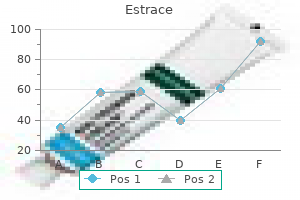
Estrace
Estrace dosages: 2 mg, 1 mg
Estrace packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

2 mg estrace trusted
This means that different causal genes for major lymphoedema have yet to be identified women's health issues research paper buy cheap estrace 1 mg. Differential diagnosis Differential diagnoses include lipoma menstrual 7 days late purchase estrace 2 mg, lymphatic malformation, lymphocele and sarcoma. A total of 65 circumstances of huge localized lymphoedema have been described in the literature, nine of which resulted in angiosarcoma (10. Prognosis the likelihood is that the lesion will proceed to enlarge and undergo continual sepsis unless treated. There is oedema each throughout the mass and tracking along the subcutaneous septae in a lacelike trend outwards from the pedicle, outlining large lobules of fats [4]. A new classification system and diagnostic pathway has been developed to find a way to delineate particular primary lymphoedema phenotypes, and facilitate the discovery of recent causative genes [1,10]. Phenotyping and genotyping of sufferers with major lymphoedema results in a greater understanding of the natural history and management of specific circumstances and extra correct recurrence dangers for future generations. More recently, chronic lymphoedema (of main and secondary causes) was estimated to have an result on as many as 1. Further epidemiological research are needed to establish the true prevalence of main lymphoedema. These five classes are discussed in flip below, including the scientific phenotypes and causal gene mutations. Clinical options Syndromic Lymphoedema is a acknowledged feature of many syndromes. Turner syndrome should all the time be suspected as the trigger of congenital hand and/or foot swelling in female infants. Lymphoedema with systemic/visceral involvement A widespread developmental abnormality of the lymphatic system results in systemic/visceral involvement and swelling that will not be confined to the limbs. Lymphatic dysfunction could current prenatally with hydrothoraces or hydrops fetalis. The improvement of in utero oedema could cause dysmorphic facial features corresponding to epicanthic folds, a broad nasal bridge and neck webbing with lowset ears [15]. Systemic lymphatic abnormalities may present with pericardial and pleural effusions, chylous ascites and pulmonary and intestinal lymphangiectasia in the postnatal interval. An particular person with intestinal lymphangiectasia will complain of stomach ache and diarrhoea following the ingestion of foods with a high fat content (as the intestinal lymphatics are liable for fats absorption). Management contains the drainage of effusions and implementation of a mediumchain triglyceride diet to handle intestinal lymphangiectasia and chylous issues [16]. The swelling affects totally different physique parts in association with a systemic lymphatic abnormality. For instance, they could have lymphoedema of one or more limbs or physique sites (including the Presentation Primary lymphoedema could additionally be current at delivery or develop later in life. One or extra limbs may be affected, or indeed there could also be generalized/whole physique swelling, relying on the subtype of lymphoedema. The medical indicators of lymphoedema can range from delicate swelling to that of grotesque enlargement in chronic, poorly managed patients. Papillomatosis (small fleshcoloured papules) occurs on account of dilatation throughout the higher dermal lymphatics and subsequent fibrosis of the dermis. Lymphangiectasia seems as small blisters on the skin floor because of engorgement of lymphatic vessels. Lymph fluid regularly leaks because of minimal trauma and is termed lymphorrhoea. Part 9: Vascular Clinical variants A variety of subtypes of primary lymphoedema exist. They each current with differing age of swelling onset, distribution of lymphoedema and attainable associated well being problems. However, the pathway remains a work in progress as new subtypes and causal genes are discovered [10]. Isolated pedal oedema is excluded from this definition as this might be a presentation of Milroy illness A area of the physique affected by lymphoedema. This consists of hydrops fetalis, chylous ascites, intestinal lymphangiectasia, pleural and pericardial effusions and pulmonary lymphangiectasia Includes congenital vascular abnormalities Part 9: Vascular Late onset unisegmental lymphoedema one hundred and five. Associated issues embrace hypothyroidism, glaucoma, seizures, hearing loss and renal abnormalities [18,19]. Lymphoscintigraphy has not often been undertaken in this situation however Bellini et al. Lymphoedema related to disturbed progress and/or cutaneous/vascular anomalies Lymphoedema might develop in affiliation with vascular abnormalities, disorders of development and cutaneous abnormalities. Identifying the type of malformation and thereby the vessels concerned is essential for analysis and administration. The current identification of de novo somatic mutations as the underlying mechanism for a few of these situations might additional understanding and enhance management. This has allowed separation of these circumstances inside the diagnostic pathway, and has recognized gene pathways that could presumably be targeted by pharmacological therapy [27]. The similar gene and same mechanism have also been implicated in a couple of patients with Klippel�Trenaunay syndrome and with fibroadipose hyperplasia [26,27]. Further molecular studies, along with cautious phenotyping, will facilitate the understanding of this spectrum of disease. It is in all probability going that combined vascular malformations may arise as a result of somatic mosaicism. Patients current with a mixture of several or all the following inside a single limb: limb length hypertrophy of muscle, fats or bone. The underlying mechanism is believed to be of somatic mosaicism, and no recognized causal genes have been identified to date. Swelling usually impacts all body elements and sometimes presents in utero with hydrops fetalis. Proteus syndrome is a disease characterized by progressive, segmental overgrowth of the bones, pores and skin and connective tissue. Lymphatic and capillary malformations are the most common vascular adjustments seen in this syndrome. The analysis could also be established using diagnostic clinical criteria and/ or molecular analysis [28]. Patients with congenital multisegmental lymphoedema with out systemic lymphatic impairment have been included inside the yellow part of the classification pathway in order to keep away from confusion with multisegmental lymphoedema occurring in association with systemic lymphatic abnormalities (in the pink section of the pathway). These sufferers have an asymmetrical sample of lymphatic failure with some limb sparing. It is feasible that somatic mosaicism in gene(s) concerned in lymphangiogenesis may explain this subtype of congenital main lymphoedema. These sufferers have in depth, asymmetrical, multisegmental lymphoedema comprising facial and conjunctival oedema, genital lymphoedema, and epidermal naevi and/or capillary malformations usually of the torso and upper limbs. These patients have a sporadic situation, suggesting probable somatic mosaicism [10]. Lymphoscintigraphy in Milroy disease confirms failure of the initial lymphatic vessels to absorb fluid. The initial lymphatic vessels are current (confirmed on histological examination) but unable to take in interstitial fluid [33].
Purchase 2 mg estrace
Secondary cicatricial alopecia Traumatic Radiodermatitis Mechanical trauma Postoperative women's health center hershey pa estrace 1 mg buy discount online. Lesions usually current as annular menopause 100 years ago estrace 1 mg cheap on line, pink or yellow plaques, with or without atrophy and telangiectasia, and infrequently contain the forehead and frontal scalp [1]. Distinguishing between necrobiosis lipoidica, granuloma annulare and sarcoidosis can be tough on clinical grounds alone [2,3]. After having this lesion since adolescence, this lady later developed biopsyproven lichen sclerosus of the vulva. Scleroderma and morphoea Introduction and basic description Scleroderma (see Chapter 56) may end up from numerous localized or generalized connective tissue disorders. Morphoea (see Chapter 57) is a definite autoimmune connective tissue disorder that may have an effect on the scalp and produce localized areas of cicatricial alopecia. In early lesions of scalp morphoea, the centrifugally increasing lilac border is commonly obscured by hair. Lesional pores and skin is thickened and indurated; as properly as pallor there could additionally be marginal hyperpigmentation. Histological examination shows persistent inflammation of the higher and midfollicle and prominent fibrosis [2]. The sclerodermatous phase of continual graftversushost illness may contain the scalp to produce a cicatricial alopecia. Initially, lesions may be papular or nodular and coalesce to form plaques, which flatten to leave areas of cicatricial alopecia exhibiting variable degrees of erythema and scaling. These plaques may have a barely raised annular border, however are otherwise nondescript. In the absence of characteristic lesions elsewhere on the skin or a identified diagnosis of sarcoid, the diagnosis is made by demonstrating the attribute naked, noncaseating, epithelioid granulomas on biopsy. Oral corticosteroids, penicillamine, sulfasalazine and chloroquine have all been used with varying success. Surgical excision of en coup de sabre could provide definitive treatment, although recurrences occur, particularly if the lesion is enlarging at the time of excision. Longterm maintenance therapy with lowdose methotrexate as a steroidsparing agent is usually successful. The prognosis is variable, but therapy is required for a minimum of 6 months within the majority of patients. Follicular mucinosis Introduction and common description Follicular mucinosis happens in two forms: a major idiopathic kind and a secondary type. The secondary type is most commonly related to lymphoma, particularly mycosis fungoides, but can be related to persistent discoid lupus erythematous, angiolymphoid hyperplasia with eosinophilia, and with verruca vulgaris. Epidemiology Follicular mucinosis is a uncommon condition, with no reported racial predilection but is extra frequent in males than females. Primary follicular mucinosis can happen at any age from early childhood onwards, however is most common between 10 and forty years. Pathophysiology All cases require a biopsy to confirm the prognosis and to look for histological proof of mycosis fungoides. The histology is characteristic and demonstrates degeneration of the hair follicles and sebaceous glands related to copious mucin (hyaluronic acid), especially in the outer root sheath of the hair follicle. A variable dermal inflammatory infiltrate is current and should be studied carefully for proof of mycosis fungoides. In such instances only regular followup of the patient will distinguish primary from secondary causes of follicular mucinosis. Management Many instances spontaneously enhance, nonetheless topical or intralesional steroids are generally effective. Superficial radiotherapy and phototherapy helps follicular mucinosis secondary to mycosis fungoides. Hydroxychloroquine has been reported as a successful treatment inducing rapid remission and hair regrowth in idiopathic follicular mucinosis [2]. Widespread pruritic lesions could profit from lowdose systemic steroids or often dapsone. It is an autoimmune, persistent, bullous disease that preferentially impacts mucosal surfaces and heals with scarring. It predominantly affects the aged; girls are extra generally affected than males [1,2]. Although the illness preferentially impacts the ocular and/ or genital mucous membranes, the pores and skin is involved in 40�50% of circumstances, and skin lesions might precede the mucosal lesions by months or years [3]. The favoured sites are the face and higher trunk, nonetheless the scalp is concerned in roughly 10% of instances. Skin lesions, predominantly on the head and neck, are the major feature of the Brunsting� Perry variant. Clinical options Follicular mucinosis consists of grouped, typically itchy, follicular papules and erythematous, boggy plaques that happen primarily on the scalp and face, however can occur anyplace. Characteristically the plaques are devoid of hair; close inspection will reveal patulous follicular openings. In the secondary group the lesions could also be extensively disseminated on the trunk and limbs. Systemic corticosteroids and immunosuppressants could also be required for more widespread and severe disease. Dissecting cellulitis of the scalp Definition and nomenclature Dissecting cellulitis manifests with a perifolliculitis of the scalp, deep and superficial abscesses within the dermis, sinus tracts formation and in depth scarring [1]. Although staphylococci, streptococci and Pseudomonas may be cultured from various lesions, no specific causative organism has been isolated. Dissecting cellulitis is associated with hidradenitis suppurativa and acne conglobata within the follicular occlusion triad [2]. Other problems of the follicular occlusion triad could additionally be current and there may be an related pilonidal sinus (the follicular occlusion tetrad) or spondyloarthropathy. Differential diagnosis Clinical differential diagnoses embody kerion, pyoderma gangrenosum and erosive pustular dermatosis of the scalp. Fungal cultures and a scalp biopsy for routine histology and direct immunofluorescence will exclude other causes of scarring alopecia. Abscess formation results, and results in destruction of the pilosebaceous follicles initially, and ultimately the opposite cutaneous appendages. Keratin fragments induce a granulomatous response, with overseas physique big cells, lymphoid and plasma cells. Management Although systemic antibiotics and topical or intralesional corticosteroids are typically helpful, relapses are frequent and the course is often protracted. Because the irritation is predominantly perifollicular, a shocking amount of regrowth may happen. The antibiotics could be stopped after 4 weeks and the prednisolone gradually tailed off and replaced by topical steroids.
Order estrace 2 mg fast delivery
It is often seen in lipodermatosclerosis and traumatic panniculitis menstruation new moon estrace 2 mg generic free shipping, but may be current in erythema nodosum and erythema induratum of Bazin women's health center memorial city discount 2 mg estrace mastercard. Necrotic adipocytes injured by this mechanism appear as granular wisps of amphophilic detritus and their cellular buildings are now not evident. Enzymatic fat necrosis is a particular kind of liquefactive fat necrosis characteristically noticed in pancreatic panniculitis. It is due to saponification of the adipocyte lipid contents by pancreatic lipase, with secondary deposition of calcium salts, resulting in socalled ghost adipocytes, which encompass adipocytes with no nuclei and granular basophilic cytoplasm. Hyalinizing fat necrosis is characteristically observed in lupus panniculitis and panniculitis associated with dermatomyositis. In this pattern, necrotic adipocytes seem as mummified anucleated cells, which are surrounded by glassy homogeneous proteinaceous material, effacing the structure of the fat lobule. When membranous fat necrosis is in depth, formation of cystic structures devoid of cellular elements and lined by hyalinecrenulated membrane may be observed. Membranous and membranocystic fat necrosis are almost always seen in lipodermatosclerosis, however like other types of fat necrosis, they might also be seen in latestage lesions of a number of forms of panniculitis. Ischaemic fats necrosis is extra regularly seen on the centre of fat lobules and is characterized by pallor of adipocytes, which are smaller than normal due to severe impairment of blood provide. Ischaemic fats necrosis is frequently seen in erythema induratum of Bazin, but can also be noticed in different panniculitides, together with calcific uraemic arteriolopathy (calciphylaxis), infectious panniculitis and cutaneous polyarteritis nodosa. Finally, basophilic fat necrosis outcomes from necrosis of adipocytes intermingled with nuclear mud of neutrophils and granular basophilic material, which characterize aggregations of bacteria and is characteristically seen in cases of infectious panniculitis. There are some disorders that should not be thought-about as specific variants of panniculitis. Weber�Christian disease is the time period that has been classically used to refer to circumstances of predominantly lobular panniculitis without vasculitis in association with systemic manifestations together with fever and involvement of visceral fat tissue. Additional phrases such as idiopathic nodular panniculitis, nodular panniculitis and relapsing febrile non suppurative nodular panniculitis have been used as synonyms for Weber�Christian disease. However, many cases initially thought of as examples of Weber�Christian illness were later reclassified when different variants of lobular panniculitis, together with erythema induratum of Bazin (nodular vasculitis), pancreatic panniculitis and 1antitrypsin deficiency panniculitis were separated as particular ailments. The authors concluded that the term Weber�Christian illness ought to be abandoned as a prognosis for circumstances of lobular panniculitis because now a more particular diagnosis could also be reached within the majority of instances. The identical is true for Rothmann�Makai disease, a time period that was used beforehand to describe instances of relapsing nodular panniculitis much like that of Weber�Christian disease but with no fever or other systemic manifestations. Varicosities and erythematous nodules with linear arrangement involving the best lower extremity. The causes of secondary hypercoagulable states are varied, however within the majority of cases venous insufficiency of the lower extremities is the only precipitating issue. The course of is extra inflammatory than thrombotic, with distinguished fibrinoid necrosis of the tunica intima, resulting within the socalled targetlike arteritis, in which an eosinophilic ring of fibrinoid necrosis replaces the intima of the affected arteriole. Some authors, nevertheless, consider that when irritation is current within and around the wall of the vessel, the identification of the interior elastic lamina of the concerned vessel is much less reliable even with elastic tissue stains, and the graceful muscle pattern has the highest sensitivity and specificity for distinguishing arteries from veins [17]. In early lesions, the inflammatory cell infiltrate consists mostly of neutrophils, whereas in later phases there are lymphocytes, histiocytes and occasional multinucleated giant cells. Direct immunofluorescence studies of lesions of cutaneous pol- yarteritis nodosa have demonstrated IgM and complement deposition within the concerned vessel walls and constant absence of IgG [3]. The involved vessel appears with a thickened wall, within which an inflammatory infiltrate is seen. In early lesions, a neutrophilic infiltrate and leukocytoclasis are sometimes seen and, in some cases, eosinophils could also be outstanding [4]. Characteristically, the intima of the concerned artery exhibits an eosinophilic ring of fibrinoid necrosis, giving a targetlike appearance to the damaged vessel. A uncommon complication is the formation of periosteal new bone beneath the cutaneous lesions [5]. Often, arterial involvement is segmental and serial sections throughout the complete specimen are required to demonstrate the pathology. As is the case in superficial thrombophlebitis, lesions of cutaneous polyarteritis nodosa present little or no involvement of the adjacent fats lobule, and the process is exclusively a septal arteritis. It is associated in the majority of however not all instances with underlying diabetes, the onset of which it might precede. There are palisading granulomas with histiocytes surrounding areas of degenerate collagen within widened septa. The most attribute characteristic supporting a analysis of necrobiosis lipoidica as the cause for an inflammatory course of involving the subcutis is the coexistence of similar lesions in the dermis, with alternating horizontal bands of inflammatory cells and fibrosis involving the whole dermis [2]. Early lesions present an inflammatory infiltrate composed predominantly of neutrophils scattered within the septa, whereas in later lesions, histiocytes, lymphocytes and plasma cells, typically with lymphoid follicle formation [3], are predominant. Multinucleated giant cells involving the septa are typically outstanding and in these instances histopathological findings resemble erythema nodosum. In chronic longstanding lesions, the dermis and the superficial subcutaneous tissue are changed by horizontal fibrosis with sclerotic collagen bundles organized parallel to the dermis and scattered by plasma cells, carefully resembling the findings seen in morphoea. In these latestage lesions, features of necrobiosis are now not evident and elastic tissue stains show dramatic loss of elastic fibres. Some authors have postulated that the discovering of vasculitis and leukocytoclasis in lesions of necrobiosis lipoidica is indicative of an underlying systemic illness [4]. Membranous fats necrosis has additionally been described in latestage lesions of necrobiosis lipoidica extending to the subcutaneous tissue [5]. The lesions consisted of indurated, hyperpigmented and barely depressed plaques. Although classical morphoea often extends from the deep dermis to the subcutaneous tissue, morphoea is usually a completely panniculitic course of with no involvement of the epidermis, cutaneous adnexa or dermis. The course of is thought variously as morphoea profunda, nodular scleroderma or keloidal scleroderma. The inflammatory cells launch cytokines, together with macrophage inhibitor issue, which trigger histiocytes (b) determine 99. When the sclerotic process involves each dermis and subcutis, the total thickness of the specimen seems homogeneously eosinophilic. Inflammatory infiltrate is present solely in active lesions, consisting of aggregates of lymphocytes surrounded by plasma cells at the interface between the thickened septa and the fat lobules. Plasma cells could additionally be additionally current arranged interstitially between the sclerotic collagen bundles [2�4]. Active lesions of deep morphoea normally show denser infiltrate than dermal morphoea [4�6]. Eosinophilic fasciitis (Shulman syndrome) is considered a variant of deep morphoea during which the thick and sclerotic septa and the fascia present inflammatory infiltrate of lymphocytes, histiocytes, plasma cells and ample numbers of eosinophils [7�14]. Histopathological examine of early stages of eosinophilic fasciitis reveals oedema and infiltration by eosinophils, lymphocytes and plasma cells between the collagen bundles of the connective tissue septa of the subcutis and subcutaneous fascia.
2 mg estrace with mastercard
Freer or Locke elevator pregnancy exercise buy estrace 1 mg amex, or a dental spatula) women's health clinic temecula ca 2 mg estrace buy with mastercard, a nail splitter, straight haemostat, nice iris or Gradle scissors, no. Diagnostic surgery proximal nail fold biopsy Three techniques are available for biopsying this area as follows: � When the indication is similar to a biopsy elsewhere on the skin, a punch biopsy (not over three mm) may be taken on the proximal nail fold, taking care that its distal margin is always preserved. This amount of tissue allows histology, immunohistology and electron microscopy to be performed [18]. The process is similar because the surgical treatment of persistent paronychia (see later). Nail mattress biopsy Indications for nail bed biopsies are diseases of the nail bed presenting as onycholysis, subungual hyperkeratosis or tumour. In the absence of onycholysis, a partial or whole nail avulsion (see later) should be carried out to expose the realm to be biopsied. As for pores and skin, incisional biopsy is carried out with a punch and excisional biopsy with a blade. No suture is required, as a defect up to four mm throughout will heal by secondary intention without dystrophy. The nail mattress may be very fragile and tightly adherent to the bone in order that reapproximation of the margins may be troublesome. Dystrophic sequelae are unlikely if the pigment is confined to the distal matrix, as the latter synthesizes the ventral a part of the nail plate. Fortunately, within the majority of circumstances longitudinal melanonychia originates in the distal matrix [19]. If the pigment is situated inside or extends to the proximal matrix, a nail plate dystrophy is extremely probable, as this part of the matrix generates the higher third of the nail plate. Each of the following procedures begins identically so as to expose the nail matrix. Using an elevator, the proximal nail fold is detached from the nail plate; two lateral incisions at 45� enable it to be mirrored. The defect is left open and the nail plate is laid back in place and sutured to the lateral nail fold. Punching by way of the nail plate at the origin of the longitudinal melanonychia before avulsing may be very helpful when coping with lightly pigmented bands: the process of avulsion usually detaches the superficial layers of the matrix epithelium and the origin of the band could then be tough to determine. By performing a punch on this manner, the realm to biopsy can be clearly seen as quickly as the nail plate has been avulsed [21]. The proximal nail fold is returned to its anatomical position and the lateral incisions are sutured [21]. The borders of the defects are generously undermined and the edges are gently reapproximated with 5/0 or 6/0 absorbable sutures. The avulsed nail plate and proximal nail fold are then changed as described above. The scalpel is then held horizontally and with sawing motions the lesion is faraway from the deep dermis. Its primary downside is a recurrence of the pigmentation in about three quarters of instances [22]. This method avoids mutilating surgery in circumstances the place the pigment derives from a large benign lesion. If histopathology exhibits that the lesion is malignant, additional surgery is required. This is probably the most rewarding biopsy method when dealing with a disease presenting as alterations of the nail plate Nail surgical procedure ninety five. This will slim the nail completely as a result of the partial amputation of the lateral horn of the matrix. The incision starts half method between the cuticle and the crease of the distal interphalangeal joint and runs distally via the proximal nail fold, the nail plate and its mattress to the hyponychium. At the junction of the lateral and proximal nail fold, the incision ought to comply with a laterally curved direction extending midway down the lateral facet of the finger so far as the distal interphalangeal joint, to have the ability to ensure removal of the lateral horn of the matrix. A second incision, starting from the distal extremity of the previous one, runs from the hyponychium into the lateral sulcus and joins the proximal end of the previous incision. At the proximal end of the biopsy, care should be taken to embody the matrix by avoiding lifting the scissors too quickly and thus foreshortening the specimen. The defect is reapproximated with horizontal mattress sutures in order to recreate a lateral nail fold [24]. An elevator is gently slid beneath the proximal nail fold in a again andforth movement from side to aspect, so avoiding injuring the delicate longitudinal nail bed ridges, until the proximal nail fold is free of the nail plate. The elevator is then pushed under the nail plate from the distal free edge until the elevator provides means (meaning the elevator has reached the matrix area to which the nail plate is loosely attached). A jaw of a sturdy haemostat is slid underneath the whole length of a lateral portion of the nail plate and grasped firmly. Proximal strategy the proximal strategy is suggested when the distal subungual space strongly adheres to the nail plate. The elevator then displays the proximal nail fold and is delicately inserted beneath the bottom of the nail plate the place the adherence to the matrix is weak. The avulsion progresses distally following the pure cleavage plane up to the hyponychium [25]. Total surgical removing must be discouraged: the distal nail mattress may shrink and turn out to be distorted dorsally. In addition, the lack of counterpressure from the nail plate allows dorsal growth of the distal pulp, promoting distal embedding. Partial surgical nail avulsion the appreciable benefit of this system is that it leaves a big portion of regular nail plate that also exerts a strain on the underlying gentle tissues, reducing the chance of distal embedding. Partial nail avulsion is part of many surgical procedures: chemical cautery of part of the matrix in ingrowing toenails, remedy of acute paronychia, surgical exploration of any nail bed or matrix tumour. It is performed in the identical method because the distal method methodology of complete surgical nail avulsion, however restricted to a limited portion of the nail plate. For exposure of the matrix space, avulsion of the proximal third of the nail plate is greatest. It starts with two lateral incisions on the proximal nail fold at 45� enabling it to be reflected. A jaw of a nail splitter is inserted underneath the lateral border of the nail plate, approximately 5 mm distal to the lunula. The incision should embrace the 5 most proximal millimetres of the lateral nail folds. In most cases, the fibrokeratoma originates from probably the most proximal part of the ventral proximal nail fold. The tumour ought to be delicately dissected up to its base utilizing fine iris scissors after which severed. The proximal nail fold is then laid again and secured with 5/0 stitches or adhesive strips [29].
Estrace 1 mg purchase line
Cyproterone acetate for extreme hirsutism: results of a doubleblind doseranging study breast cancer wristbands 2 mg estrace for sale. Spironolactone versus placebo or together with steroids for hirsutism and/or acne womens health zinio order estrace 2 mg online. Melanocyte stem cells: a melanocyte reservoir in hair follicles for hair and pores and skin pigmentation. Changes in tyrosinase activity during melanocyte proliferation within the hair development cycle. Combined chemical and electron microscopic studies of pheomelanosomes in human red hair. Variants of the melanocyte stimulating hormone receptor gene are related to purple hair and fair pores and skin in humans. Human hair greying is linked to a selected depletion of hair follicle melanocytes affecting each the bulb and the outer root sheath. Synonyms and inclusions � Acne (acne vulgaris) � Comedonal acne (acne comedonica) � Prepubertal zits � Nodulocystic zits (acne conglobata, conglobate acne) � Acne fulminans Introduction and common description Acne vulgaris is doubtless one of the commonest skin diseases worldwide, affecting all ethnicities and races [1�3]. The age of onset has modified over time, paralleling the earlier onset of puberty reported lately [4,5]. Acne generally has a protracted course, with acute or insidious relapse or recurrence over time. Clinical presentation contains noninflammatory and/or inflammatory lesions extending over the face and/or trunk. Successful treatment correlates with enchancment of psychological elements in many instances [6]. Despite the lowered prevalence with age, the burden of pimples stays excessive in adults [8]. Earlier growth of zits has been linked with earlier onset of puberty, which can also relate to diet/obesity and different way of life components [11,12]; however; earlier recognition can also lead to earlier presentation. Large communitybased surveys and detailed smaller scale research have shown that zits begins at a youthful age in women than boys aligning with earlier puberty [13�15]. Comedonal pimples can be detected in some youngsters before any overt indicators of puberty [16,17]. The early development of comedonal zits in girls may be a predictor of extra extreme disease in later life. Ethnicity Acne is now thought of to be amongst the ten most typical diseases worldwide [28]. However, ethnic variation within the prevalence of acne does appear to exist even when socioeconomic and cultural Table ninety. A giant multinational crosssectional study discovered that 26% of women aged 31�40 years and 12% of women aged 41�50 years had clinical acne (range 7�22%) relying on ethnicity [4,22]. Peak prevalence occurred between the ages of 15 and 20 years in all ethnic groups. A historical review [13] recognized numerous research displaying that males have more extreme pimples in late adolescence than ladies. Using the Rotterdam criteria, between 5 and 10% of adult women are classified as having the syndrome. Can be brought on by premature adrenarche or tumours (of the pituitary or adrenal mainly) Predisposes Predisposes Predisposes especially to early onset. Rotterdam diagnostic criteria � requires two of the following: 1 Oligo or anovulation 2 Clinical and/or biochemical signs of hyperandrogenism 3 Polycystic ovaries 90. Higher prevalences are seen in some Jewish, Mediterranean, MiddleEastern and Indian populations. The situation is most frequently diagnosed in late childhood or early maturity however can present as precocious puberty. If delicate, it can go unnoticed till signs corresponding to persistent acne, irregular menses or issues conceiving present. Affected topics might notice elevated sebum production [83] and in some circumstances zits is the only presenting symptom [80]. In the classical syndrome, sufferers present with sudden onset haemorrhagic and ulcerative zits on the face and trunk, sterile pustular lesions on the palms and soles and ache especially pimples vulgaris ninety. Adulthood Short stature Hirsutism Acne Testicular enlargement in boys Oligospermia Menstrual irregularities Infertility both sexes Childhood Tall stature Pseudoprecocious puberty Cystic zits Premature pubarche Box 90. In isolated circumstances, benefit has been famous following treatment with infliximab [89] and ustekinumab [90]. Patients current with typical signs of hyperandrogenism, hyperseborrhoea, hirsutism, acne, menstrual irregularities and androgenetic alopecia. They may show different options including deepening voice, clitoromegaly and increased muscle mass [93]. The primary abnormality is hyperinsulinaemia, elevated or upper restrict ranges of testosterone and androstenedione are frequent. The hyperinsulinaemia and hyperandrogenaemia stimulate epithelial proliferation and melanin accumulation ensuing within the cutaneous changes seen. The syndrome is assessed into idiopathic, ovarian, adrenal and hyperprolactinaemic types. All four main medical indicators are only current in about 20% of cases, seborrhoea is a consistent discovering and acne is clear in round 10% of cases [100]. Skin issues embody pathergy, with abscesses growing on the websites of injections; severe nodulocystic zits appears in adolescence adopted by recurrent sterile ulcers often identified as pyoderma gangrenosum [103]. Systemic or domestically administered glucocoticosteroids are usually useful for the inflammatory signs. Apert syndrome Apert syndrome, also known as acrocephalosyndactyly, was first described in 1906 [105]. The prevalence is estimated at 15/1000 000 births based on a current populationbased research [106]. Apert syndrome is characterised by craniosynostosis and early epiphyseal closure which outcomes in deformities of the skull, hands and ft. The attribute facial abnormalities are hypertelorism, a flattened occiput, proptosis as a end result of shallow orbits, prognathism, a parrotbeaked nose and fused shortened digits. Severely delayed tooth eruption, shovelshaped incisors and malocclusion of teeth occurs. Abnormalities of the higher and lower respiratory tracts embody cleft soft palate and bifid uvula [107]. Moderate to severe pimples which generally presents early in puberty is a attribute characteristic of Apert syndrome [108�110]. No distinction within the androgen receptor expression has been demonstrated suggesting that the underlying downside in Apert syndrome relates to irregular sensitivity to normal circulating ranges of androgens [112�114].
Black-Berried Alder (Elderberry). Estrace.
- What other names is Elderberry known by?
- Are there safety concerns?
- "The flu," also called influenza.
- Are there any interactions with medications?
- How does Elderberry work?
- Cancer, constipation, nerve pain, chronic fatigue syndrome (CFS), hayfever, HIV/AIDS, and other conditions.
- Dosing considerations for Elderberry.
- What is Elderberry?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96444
1 mg estrace order overnight delivery
Numerous complicated interactions happen menstruation every two weeks cheap estrace 2 mg on line, involving von Willebrand factor and its glycoprotein receptor womanlog pregnancy estrace 2 mg purchase with visa, numerous integrin adhesion molecules, thrombospondin, fibronectin, laminin, phospholipases and adenosine diphosphate released from broken cells, in addition to collagen and platelets. Platelet activation causes the release of serotonin and thromboxane A2, each of which trigger vasoconstriction, and enhance platelet adhesiveness and aggregation leading to the formation of a platelet plug. This process is aided further by the presence of plasma fibrinogen and by thrombin. The production of prostacyclin, a powerful vasodilator and inhibitor of platelet aggregation, is decreased because of endothelial injury. Developing platelet plugs are strengthened by fibrin strands formed on account of activation of the plasma clotting system by platelet issue 3, when this is uncovered by alterations within the surface characteristics of the aggregated platelets. Purpura as a outcome of platelet defects can be divided into three teams, the second and third of that are discussed on this chapter: � Thrombocytopenia, i. Abnormalities of platelet perform Several haemorrhagic syndromes have become recognized during which platelet function is abnormal, although the whole depend may be regular [1,2�4,5,6]. These may be inherited, idiopathic or secondary to medicine or many other diseases, including thrombopathia, thrombasthenia, von Willebrand disease, severe anaemia, continual renal failure and fibrinogen defects. Hermansky�Pudlak syndrome consists of a bleeding diathesis due to storage pool disorder, with oculocutaneous albinism and pigmentcontaining cells within the bone marrow. Laboratory testing of platelet perform is of limited direct relevance to dermatologists [6]. Natural and natural treatment agents that may trigger platelet dysfunction embrace fish oil, garlic, cumin, turmeric, Gingko biloba and black tree fungus [5]. May�Hegglin abnormality) � granule issues � Dense granule (granule) disorders (Hermansky�Pudlak syndrome, Chediak�Higashi syndrome, storage pool disease) � Abnormalities of signal transduction pathways � Membrane phospholipids abnormalities. This may lead to an inclination to platelet plugging and thrombosis or, paradoxically, to a bleeding tendency (particularly when the platelet count exceeds 1000 � 109/L with a clonal platelet defect similar to an acquired type of storage pool disease). Dermatological manifestations and associations of thrombocythaemia include purpura with or without necrosis, livedo reticularis, acrocyanosis, purple (blue) toe syndrome, Raynaud phenomenon, erythromelalgia, different vascular signs together with gangrene, and related problems corresponding to pyoderma gangrenosum [1,2�6,7]. Many of those shows are also seen in other hyperviscosity and dysproteinaemic conditions. It is more frequent in females, linked with greater imply platelet volume and better fibrinogen ranges, and is partly genetically determined. Gravity and venous stasis are crucial causes of pupura due to raised intravascular pressure, though it could additionally occur at the aspect of different dermatoses. Many eruptions on the decrease leg, particularly within the elderly, are inclined to Abnormal or decreased assist of blood vessels one hundred and one. Rapid development of lower leg oedema may trigger an eczematous eruption in which purpura could also be distinguished [1]. Acroangiodermatitis (of Mali, or pseudo Kaposi sarcoma) may mimic a pigmented purpuric dermatosis, however is discussed here because the purpura is due to abnormal vasculature other than to capillaritis. There are a number of reports of it occurring as a stump dermatosis in amputees [2], and it has been reported in a patient with a thrombophilic prothrombin mutation [3]. The lesions of acroangiodermatitis happen particularly on the lower legs but could prolong onto the dorsa of the ft and toes, and up the leg, particularly over dilated varicosities. Individual lesions are minute purpuric macules that coalesce to form irregular plaques, which may be several centimetres in diameter. Oedema, sclerosis, ulceration and different indicators of venous insufficiency could additionally be associated, but could additionally be totally absent even in instances of long duration. Differential analysis includes strange gravitational dermatitis, Schamberg disease and Kaposi sarcoma. Treatment for acroangiodermatitis is unsatisfactory but assist hosiery appears logical. The typical presentation of exerciseinduced purpura is with purpuric lesions, which can be urticarial, on the lower legs after prolonged walking (many descriptions are in golfers, marathon runners or longdistance walkers), often in hot weather. Patients are normally middle aged; nonetheless it has also been described in a baby with recurrent purpura on the trunk after vigorous exercise [6]. This situation is distinct from actinic purpura, which is a manifestation of cumulative sunlightinduced ageing of the pores and skin. Some view it as a variant of polymorphic gentle eruption or arising from photo voltaic capillaritis [7,8]. Parent conditions such as Ehlers�Danlos syndrome (collagen), pseudoxanthoma elasticum (elastic) and amyloidosis (abnormal protein) are discussed in more element elsewhere. Along with corticosteroid purpura, actinic (also known as Bateman pupura or senile pupura) and corticosteroid purpura are the most typical patterns of purpura because of lack of assist in blood vessels [1,2]. It occurs mostly in pores and skin altered by both age and solar radiation, however might occur in premature ageing syndromes. Damage to the connective tissue of the dermis induced by sun exposure presents as purpuric macules on the forearms, palms, face and neck. Corticosteroid purpura has the identical sample whether because of topical, oral, endogenous (Cushing syndrome) and even inhaled corticosteroids [4]. The purpura happens mainly in atrophic pores and skin on exposed components of the palms and forearms, or on the legs. They are normally asymptomatic and differ in dimension from a couple of millimetres to a quantity of centimetres throughout. Type of disorder Inherited defects affecting structural parts of the dermis and/or vascular wall Acquired defects affecting structural parts of the dermis and/or vascular wall Haemangiomatous disorders Clotting issue and associated inherited or acquired deficiencies Nonthrombocytopenic platelet abnormalities Biochemical (congenital or acquired) Examples Ehlers�Danlos syndromea Marfan syndromea Osteogenesis imperfecta Pseudoxanthoma elasticum Deposition problems, Also known as Achenbach syndrome, paroxysmal finger haematoma might be more widespread than the variety of reported circumstances would suggest [5]. Its importance is that it could be confused with Raynaud phenomenon or acute connective tissue illnesses and investigated unnecessarily [6]. In paroxysmal finger haematoma there are recurrent episodes of painful bruising on the palms and palmar elements of the fingers. It appears probably that the syndrome represents venous rupture, due to frictional trauma. In scurvy, altered collagenous help for the blood vessels is manifest by both petechiae, especially on the legs, or by small or giant bruises on the limbs following gentle or inapparent trauma [7]. Bizarre patterns of purpura could additionally be attributable to suction, for example vacuum extractors within the neonate, electrocardiogram leads or across the mouth after sucking out the air from a glass [1]. Cultural cures corresponding to cupping, coin rubbing (Cao Gio) and spooning (Quat sha) can also produce unusual patterns of purpura which are usually clearly extrinsic in causation. Black heel (talon noire) is a type of purpura because of frictional shearing of vessels. It is pigmentation of the heel (or palm) secondary to extravasation of red blood cells [2]. Infection Increased pressure inside vessels Physical Drugs Others Epidemiology Incidence and prevalence Either intercourse could additionally be affected by black heel, however the condition is virtually confined to athletic adolescents. The appearance of the lesions is characteristic, with irregular areas, often not palpable, that present little inflammatory reaction and which are normally darkish purple quite than having the sequential colour adjustments of a standard bruise. Pathophysiology Pathology In black heel, extravasated erythrocytes may be discovered in the dermal papillae [1], however usually the histological modifications are restricted to Dysproteinaemic and Waldenstr�m hypergammaglobulinaemic purpura 101. Clinical options History the situation of black heel results from shear�stress rupture of the papillary capillaries, for example throughout violent sport, significantly the place repeated leaping and sudden stopping or twisting of the heel occurs.
Purchase 2 mg estrace visa
The syndrome is brought on by mutations within the Sonic Hedgehog patched gene women's health clinic erina best 1 mg estrace, a tumour suppressor gene [5] women's health boutique houston tx estrace 2 mg discount without prescription. A single level mutation in one patched allele could also be liable for the varied malformations found in the syndrome [5�10]. Inactivation of each patched alleles results in the formation of tumours and cysts (basal cell carcinomas, odontogenic keratocysts and medulloblastomas) [5]. There are additionally occasional reviews of oral neoplasms, notably fibrosarcoma, ameloblastoma, squamous carcinoma, basal cell carcinoma and Bcell lymphoma [6�15]. Jacob illness Jacob illness is a uncommon condition consisting of recent joint formation between the coronoid process of the mandible and the inside aspect of the zygomatic arch [1,2]. Kindler syndrome Kindler syndrome (Weary�Kindler syndrome) is characterized by bulla formation, which starts at start on areas of the skin that receive pressure and will lead to bilateral incomplete syndactylies involving all web spaces [1�3]. Oral lesions might embody atrophy of the buccal mucosa, white patches on the gingiva and oral mucosa show, trismus (an inability to absolutely open the mouth), aggressive periodontitis and a type of desquamative gingivitis [4,5]. Histology shows classical options of poikiloderma, specifically epidermal atrophy with flattening of the rete ridges, vacuolization of basal keratinocytes, pigmentary incontinence and mild dermal perivascularization. Ultrastructural studies show reduplication of the basal lamina with branching buildings throughout the higher dermis and cleavage between the lamina densa and the cell membrane of the keratinocytes. Noonan syndrome Synonyms and inclusions � Ullrich�Turner syndrome Lip pits and sinuses Congenital lip pits or sinuses are small blind fistulae on the vermilion border [1�5]. They are usually bilateral and symmetrical, usually just to one aspect of the philtrum. They might talk with Ullrich�Turner syndrome is attributable to monosomy X or a structural abnormality of the second X chromosome. It is seen in females with a syndrome of short stature, sexual infantilism and a pattern of attribute minor anomalies together with pterygium colli. This syndrome was later referred to as Noonan syndrome, and it was proven that central large cell lesions or cherubism of the jaws may be present [1�9]. This autosomal dominant syndrome has a frequency of 1/75 000 to 1/100 000 in white populations. Their incidence is 1�20% in numerous population groups [13]; for instance, in a single sequence they have been found in 12% of white individuals and 20% of black folks [14]. Rarely, they could be contaminated and current as recurrent or refractory angular cheilitis. Oral retinoids similar to etretinate or isotretinoin may be of prophylactic value [4�6]. Topical 5fluorouracil or surgical procedure could also be used to treat doubtlessly malignant lesions. Oral manifestations in tuberous sclerosis include pitshaped enamel defects in both dentitions, and gingival fibromatosis [1�7] and rare situations of myxoma or desmoplastic fibroma [8,9]. It is the most common syndromic type of cleft lip and palate, and in Van der Woude syndrome decrease lip pits are related to cleft lip and/or palate [2�5,6,7]. There is phenotypic and genotypic overlap between Van der Woude syndrome and isolated cleft of the lip and/or palate. Van der Woude syndrome is usually seen with syndactyly or talipes equinovarus, or cognitive dysfunction [8]. Blisters, erosions and ulcers Blisters could additionally be of native cause similar to a burn, because of mucocoeles, or related to infections or vesiculobullous illness. Vesicles/ blisters quickly break down within the mouth as a end result of trauma, moisture and infection to depart eosions or ulcers. About twothirds of patients have intraoral neurofibromas affecting predominantly the tongue, lips, buccal mucosa or palate. Neurofibroma represents a benign overgrowth of all parts of a peripheral nerve (axon cylinder, Schwann cells and fibrous connective tissue), organized in quite so much of patterns. About 60% of sufferers have radiographic evidence of illness, particularly enlargement of the inferior alveolar canal or foramen, or branching of the canal. Other rare, malignant tumours embrace nerve sheath tumour [18], triton tumour [19] and Merkel cell carcinoma [20]. Accidental cheek biting or facial trauma might trigger ulceration in any individual; the history is often fairly clear and a single ulcer of quick period (5�10 days) is present. Ulceration as a outcome of biting an anaesthetized lower lip or tongue following a dental local analgesic injection is a reasonably widespread problem in young kids. Orthodontic appliances or, more generally, dentures (especially if new) are answerable for many traumatic oral ulcers. These ulcers are normally clearly related to the appliance and have been a problem within the care of cleft palate patients [1]. The chance of some other aetiology for ulcers of apparently native trigger should all the time be borne in thoughts. Riga�Fede illness consists of ulcers of the lingual frenum in neonates with natal lower incisors [3]. Selfmutilation may be seen in some psychologically disturbed sufferers [4,5], sufferers with learning incapacity, people with sensory impairment and in Lesch�Nyhan syndrome [6�11]. Oral purpura or ulceration may be seen on the lingual fraenum or palate due to cunnilingus or fellatio, respectively [12]. Other local causes of ulceration embrace thermal burns, especially of the tongue and palate. Most ulcers of native cause heal spontaneously inside 7�14 days if the cause is removed. Any patient with a single ulcer lasting more than 2�3 weeks ought to be regarded with suspicion and investigated further, usually by biopsy � it might be a neoplasm or different serious dysfunction [15]. Pathophysiology Predisposing factors the aetiology of the disease that impacts older adults or kids stays obscure and could also be related to traumatic elements. Clinical options Eosinophilic ulcer of the oral mucosa, additionally known as traumatic eosinophilic granuloma or Rida�Fede disease (see above), is an uncommon, benign and selflimited lesion which generally affects the tongue, the lateral or dorsal surface. Recurrent aphthous stomatitis Definition and nomenclature Recurrent aphthous stomatitis is characterized by recurring episodes of ulcers, usually from childhood or adolescence, each lasting from 1 to about four weeks earlier than healing. Synonyms and inclusions � Aphthae � Canker sores Eosinophilic ulcer of the oral mucosa [1�7,eight,9] Definition and nomenclature A benign and selflimited lesion which usually affects the tongue. Incidence and prevalence Recurrent aphthous stomatitis is a common disease that probably afflicts no much less than 20% of the population. The serum immunoglobulin ranges are normally regular, although IgA and IgG could additionally be elevated, and immune complexes could also be discovered. Cellmediated immune mechanisms appear to be involved within the pathogenesis of recurrent aphthous stomatitis. In the lesions, helper T cells predominate early on, with some natural killer cells.
Cheap 2 mg estrace
This intensely uncomfortable burning related to paroxysmal erythema of the distal extremities is frequently triggered by pores and skin contact with a warm floor women's health new dimensions generic estrace 1 mg with mastercard. Although erythromelalgia has been seen in many various settings women's health issues periods estrace 2 mg discount on-line, the association of purpuric or necrotic areas on the arms and ft with dysaesthetic erythema is completely seen with myeloproliferative or myelodysplastic thrombocytosis [10]. Anaemia and altered red cell morphology can happen over time in all patients, and all these diseases have some danger of transition to dyspoiesis and extreme anaemia, leukaemia or myelofibrosis. Cryofibrinogen deposits consist of a fancy of fibrinogen, fibrin and fibronectin that forms on cold exposure [5]. Cold agglutinins are immunoglobulins that are in a position to agglutinate purple blood cells under regular physique temperatures. Although the precipitation of cryoglobulins is primarily related to reversible coldinduced denaturation of protein, different elements corresponding to cryoglobulin concentration in the microvascular environment, pH and noncovalent binding factors additionally influence the likelihood and intensity of precipitation. Epidemiology Other syndromes are also associated with cryoglobulins detectable in serum. Chronic inflammatory disease, corresponding to liver cirrhosis from any cause, can also be related to a higher than expected rate of detectable cryoglobulins. Cryofibrinogenaemia may be idiopathic or may be related to malignant problems (especially haematological), thromboembolic illness, IgA nephropathy or varied inflammatory, connective tissue or infectious syndromes [8,9]. Monoclonal chilly agglutinins are idiopathic or secondary to malignant lymphoproliferative diseases. Cryofibrinogens and chilly agglutinins are hardly ever the purpose for occlusive syndromes triggered by cold exposure, regardless of being usually detected in sufferers with varied diseases [6]. Age the median age at diagnosis of cryoglobulinaemia is the early to center sixth decade. Pathology Sex Cryoglobulinaemia incidence has a female to male ratio of 2: 1 [2]. Type I cryoglobulins are single monoclonal immunoglobulins, often IgG or IgM, less generally IgA, and rarely Bence�Jones protein. Those that bind immunoglobulin (usually IgG) by antiFc affinity are also, by definition, rheumatoid components, although solely the IgM/antiIgG rheumatoid elements are recognized by standard rheumatoid factor testing. Acquired dysfibrinogenaemia may not often mimic a cryofibrinogen syndrome by acral occlusion, together with gangrene. Interestingly, this subset of dysfibrinogenaemia seems to act by significantly increasing purple cell aggregation, mimicking occlusioninducing cold agglutinins. In circumstances of chilly agglutininrelated cutaneous occlusion, the agglutination of pink blood cells depends on binding of antibody to a couple of cell at a time. Just as with cryoglobulins, there Associated diseases Type I cryoglobulins are sometimes related to an underlying lymphoproliferative disorder, particularly a quantity of myeloma or Waldenstr�m macroglobulinaemia [5]. Rheumatoid issue exercise (defined by antiFc binding) is detectable within the sera of 87�100% of patients with blended cryoglobulinaemia [3]. Clinical features History the affected person will have undergone publicity to chilly temperatures. Presentation Occlusion syndromes triggered by chilly exposure are instructed by an acral distribution of lesions of necrosis or purpura, often with retiform features, and sometimes associated with acral livedo reticularis. An acral distribution have to be distinguished from a dependent distribution of lesions. Both patterns might contain palms and ft, but with a dependent pattern there are typically many more lesions on the feet and legs than on the arms. Ulceration, haemorrhagic crusts or cutaneous infarction are seen in 10�25% of patients, most often with kind I cryoglobulins. Coldinduced acrocyanosis of acral areas, and non inflammatory retiform purpura are also more typical of sort I cryoglobulinaemia. Other reported cutaneous findings embrace acral cyanosis, Raynaud phenomenon, urticarial lesions, ulceration and livedo reticularis [4,12]. Noncutaneous medical findings most frequently include involvement of the joints, peripheral nerves, kidneys and liver [2,3,4]. The foot lesion exhibits minimal erythema, retiform bullae and haemorrhage with necrosis. Distal occlusion syndromes (cholesterol emboli, acral antiphospholipid antibody syndrome) can also current similarly, however lack a historical past of chilly exposure and the presence of lesions on the nose and ears. Complications and comorbidities There are solely two known methods in which cryoglobulins may end up in illness. The first is by precipitation inside the vascular lumen, usually cold induced, with hyaline plug formation and minor earlyphase irritation. Typical medical lesions are characterised by minimally inflammatory cutaneous infarction, with or without related livedo reticularis, or noninflammatory retiform purpura. If they cryoprecipitate close to Differential analysis A dependent distribution of lesions suggests immune complex mediated disease, and often presents as basic palpable purpura or sometimes as inflammatory retiform purpura, not as bland or noninflammatory purpura or paucierythematous necrosis. Chilbains should be thought-about, although these lesions develop slowly and infrequently have acute purpura or necrosis [6]. Cryofibrinogenaemia is widespread as a laboratory abnormality however is a uncommon reason for symptomatic scientific illness [15]. Just as with many cryoglobulins and most cryofibrinogens, cold agglutinins are more than likely to be asymptomatic. When answerable for illness, reversible acrocyanosis secondary to coldinduced acral agglutination is most common. Livedo reticularis, Raynaud phenomenon, chilly urticaria and infrequently cutaneous necrosis could occur. In addition to acral lesions on environmental chilly publicity, chilly intravenous infusions can also set off localized cutaneous necrosis [16]. Cold agglutinins can induce complement activation after coldinduced binding to purple blood cells, followed by lysis and haemolytic anaemia, unbiased of occlusive syndromes from agglutination. Investigations A biopsy of early lesions, before necrosis has had time to trigger a secondary vasculitic histology, ought to show noninflammatory occlusion of dermal vessels with cryoprotein or agglutinated purple cells. Careful handling of serum and plasma is critical to allow the identification of cryogelling proteins, as a outcome of these most likely to trigger illness are those that gel at temperatures very close to normal body temperature. A more sensitive technique, such as immunofixation, is required to identify the presence of a clonal protein. Histological demonstration of noninflammatory hyaline thrombosis is more widespread in sufferers with kind I cryoglobulinaemia, but some such sufferers have additionally been reported to have cutaneous vasculitis [11]. Since cryofibrinogens could be cleaved to kind fibrin, plasma somewhat than serum must be tested to detect these cryogelling proteins. Biopsy specimens from skin lesions typically present thrombi in small vessels with dermal necrosis [8]. Leukocytoclastic vasculitis has been reported, however is probably because of ischaemic necrosis rather than being a cause [9]. Fibronectin may be a major component of vascular plugs in patients with cryofibrinogenaemia alone, whereas vascular occlusion in sufferers with both cryofibrinogens and cryoglobulins exhibits a predominance of cryoglobulin deposition [9].