secondary wrist issues including tears of the triangular fibrocartilage complicated and ulnar impingement syndrome. Anteroposterior radiograph of wrist of gymnast with 3-month historical past of wrist pain. Note radiolucency on the metaphyseal facet of progress plate (physis) indicative of stress physeal reaction. Treatment of those overuse stress reactions is centered on the discontinuation of the offending force or modification of actions till the signs of pain subside. Baseball pitchers could must chorus from pitching for 2 to 3 months till the pain that accompanies the throwing motion completely subsides. Gymnasts with symptomatic radial physeal stress response ought to chorus from loading their wrists for as much as 2 to three months to allow the reactive adjustments to heal. Strengthening exercises to specifically strengthen the wrist flexors should be undertaken in gymnasts, and taping or bracing to restrict wrist dorsiflexion may assist prevent recurrence. Radiographs of the proximal humerus in a 14-year-old, right-handed baseball pitcher with shoulder pain that progressed over the final few weeks of the season. A: Widening and irregularity of the physeal plate are current in the best shoulder. The elbow of the immature athlete is vulnerable to damage when the athlete throws too regularly or makes use of a method that puts too much stress on the elbow joint. While young athletes have excellent healing potential and regenerative capacities, the apophyses and physes are areas of weak spot in young throwers. In a youth baseball research of 476 pitchers, 50% of 9- to 14-year-olds reported elbow or shoulder pain (386). During the throwing movement, a big valgus moment is applied to the elbow joint (385). Recent literature has emphasized the necessity for correct pitching mechanics in order to cut back damage risk (388, 389). Better pitching mechanics have been proven to improve efficiency as nicely as create lower valgus load on the elbow and rotational torque on the humerus (388). They really helpful for 9- to 10-year-old pitchers limits of 50 pitches per sport and 75 pitches per week. Pitchers are additionally discouraged from pitching for multiple group in a given season and from returning to the mound in a sport as quickly as he or she has been eliminated (393). Youth pitchers are additionally at elevated risk of elbow and shoulder damage once they throw curveballs and sliders, and youth pitchers ought to therefore avoid throwing breaking pitches (386). The authors suggest that increased threat of harm is due to the amount of pitching quite than the type of the pitch (394). Risk components that cause elbow problems within the younger athlete involved in throwing sports have been studied extensively in current years.
Clindamycin 150 mg line
The mechanism of damage is usually a fall on the shoulder or extreme lateral compression of the shoulder girdle virus outbreak 2014 buy discount clindamycin 150 mg online. The subclavian vessels topical antibiotics for acne uk clindamycin 150 mg buy overnight delivery, brachial plexus, and apex of the lung lie beneath the clavicle but are hardly ever injured on the time of fracture. A figure-eight harness and/or a sling may be used till the patient is ready to transfer the arm comfortably. Uneventful, rapid therapeutic is the rule, though displaced fractures may heal with a visible subcutaneous prominence. Parents should be advised that, no matter alignment, healing will produce a bump that will transform over the course of a number of months to years. Indications for surgical procedure are rare but embody open fractures, severe displacement with the bone finish impaled through the trapezius, and irreducible tenting of the pores and skin by the bone fragments. Recently, adults with clavicle fractures which are severely displaced and/or shortened have been found to have dissatisfaction and decreased function after nonoperative therapy (2), leading to recommendations for operative treatment of fractures with >100% displacement or shortening >2 cm. The treatment of clavicle fractures in adolescents approaching skeletal maturity is evolving, with some recommending surgical therapy for widely displaced or shortened fractures. Some practitioners favor operative treatment in teenage athletes to facilitate rehabilitation and maybe earlier return to sport, particularly in circumstances where the clavicle fracture is on the dominant facet of a throwing athlete. Two current papers have noted that kids and adolescents may be handled efficiently with plate fixation with very low complication charges (3, 4). In adolescent patients, a "wait-and-see" method recognized four patients with displaced clavicle fractures who developed symptomatic malunions. Nonunion after clavicle fracture has been reported in adolescents, however it responds to bone grafting and plating (5). Posterior or retrosternal displacement of the medial clavicle can cause damage to or compress the nice vessels, trachea, or esophagus, and thus discount is indicated. Because of the potential for hemorrhage, it is recommended that reduction be tried within the working room beneath common anesthesia with consciousness by a thoracic or a vascular surgeon. Some recommend that a thoracic surgeon be scrubbed in at the time of reduction (8), especially for circumstances with delayed treatment (>1 week) as the medial end of the clavicle could also be adherent to adjoining vascular buildings. Fractures with anterior or superior displacement are often managed nonoperatively. Closed discount is tried in acute injuries by longitudinal traction, abduction, and shoulder extension of the involved arm and is often profitable. In posteriorly displaced dislocations, the discount can be unstable because of the posteriorly directed Medial Clavicle Fracture and Sternoclavicular Separation. Therefore, displacements of the medial end of the clavicle are often physeal separations that mimic sternoclavicular dislocation (7). Posterior displacement by fracture or dislocation may cause dysphagia or respiratory compromise. Physical examination and plain radiography are unreliable in assessing displacement. These injuries are incessantly missed, and a high index of suspicion for sternoclavicular injury is required in patients with pain and tenderness in the area. Posteriorly displaced medial clavicle fractures or sternoclavicular dislocations are usually handled operatively to relieve compression of mediastinal buildings. If the surgeon believes a steady discount is achieved, postoperative axial imaging must be obtained to doc upkeep of discount. If the reduction is unstable, or with late presentation, open discount and fixation is performed. The surgical preparation extends from the midneck to stomach, and across the chest to include the contralateral acromioclavicular joint. Having a thoracic or vascular surgeon on standby and emergency thoracotomy devices available is really helpful (8, 9, 19) the ipsilateral higher extremity can be prepped into the surgical field if desired to permit traction through the arm and stability testing with vary of motion of the shoulder after fixation. The medial clavicle is approached via a transverse incision extending from the middle thirdέedial third junction of the clavicle to just previous the midpoint of the sternal notch. Subcutaneous dissection is carried out through the platysma to the level of the periosteum, after which the periosteum is incised from lateral to medial instantly anterior over the clavicle. As the dissection proceeds medially, the periosteum will remain intact and attached to the medial clavicular epiphysis in physeal accidents and must be preserved. In dislocations, the periosteum will often be hooked up anteriorly to the fibrocartilaginous disc of the sternoclavicular joint. Instead, cautious subperiosteal circumferential dissection around the clavicle close to the middle thirdέedial third junction may be carried out, and a clamp can then be placed around the clavicle extra laterally. This will help in stabilizing the clavicle for careful subperiosteal dissection with an elevator working from lateral to medial. During discount of dislocations, it is important to notice that solely about the inferior one-third to one-half of the medial clavicle articulates with the sternal notch. Intraoperative photograph (with head to left) of blunt-tip clamp round medial proper clavicle. The metaphysis is displaced posteriorly and cephalad from the epiphysis, which is seen between the 2 Senn rake retractors. Suture fixation, wire fixation, and tendon weave via bone tunnels have all been recommended. For physeal accidents, suture or sternal wire fixation from the metaphysis to the epiphysis (medial clavicular head) is enough. For dislocations, drill holes by way of sternum are used with figure-of-eight heavy suture to the anterior medial clavicle. After repair, the adequacy of discount and stability are assessed under direct visualization. The stability is examined by direct posterior pressure (and range of motion of the ipsilateral shoulder if desired). The periosteum is commonly thick and is then closed over the clavicle to increase the fixation. The patient is placed in a sling for four weeks, and for 6 weeks the affected person avoids crossarm adduction and heavy lifting with the involved extremity. The mechanism of harm to the distal clavicle is similar to adult acromioclavicular separation. This is as a end result of the distal epiphysis of the clavicle remains a cartilaginous cap until the age of 20 years or older (6), whereas the acromioclavicular and coracoclavicular ligaments are firmly connected to the thick periosteum of the clavicle. Because these accidents characterize physeal disruption with herniation of bone from the periosteal tube, tremendous potential for therapeutic and transforming exists. Lifting the clamp on medial clavicle anteriorly reduces the metaphysis to the epiphysis (beneath Senn rake retractor) prior to figure-of-eight suture fixation. A sling or shoulder immobilizer is used for 3 weeks, adopted by a graduated exercise program. Even in competitive athletes, shoulder strength and vary of motion are sometimes not impaired after rehabilitation (17ͱ9). The occasional affected person who develops late symptoms of ache and stiffness could also be relieved by resection of the distal clavicle (18), with ligament reconstruction. In grade V separations, the clavicle is displaced 100 percent to 300% superiorly, and the clavicle lies subcutaneously.
Groundnuts (Peanut Oil). Clindamycin.
- Dosing considerations for Peanut Oil.
- Are there safety concerns?
- How does Peanut Oil work?
- What is Peanut Oil?
- Lowering cholesterol, preventing heart disease, decreasing appetite for weight loss, preventing cancer, arthritis and joint pain, scalp crusting and scaling, dry skin and other skin problems, constipation, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96490
Discount 300 mg clindamycin amex
The snapping and pain at this stage often occur with every day activities but antibiotic 1174 clindamycin 300 mg generic without a prescription, sometimes antibiotic resistance and superbugs clindamycin 300 mg purchase otc, are current only during physical exertion. Over the final 50 years, numerous surgical methods have developed for the treatment of refractory instances of the iliopsoas snapping tendon. Two of the patients had an exostosis faraway from the anteromedial facet of the lesser trochanter; these exostoses had been believed to have been contributing to the symptomatic snapping. The authors famous that their skin incision modified from an anterior vertical incision to a extra cosmetically interesting incision working just distal to the inguinal crease in the final 14 patients. In all the sufferers, the tendon was partially divided below the pelvic brim near its insertion onto the lesser trochanter. Of the 20 sufferers within the sequence, 6 (30%) had recurrent snapping, 3 (15%) reported weakness in hip flexion, and a couple of (10%) required reoperation. They described a medial approach by way of a horizontal incision a quantity of centimeters below the inguinal skin crease. As with previously reported approaches, the tendon lengthening was carried out below the pelvic brim, near the insertion of the tendon on the lesser trochanter. No sufferers skilled continued snapping postoperatively, but two sufferers reported continued hip pain. In the only research to tackle inner snapping hip within the adolescent population, Dobbs et al. All the hips have been handled with a fractional iliopsoas tendon lengthening above the pelvic brim by way of a modified iliofemoral method. This approach permits wonderful visualization of the iliopsoas musculotendinous junction and facilitates complete transection of all tendon fibers at this level. Two sufferers had a transient lower in sensation that was localized to the anterolateral aspect of the thigh. For patients with continued pain and popping that limits activities, a fractional iliopsoas tendon lengthening via a modified iliofemoral strategy is beneficial (76). This strategy has been effective in relieving signs and permitting sufferers to return to their preoperative stage of functioning while preserving hip-flexion energy. Both the anterior and medial approaches to the hip permit the surgeon to partially divide the iliopsoas tendon just above its insertion on the lesser trochanter. The benefits of those two approaches embody good visualization of the tendon insertion and direct entry to any contributing exostoses on the lesser trochanter and femoral head. The main drawback with these two surgical approaches that try and lengthen the tendon under the pelvic brim lies in judging the amount of tendon to launch. Insufficient lengthening ends in recurrent snapping, whereas overlengthening leads to hipflexion weak spot (69, seventy one, 83). Other issues embody the potential for a cosmetically unappealing scar resulting from an anterior vertical incision (69) and the frequent periincisional loss of sensation with the medial strategy by way of a horizontal incision beneath the inguinal crease (83). Approaches that lengthen the tendon above the pelvic brim have higher reported maintenance of hip-flexion strength and less recurrence of snapping than people who lengthen the tendon under the pelvic brim (76, 78). A drawback of the ilioinguinal strategy for this condition is the relative unfamiliarity of this method to many pediatric orthopaedic surgeons. The modified iliofemoral approach (76), then again, is used regularly by pediatric orthopaedists in performing pelvic osteotomies. Extreme care must be taken to accurately identify the tendon earlier than transection as a outcome of the femoral nerve lies close by. The nerve must be identified on the sartorius facet of the sartoriusδensor muscle interval and retracted medially. Transient synovitis of the hip is the most typical source of ache within the young baby. It is characterized by an acute onset of hip pain related to a limp in a baby that has no other musculoskeletal or constitutional signs. This scientific problem has been typically referred to as irritable hip, remark hip, poisonous synovitis, transitory coxitis, coxitis serosa, coxalgia fugax, and phantom hip. Treatment is necessary only for sufferers with a painful and symptomatic iliopsoas snapping hip. A supervised bodily remedy program emphasizing iliopsoas stretching for a minimal of three months Etiopathogenesis. Affected children vary in age from three to 12 years, with the typical affected person being between 5 and 6 years of age. They also reported a seasonal variation, with extra circumstances within the fall than within the winter. Ninety-five percent of the instances are unilateral and proper and left hips are affected equally. After a child has had an episode of transient synovitis of the hip, the annual risk of recurrence for that baby is 4% (84, 86). Lovett and Morse (87) first described this situation as a short-lived and ephemeral form of hip illness, and differentiated it from tuberculosis. Some authors have proposed trauma as a explanation for transient synovitis, with local trauma to the concerned hip being current in up to 30% of the instances (881). However, as with most childhood musculoskeletal conditions, a major variety of sufferers could relate an episode of trauma to the onset of signs, however this is in all probability not the precise explanation for this condition. Because a excessive share of the children with transient synovitis present with a latest historical past of an upper respiratory tract infection, a viral etiology has been suggested. Viral serology in 67 sufferers confirmed raised antibody titers to viruses including rubella, enterovirus, and Epstein-Barr. Other investigators have evaluated different viruses together with parvovirus B-19 and herpes virus-6 and were unable to affirm any correlation between transient synovitis and an infection with these specific viruses (946). Upper respiratory bacterial infections, pharyngitis, otitis media, and gastrointestinal issues have additionally been related to transient synovitis of the hip in as a lot as 70% of the patients. Spock (97) reported a better incidence of nostril and throat b-hemolytic streptococci in patients with transient synovitis when in comparison with asymptomatic sufferers. Allergic predisposition has additionally been related to transient synovitis of the hip in as much as 25% of patients. In 1952, Edwards reported that sufferers with transient synovitis recovered in a couple of days with the usage of antihistamines, and Rothschild et al. Finally, some investigators have instructed that progress abnormalities are associated with transient synovitis of the hip. Spock (97) found a 3 times higher incidence of transient synovitis in obese, stocky kids in contrast with a randomly selected, age-matched control group. The traditional medical presentation is a reasonably rapid onset of limping, unilateral hip pain, and subsequent refusal to bear weight on the involved extremity in an otherwise wholesome child. The pain is normally situated in the groin and hip space, with referred ache to the anteromedial aspect of the thigh and knee. The ache is acute in about half of the sufferers, with symptoms being present for 1 to three days before presentation. In other patients, the signs could also be extra chronic, with symptoms being present for several weeks. The pain is usually delicate, but in some youngsters, it can be extreme sufficient to awaken them at night time.
Buy cheap clindamycin 150 mg on line
Appropriate instruction virus removal tools clindamycin 300 mg buy free shipping, supervision antibiotics qt prolongation clindamycin 150 mg purchase, and protecting equipment, including helmets, wrist guards, and elbow and knee pads, should be mandated (18). Trampoline-related injuries have gotten rather more common and, like skateboard accidents, are regularly high-energy accidents. These accidents typically happen within the home setting usually underneath the supervision and with the knowledge of the dad and mom, most of whom know of the potential dangers of trampoline use (21, 22). Jumping with a couple of person on the trampoline increases the chance of harm considerably. It is unclear if trampolines at house or on playgrounds can ever be used safely, and some advise that trampolines be Motor Vehicle Accidents. Motor automobile accidents are the most typical cause of demise for kids and adolescents in the United States. Child safety seats can reduce fatal injuries by 71% for infants youthful than 1 year old and scale back deadly injuries by 54% for toddlers 1 to four years old. The character of accidents in restrained youngsters is different in comparability with those unrestrained, with fewer fractures occurring however with higher proportion of femur, spinal, and pelvic injuries. Appropriate use of child security automobile seats, mixed with sitting the child in the rear seat (center place ideally) and by no means in the entrance seat with an airbag, is critical for the prevention of injury in a motorcar accident. All dad and mom should be made conscious of the protection pointers for youngster restraints in motor automobiles established by the American Academy of Pediatrics, not only to minimize the risk of injuries in motorcar crashes, but additionally to facilitate adherence to state and federal guidelines for protected transportation of children. Like grownup bone, the diaphysis of lengthy bones is comprised of dense cortical bone and the metaphysis is comprised of spongy, cancellous bone. There are 4 distinct areas which are associated with development and reworking processes. The epiphysis is the location of secondary bone ossification that determines the dimensions and form of the articular surface. The epiphysis is also the resting site of osteoprogenitor cells, or chondrocytes, that develop into the components of the physis. Ligaments take their origin from or insert into the epiphyses at many joints, such as at the knee or ankle. Physeal development and the appearance of the secondary ossification centers happen in a predictable manner because the youngster matures. The physis, or development plate, is a narrow band of cartilage that lies between the epiphysis at the finish of the bone and the metaphysis. The physis or growth plate is the most important feature that differentiates bones of children from that of an adult. Longitudinal bone progress happens primarily through the substitute of a cartilage anlage by a process termed endochondral ossification. The physis is very organized at the mobile degree into columns that span the epiphyseal end and the metaphysis. The germinal zone is closest to the articular floor and incorporates the resting chondrocytes, the precursors of recent bone. Guided by local and systemic development factors, these cells divide, forming the proliferating zone (27). In the hypertrophic zone, adjoining to these cells, the chondrocytes enlarge and mature. As these cells begin to degenerate, vascular budding from the adjacent metaphysis triggers the dystrophic calcification of the matrix producing the so-called zone of provisional calcification. As the metaphyseal vessels migrate into this dead cartilage and its degenerated matrix, they carry in either chondroclasts or osteoclasts that reabsorb the lifeless cartilage cells and exchange them with osteoclasts to produce osteocytes and a very ossified tissue. With additional vascular ingrowth, this zone remodels quickly and turns into mature metaphyseal (lamellar) bone to kind the diaphysis. Extracapsular physes are extra richly vascularized by vessels that penetrate directly into the periosteum and the capsular attachments that encompass them. Because of this, intracapsular epiphyses are more susceptible to vascular disruption from physeal fractures or osteoarticular infections. Serious development disturbances, manifesting as articular floor deformity, angular deformation, or limb-length inequalities, may happen in younger children from these etiologies. It have to be additionally remembered that underlying the articular cartilage is a small area of endochondral ossification that contributes to the growth of the cartilage of the articular floor. Any injury to this space of endochondral ossification can lead to the event of a defect within the articular floor. Another unique characteristic of growing bone is its thick, vascular, and highly osteogenic periosteum. With the exception of those websites, fracture displacement in children causes muscles and ligaments to separate from the outer fibrous layer of periosteum, forsaking the inner osteogenic layer. The partially intact periosteal sleeve limits fracture displacement to a point and may be exploited by the surgeon to achieve and preserve fracture discount. Periosteum, nevertheless, may also inhibit fracture reduction if a torn finish turns into interposed between the fragments or if the bone ends button-hole by way of a longitudinal tear within the periosteum. Failure of closed reduction is usually the result of entrapment of the bone end outdoors the periosteal gap when reduction with longitudinal traction is tried. Fractures to the immature skeleton, like in the grownup, are described by location and fracture pattern. Many of those fracture patterns are similar to grownup fractures, but others are unique to the growing baby. Because of its lower density, growing bone has a lower modulus of elasticity, diminishing its power and response to bending forces but allowing it to absorb larger energy earlier than failure. This mechanical property explains the incidence of a few of the fracture types unique to kids. While youngsters maintain full fractures like adults, incomplete fracture sorts are extra frequent in children compared to adults. As the kid matures, fracture patterns sustained extra carefully resemble those of an adult. This is composed of mature cortical bone which, in youngsters, has remodeling potential. Intracapsular epiphyses, such because the proximal femur and proximal radius among others, receive blood through vessels that enter round Incomplete Fractures. Incomplete fractures include stress fractures and insufficiency fractures in adults. If the limit of plastic deformation is exceeded, gross failure of a portion of the osseous construction happens. Because of a selection of elements, including the elevated flexibility of the osseous construction and the dissipation of a nice deal of the force with the initial elastic and plastic deformation, there is probably not enough residual pressure to complete the failure of the complete osseous construction (30). The metaphysis of long bones is composed largely of cancellous bone surrounded by a thin layer of cortical bone. If a longitudinal force is utilized along the axis of the extremity, this skinny cortex will fail in compression producing the everyday bulging of the "torus" or "buckle.
Clindamycin 300 mg
In the young child antibiotic resistance experiment 150 mg clindamycin purchase with amex, acetabular deficiencies are generally assessed by arthrography and by inspection on the time of open discount virus 68 cheap clindamycin 300 mg overnight delivery. In most instances, an arthrogram at the time of surgery shows glorious protection of the femoral head by the unossified acetabular cartilage. Given enough time, a few of this acetabu- lar cartilage might resume normal ossification and proper a considerable quantity of the dysplasia. Any osteotomy of the iliac bone and the neovascularity stimulated by it in therapeutic may improve the ossification of the in any other case unossified acetabular cartilage. In any case, the redirection of the acetabulum restores more regular bony anatomy and regular biomechanics that will even be components in stimulating ossification (260). Shelf procedures had been described earlier than 1900 and were used extensively until the mid-1950s, when Chiari described his medial displacement osteotomy (414). Later, Salter, Pemberton, and others described various pelvic osteotomies for redirecting the acetabulum and covering the femoral head with articular cartilage. There are two oval holes on the facet plate, which within the smaller two plates accommodate the 3. It is best to carry out this operation on a regular, flat radiolucent working desk. After the intertrochanteric area of the femur is uncovered, the leg is manipulated to place the femoral head and neck within the desired place. A Steinmann pin heavy enough to management the proximal fragment is then drilled into the proximal fragment. This pin ought to start just below the epiphysis of the greater trochanter and be parallel to the floor and perpendicular to the median aircraft of the physique (A, B). When this pin is returned to this place after the osteotomy, the femoral head is returned to the desired relationship with the acetabulum. The osteotomy reduce is then made parallel to this pin and just above the lesser trochanter. In children youthful than 3 to four years of age, a single osteotomy minimize perpendicular to the femoral shaft and just proximal to the lesser trochanter can be made. As the proximal fragment is tipped again into the specified position and displaced medially, the spike it forms tends to stabilize within the canal of the distal fragment (A). The angle of the Altdorf clamp is 130 levels, but the clamp could be bent with pliers or plate benders to the required angle. The Altdorf clamp is designed to be pushed into the cut surface of the proximal fragment and not by way of the lateral cortex. Medial displacement is controlled by the purpose at which the splines of the clamp enter the proximal fragment. The more medially the splines enter the proximal fragment, the more medial is the displacement achieved. The amount of varus achieved is decided by the angle at which the blade enters the femoral neck. To choose the angle for insertion of the blade, the fragments are held in the desired place whereas the splines are first pushed into the cancellous bone of the femoral neck and then impacted with a mallet. Finally, a 4-mm cancellous screw is inserted through the proximal round hole into the proximal fragment. Traditionally, the remedy choices for residual acetabular dysplasia are divided into four groups. The first group consists of osteotomies of the pelvis that redirect the complete acetabulum. This redirection offers coverage of the femoral head by acetabular articular cartilage. These procedures involve full cuts through varied pelvic bones and rotation of the acetabulum. The general prerequisites for rotational osteotomy embody full concentric discount and release of muscle contractures, including the iliopsoas and hip adductors; a congruous joint; and a great range of motion. Rotational pelvic osteotomies within the face of subluxation may lead to severe damage to the femoral head. These procedures are finest carried out earlier than 6 years of age, however the age limits range significantly, depending on the surgeon. Radiograph (A) showed persistent widening of the joint and failure of the acetabulum to transform. The position of the femur was ascertained interoperatively by image intensifier (B). The place of the femoral head in relation to the acetabulum and the healing osteotomy is proven 6 weeks after surgery (C). The fact that this method of fixation is used most often in younger children together with other procedures for congenital dislocation of the hip implies that a cast is often required. In addition, the issue in executing this osteotomy to perfection, which is what produces the compression and stability (along with the malleable plate and only two screws for fixation), tends to make most surgeons uncomfortable treating kids without cast immobilization. In 1961, Salter described an operation primarily based on a new precept: redirection of the whole acetabulum as a unit. This was completed by performing a transverse osteotomy of the ilium simply above the acetabulum and opening the osteotomy anterolaterally by hinging and rotating the acetabular section on the symphysis pubis (322, 323). A 10-year-old woman whose developmental dysplasia of the hip was diagnosed at 5 years of age. She had previously undergone open reduction, but had residual proximal femoral and acetabular deformities. B: Three years after varus derotation osteotomy and Staheli slotted acetabular augmentation. One of the most obvious and common errors is the failure to obtain a concentric discount earlier than performing the osteotomy. The Salter innominate osteotomy provides about 15 levels of lateral coverage and 25 levels of anterior coverage, although many clinicians imagine that more lateral coverage can be obtained. B: Anteroposterior view of the pelvis with abduction, flexion, and slight internal rotation; the femoral head seems slightly uncovered. Note the wonderful protection of the proximal femur by unossified acetabular cartilage. The double-innominate osteotomy of Sutherland and Moore, though not often carried out right now, goals to allow larger rotation of the pelvic fragment by chopping through the pubis, instead of merely hinging on it (420). Complications of this process can contain harm to the spermatic cords, bladder, and urethra. The triple-innominate osteotomy allows even larger protection by the use of cuts of all three hip bones (234). It is a reconstructive process because it uses the articular cartilage and the subchondral bone of the acetabulum. Subsequent stories have demonstrated the effectiveness of this procedure (234, 426ʹ31). As within the Salter osteotomy, a prerequisite for the triple-innominate osteotomy is that the femoral head and the acetabulum are congruous after the osteotomy is completed. Some surgeons have adapted the strategy used by Le Coeur (451) in his osteotomy to divide the ischium and the pubis by way of a groin incision just like that utilized in adductor myotomy or proximal hamstring release. The periosteum is elevated carefully from the sciatic notch with a curved periosteal elevator, similar to a Crego or Cobb elevator.
Cheap clindamycin 150 mg with visa
Frejka pillow and Becker gadget for congenital dislocation of the hip: potential 6-year study of 104 latediagnosed cases does antibiotics for acne work clindamycin 150 mg generic line. The Pavlik harness within the therapy of congenital dislocating hip: report on a multicenter examine of the European Paediatric Orthopaedic Society triple antibiotic ointment clindamycin 300 mg purchase free shipping. Comparison of the Frejka pillow and the von Rosen splint in therapy of congenital dislocation of the hip. The von Rosen splint compared with Frejka pillow: a examine of 408 neonatally unstable hips. Treatment of congenital dislocation of the hip by the Pavlik harness: mechanism of reduction and utilization. Abduction treatment in late identified congenital dislocation of the hip: follow-up of 1,010 hips handled with the Frejka pillow 1967ͷ6. Stirrups as an aid within the remedy of congenital dysplasias of the hip in children. The functional technique of treatment utilizing a harness with stirrups as the primary technique of conservative therapy for infants with congenital dislocation of the hip, 1957 (classical article). The natural historical past of developmental dysplasia of the hip after early supervised therapy in the Pavlik harness. Use of the Pavlik harness in congenital dislocation of the hip: an evaluation of failures of treatment. Developmental hip dysplasia potentiated by inappropriate use of the Pavlik harness. Avascular necrosis price in early discount after failed Pavlik harness therapy of developmental dysplasia of the hip. Congenital dislocation of the hip: use of the Pavlik harness in the baby through the first 6 months of life. Residual dysplasia after profitable Pavlik harness therapy: early ultrasound predictors. Inferior (obturator) dislocation of the hip in neonates: a complication of treatment by the Pavlik harness. Obturator dislocation in developmental dislocation of the hip: a complication throughout treatment. Avascular necrosis in patients treated with the Pavlik harness for congenital dislocation of the hip. Avascular necrosis and the Pavlik harness: the incidence of avascular necrosis in three types of congenital dislocation of the hip as categorised by ultrasound. Management strategy for prevention of avascular necrosis throughout treatment of congenital dislocation of the hip. Avascular necrosis of the capital femoral epiphysis as a complication of closed discount of congenital dislocation of the hip. Closed reduction by two-phase pores and skin traction and useful splinting in mitigated abduction for remedy of congenital dislocation of the hip. The impact of traction treatment on the outcomes of closed or open reduction for congenital dislocation of the hip: a preliminary report. The treatment of congenital dislocation and subluxation of the hip within the older child. Congenital dislocation of the hip: the relationship of premanipulation traction and age to avascular necrosis of the femoral head. Treatment of congenital dislocation of the hip in kids between the ages of one and three years. The impact of traction treatment on blood flow in the immature hip: an animal study. Closed reduction with traction for developmental dysplasia of the hip in youngsters aged between one and 5 years. Derotational femoral shortening for developmental dislocation of the hip: special indications and results in the kid younger than 2 years. Latepresenting developmental dysplasia of the hip handled with the modified Hoffmann-Daimler functional technique. Current apply in use of prereduction traction for congenital dislocation of the hip. Open discount by the Ludloff strategy to congenital dislocation of the hip underneath the age of two. Preliminary traction as a single determinant of avascular necrosis in developmental dislocation of the hip. The value of preliminary traction within the treatment of congenital dislocation of the hip. Tangential view arthrogram at closed discount in congenital dislocation of the hip. Prognostic elements in congenital dislocation of the hip treated with closed reduction: the significance of arthrographic evaluation. The function of arthrographyguided closed discount in minimizing the incidence of avascular necrosis in developmental dysplasia of the hip. A dynamic canine mannequin of experimental hip dysplasia: gross and histological pathology, and the effect of place of immobilization on capital femoral epiphyseal blood flow. Incidence of avascular necrosis of the femoral head in congenital hip dislocation related of the degree of abduction throughout preliminary traction. Avascular necrosis of the femoral head as a complication of remedy for congenital dislocation of the hip in young kids: a clinical and experimental investigation. The prognostic significance of the ossific nucleus in the therapy of congenital dysplasia of the hip. A new open reduction treatment for congenital hip dislocation: long-term follow-up of the in depth anterolateral strategy. Role of innominate osteotomy within the treatment of congenital dislocation and subluxation of the hip in the older youngster. Innominate osteotomy in the management of residual congenital subluxation of the hip in young adults. Long-term outcomes after open discount of developmental hip dislocation by an anterior strategy lateral and medial of the iliopsoas muscle. A new capsuloplasty technique in open reduction of developmental dislocation of the hip. Medial approach open reduction with out preliminary traction for congenital dislocation of the hip. Medial strategy open discount for congenital dislocation of the hip utilizing the Ferguson procedure. Indications for therapy of congenital dislocation of the hip by the surgical medial approach. Early results of medial method open reduction in congenital dislocation of the hip: use earlier than strolling age. Open reduction for congenital dislocation of the hip using the Ferguson procedure. A comparative evaluation of the current methods for open discount of the congenitally displaced hip. Open discount (Ludloff approach) of congenital dislocation of the hip earlier than the age of two years.
Order clindamycin 150 mg mastercard
This is a consensus definition that has been just lately adopted in the medical literature (237 oral antibiotics for acne side effects clindamycin 300 mg effective, 308 antibiotic guidelines 2015 order clindamycin 150 mg line, 478 480), however has not been officially adopted in medical dictionaries. Lateral radiograph of the hindfoot exhibiting the conventional irregularities of ossification of the apophysis of the os calcis within the growing youngster. A, B: Apparent metatarsus adductus, but with the head of the talus visible and palpable medially. This signifies coexistent eversion of the subtalar joint with abduction of the navicular on the top of the talus. Inconsistent terminology was used in the three seminal articles on this deformity within the English literature. Peabody and Muro (449) labeled it congenital metatarsus varus, McCormick and Blount (438) coined the term skewfoot, and Kite (436) known as it serpentine metatarsus adductus. Consistency in these articles was found within the reported rarity of the deformity and the problem in correcting and maintaining correction of the deformity. The lack of a strict definition has contributed to the lack of information on this deformity, together with its incidence, etiology, pure history, and therapy. Some researchers have said that the deformity occurs as a outcome of improper cast remedy of metatarsus adductus and clubfoot. Some authors imagine that a skewfoot deformity can be created in a foot with metatarsus adductus by applying abduction stress to the forefoot with out stabilizing the hindfoot when manipulating, casting and bracing these ft (5, 446). A thickened portion of the tibialis anterior courses alongside an oblique dorsal-to-plantar groove on the concave medial border of the medial cuneiform (308, 478). Little has been written on the medical options of skewfoot deformities, so I will present my personal observations on a reasonably large variety of these deformities. It is difficult to differentiate skewfoot from metatarsus adductus in an infant, however sure traits are useful. The plantar floor of the skewfoot is S-shaped, whereas the foot with metatarsus adductus is C-shaped. In the infant and young youngster with skewfoot deformity, the Achilles tendon has full flexibility and the ankle may be easily dorsiflexed. This creates discordance in the scientific look of the foot within the frontal and sagittal planes, a characteristic that modifications with age in some kids. Young youngsters with persistent and inflexible forefoot adductus deformity occasionally current with ache and callus formation at the base of the fifth metatarsal or the medial side of the hallux. Valgus deformity of the hindfoot with flattening of the longitudinal arch and adductus of the forefoot could be better appreciated in older children, adolescents, and adults with skewfoot, although the deformity is commonly misclassified, even in the orthopaedic literature. There is now concordance within the medical look of the foot in the frontal and sagittal planes. Shortening of the tendo Achillis is famous within the older youngster, adolescent, and grownup with symptomatic skewfoot (237, 308, 478, 479). Because of the issue in differentiating these two foot deformities in infants, a few of the so-called metatarsus adductus feet in these research might have truly been skewfeet. Painful callus that developed underneath the pinnacle of the talus in a skewfoot with contracted Achilles tendon. The classification system was found to have poor interobserver and intraobserver reliability by Cook et al. Preoperative, intraoperative, and postoperative radiographs of a painful skewfoot in a 13-year-old adolescent. Calcaneal lengthening osteotomy, medial cuneiform opening-wedge osteotomy, and Achilles tendon lengthening were used. He also recognized the flaw in using the usual talusΦirst metatarsal angle to assess deformity between the forefoot and the hindfoot (237). The skewfoot has two deformities in opposite instructions from one another between the talus and the primary metatarsal in both the frontal and sagittal planes. These angular deformities tend to cancel each other out when the talusΦirst metatarsal angle is measured. For that purpose, a skewfoot with extreme valgus deformity of the hindfoot will seem much less deformed than a flatfoot with much less valgus deformity when both are assessed clinically and radiographically. One would assume that some youngsters undergo spontaneous correction of their skewfoot deformities with age, as occurs with isolated metatarsus adductus (5, 6) and flexible flatfoot (9, 10). The prevalence of long-term incapacity as a result of residual deformity is unknown, but some youngsters have pain, callosities, and issue sporting shoes as early as the tip of the first decade of life (237, 308, 436ʹ38, 449, 478ʹ80). Several authors have reported success with this strategy, noting that it takes longer to right a skewfoot and that further care have to be exercised to keep away from valgus stress on the already deformed hindfoot (5, 436ʹ38, 444, 446). Berg (446) cautioned in opposition to the usage of reverse final footwear and Denis-Browne bars for a similar purpose. Rarely, a child in the midst of the first decade of life will present with ache and callus formation at the base of the fifth metatarsal or the medial facet of the hallux, because of a extreme and rigid adductus part of a skewfoot deformity. Recommendations within the literature for correction of the forefoot adduction component of skewfoot in this age group embody tarsometatarsal capsulotomies (456), metatarsal base osteotomies (459), and medial cuneiform opening-wedge osteotomy (77, 223), presumably mixed with closing cuboid wedge osteotomy (224). Some older youngsters, adolescents, and adults with skewfoot deformity will report pain and callusing under the distinguished head of the plantar-flexed talus (237, 308, 478, 479). Attempts can be made to stretch the Achilles tendon by the use of exercises or casts. Rigid orthoses increase the stress beneath the top of the rigidly plantar-flexed talus and must be prevented. Less generally, children with skewfoot will present with isolated or coexisting pain and callosities on the head of the primary metatarsal or the bottom of the fifth metatarsal (479). An operation is indicated when nonoperative administration fails to relieve the pain and callosities (237, 308, 478, 479). Suggestions for operative management could be found within the literature, however most are based on theory and never on a evaluation of operative outcomes. Historical suggestions have been for tarsometatarsal capsulotomies or osteotomies on the base of the metatarsals to correct the forefoot deformity (449) with subtalar or triple arthrodesis for the hindfoot (458, 459, 480). Reported issues from these procedures on the forefoot are enumerated within the part of this chapter on metatarsus adductus (457ʹ59, 461, 462). Reported complications and incapacity from subtalar and triple arthrodesis are enumerated in the section of this chapter on flatfoot (19Ͳ7). Mosca (478) proposed correction of symptomatic skewfoot by combining one of the best and safest strategies for correcting the individual deformities of the forefoot and hindfoot. In 1993, he reported the short-term outcomes of the biggest sequence of operatively handled skewfoot deformities utilizing a single technique. The method consists of a calcaneal lengthening osteotomy, conceptualized by Evans (236) and elaborated by Mosca (237, 238); a medial cuneiform opening-wedge osteotomy, in accordance with Fowler et al. Nine of ten extreme skewfoot deformities achieved a passable scientific and radiographic consequence whereas sustaining joint mobility. The webbing may be full to the ends of the toes or it might be extremely shallow and refined. They should be performed if deformity, from differential length of the toes, is present and surgical administration is planned.