Geodon
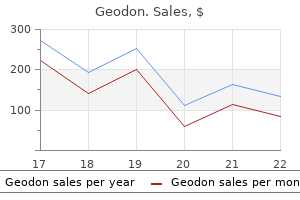
Geodon dosages: 80 mg, 40 mg, 20 mg
Geodon packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 360 pills

Order 20mg geodon
Neurons communicate with each other at synapses bipolar depression recurrence buy 40 mg geodon with amex, points of contact between neurons depression test health canada purchase geodon 20 mg with amex. The communication occurs via neurotransmitters, chemical agents launched or secreted by one neuron, which can excite or inhibit another neuron, continuing or terminating the relay of impulses or the response to them. Clinical Box Lymphangitis, Lymphadenitis, and Lymphedema the phrases lymphangitis and lymphadenitis discuss with the secondary inflammation of lymphatic vessels and lymph nodes, respectively. These pathological processes may occur when the lymphatic system is involved within the metastasis (spread) of cancer-the lymphogenous dissemination of cancer cells. For occasion, if cancerous lymph nodes are surgically removed from the axilla (armpit), lymphedema of the upper limb might outcome. The nerve cell our bodies lie inside and represent the grey matter; the interconnecting fiber tract techniques type the white matter. The struts (supports) of the H are horns; due to this fact, there are right and left posterior (dorsal) and anterior (ventral) gray horns. The mind and spinal twine are intimately lined on their outer floor by the innermost meningeal layer, a delicate, transparent masking, the pia mater (pia). External to the pia and arachnoid is the thick, tough dura mater (dura), which is intimately related to the internal side of the bone of the surrounding neurocranium (braincase). The dura of the spinal wire is separated from the vertebral column by a fat-filled house, the epidural house. Their proximal stumps begin to regenerate, sending sprouts into the world of the lesion; nonetheless, progress is blocked by astrocyte (a type of glial cell) proliferation on the web site of injury. A nerve fiber consists of an axon, the single process of a neuron; its neurolemma, the cell membranes of Schwann cells that instantly surround the axon, separating it from different axons; and its endoneurium, a connective tissue sheath. The neurolemma of myelinated nerve fibers have a myelin sheath that consists of a continuous series of Schwann cells enwrapping an individual axon, forming myelin. The neurolemma of unmyelinated nerve fibers encompass a number of axons individually embedded inside the cytoplasm of each Schwann cell. Most fibers in cutaneous nerves (nerves that provide sensation to the skin) are unmyelinated. Endoneurium, a fragile connective tissue sheath that surrounds the neurolemma cells and axons 2. Perineurium, a layer of dense connective tissue that encloses a fascicle (bundle) of peripheral nerve fibers, providing an effective barrier against penetration of the nerve fibers by international substances three. Epineurium, a thick connective tissue sheath that surrounds and encloses a bundle of fascicles, forming the outermost masking of the nerve; it contains fatty tissues, blood vessels, and lymphatics A peripheral nerve is very like a telephone cable: the axons are the person wires insulated by the neurolemma and endoneurium, the insulated wires are bundled by the perineurium, and the bundles are surrounded in turn by the epineurium, forming the outer wrapping of the "cable. Skeletal muscle Skin myotome: dermatome: Spinal nerve Clinical Box Peripheral Nerve Degeneration When peripheral nerves are crushed or severed, their axons degenerate distal to the lesion as a end result of they rely upon their cell bodies for survival. A crushing nerve harm damages or kills the axons distal to the injury site; nevertheless, the nerve cell bodies normally survive and the connective tissue coverings of the nerve are intact. No surgical restore is needed for this kind of nerve damage because the intact connective tissue sheaths guide the growing axons to their locations. Surgical intervention is critical if the nerve is cut as a outcome of the regeneration of axons requires apposition of the cut ends by sutures by way of the epineurium. The particular person fascicles (bundles of nerve fibers) are realigned as accurately as potential. Prolonged ischemia of a nerve might lead to harm no much less extreme than that produced by crushing and even slicing the nerve. The somatic motor fibers stimulate skeletal (voluntary) muscle exclusively, evoking voluntary and reflexive motion by inflicting its contraction. Schematic representation of a dermatome (the unilateral space of skin) and a myotome (the unilateral portion of skeletal muscle) receiving innervation from a single spinal nerve. This map is predicated on the studies of Foerster (1933) and reflects each anatomical (actual) distribution or segmental innervation and medical expertise. The posterior root carries general sensory fibers to the posterior horn of the spinal cord. The anterior and posterior roots unite at the intervertebral foramen to type a spinal nerve, which instantly divides into two rami (branches): a posterior ramus and an anterior ramus. As branches of a combined spinal nerve, the anterior and posterior rami also carry each motor and sensory nerves, as do all their branches. Proprioceptive sensations are unconscious sensations that convey info on joint place and the tension of tendons and muscular tissues, offering information on how the body and limbs are oriented in house, unbiased of visible input. Clinicians need to understand the dermatomal innervation of the skin so they can determine, utilizing sensory testing. Each skeletal muscle is often innervated by the somatic motor fibers of several spinal nerves; due to this fact, the muscle myotome will consist of several segments. Causes ejaculation and vasoconstriction, leading to remission of erection Release of adrenaline into blood Effect of Sympathetic Stimulation Dilates pupil (admits more mild for elevated acuity at a distance) Effect of Parasympathetic Stimulation Constricts pupil (protects pupil from excessively bright light) Contracts ciliary muscle, permitting lens to thicken for close to vision (accommodation) No impact (does not reach)a No effect (does not reach)a No impact (does not reach)a Promotes secretion Promotes ample, watery secretion Decreases fee and strength of contraction (conserving energy); constricts coronary vessels in relation to reduced demand Constricts bronchi (conserving energy) and promotes bronchial secretion Stimulates peristalsis and secretion of digestive juices; contracts rectum and inhibits internal anal sphincter to trigger defecation Promotes building/conservation of glycogen; will increase secretion of bile Inhibits contraction of internal sphincter of bladder, contracts detrusor muscle of bladder wall, causing urination Produces engorgement (erection) of erectile tissues of exterior genitals No impact (does not innervate) Lungs Digestive tract Liver and gallbladder Urinary tract Genital system Suprarenal medulla a the parasympathetic system is restricted in its distribution to the head, neck, and body cavities (except for erectile tissues of genitalia); otherwise, parasympathetic fibers are by no means discovered within the body wall and limbs. Sympathetic fibers, by comparability, are distributed to all vascularized portions of the physique. With the exception of the coronary arteries, vasoconstriction is sympathetically stimulated; the effects of sympathetic stimulation on glands (other than sweat glands) are the oblique results of vasoconstriction. In general, the results of sympathetic stimulation are catabolic (preparing the physique for "flight or struggle"). In basic, the results of parasympathetic stimulation are anabolic (promoting normal function and conserving energy). A practical distinction of pharmacological significance in medical practice is that the postsynaptic neurons of the 2 techniques generally liberate totally different neurotransmitter substances: norepinephrine by the sympathetic division (except in the case of sweat glands) and acetylcholine by the parasympathetic division. The superior paravertebral ganglion-the superior cervical ganglion of every sympathetic trunk-lies at the base of the cranium. The ganglion impar varieties inferiorly, where the 2 trunks unite on the stage of the coccyx. Pass through sympathetic trunk with out synapsing to enter an abdominopelvic splanchnic nerve for innervation of abdominopelvic viscera solely T5 Viscera of abdominopelvic cavity. Almost instantly after getting into the rami, all of the presynaptic sympathetic fibers depart the anterior rami of these spinal nerves and cross to the sympathetic trunks through white rami communicantes. Presynaptic sympathetic fibers innervating viscera throughout the abdominopelvic cavity observe the fourth course. By this means, they enter all branches of all 31 pairs of spinal nerves, together with the posterior rami, to stimulate contraction of blood vessels (vasomotion) and the arrector muscles of hair (pilomotion, resulting in goose bumps) and to cause sweating (sudomotion). Postsynaptic sympathetic fibers that carry out these features within the head (plus innervation of the dilator muscle of the iris) all have their cell bodies within the superior cervical ganglion at the superior end of the sympathetic trunk. The presynaptic sympathetic fibers concerned in innervation of viscera of the abdominopelvic cavity. All presynaptic sympathetic fibers of the abdominopelvic splanchnic nerves, besides those involved in innervating the suprarenal (adrenal) glands, synapse within the prevertebral ganglia.
CO Q10 (Coenzyme Q-10). Geodon.
- Improving the immune system of people with HIV/AIDS.
- What is Coenzyme Q-10?
- Coenzyme Q-10 deficiency (very rare).
- Decreasing the risk of additional heart problems in people who have had a recent heart attack (myocardial infarction).
- Congestive heart failure (CHF), in combination with other medications.
- Coenzyme Q-10 Dosing »
- Dosing considerations for Coenzyme Q-10.
- Improving exercise performance.Dental (periodontal) disease, when applied directly to the teeth and gums.
- You are pregnant or breast-feeding.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96901
Order geodon 40mg online
This allows them to take advantage of their regular physique reflexes depression during period discount 40 mg geodon otc, somewhat than having to pressure to defecate mood disorder treatment plan buy generic geodon 20 mg online. Although these methods can be used alone, extra evidence exists for the usage of biofeedback strategies to help with defecation issues associated with pelvic flooring muscle rest issues, also referred to as dyssynergic defecation. The chief underlying pathophysiologic mechanism of dyssynergic defecation is a failure of rectoanal coordination and may happen concurrently with slow-transit constipation. Evidence from randomized managed trials means that biofeedback may be successful for the treatment of dyssynergic Combining Behavioral and Drug Therapy Some clinicians combine behavioral and drug treatments primarily based on the premise that suppressing detrusor overactivity with a medication makes it easier for the patient to achieve volitional control. Others consider that medicine are useful, however their effectiveness is significantly improved with the addition of behavioral remedies. One managed research examined the effects of bladder training with and with out antimuscarinic medication. In a second study, prompted voiding was mixed with oxybutynin or a placebo in functionally impaired nursing residence sufferers with detrusor instability. Subjects who initially received drug remedy additionally showed extra improvement with combined remedy (P =. Two newer studies examined combining behavioral and drug therapy in preliminary therapy. One examine in contrast the effects of mixed therapy with drug remedy alone for urgency incontinence in women. The other study investigated whether or not combining therapies would enable women with urgency-predominant incontinence to discontinue drug therapy and preserve a clinically significant reduction in incontinence episodes. Three hundred and 7 girls with urgency-predominant incontinence have been randomized to drug remedy with extendedrelease tolterodine with or without behavioral remedy. Women who underwent behavioral training along with drug therapy were no more prone to discontinue drug remedy and sustain improvements in continence standing than women handled with drug alone. However, ladies who obtained mixed therapy reported larger enhancements on affected person notion of enchancment, affected person satisfaction, and validated measures of symptom misery and bother while on lively therapy and 6 months after drug therapy was discontinued. Another massive multicenter, uncontrolled trial examined the effects of extended-release tolterodine plus a self-administered behavioral intervention (educational pamphlet with verbal reinforcement) in sufferers who have been previously treated and dissatisfied with tolterodine or other antimuscarinics. Thus, combined remedy resulted in high remedy satisfaction and improved urinary symptoms in sufferers who were previously handled and dissatisfied with antimuscarinic remedy. Less research has been done combining behavioral and drug therapies for stress incontinence. A single examine in contrast duloxetine alone, pelvic ground muscle coaching alone, combined duloxetine and pelvic floor muscle training, and placebo. As in the case of urgency incontinence, combining treatments for stress incontinence is thought to enhance outcomes as a result of the different modes of motion of behavioral and drug therapies. Some clinicians have advocated utilizing electrical stimulation to facilitate training by serving to patients better establish and strengthen their muscles. Two studies have examined whether or not including electrical stimulation might lead to higher outcomes with pelvic floor muscle training. One research explored whether combining training with home-based, lowintensity electrical stimulation or clinic-based maximal intensity electrical stimulation would yield higher outcomes than pelvic floor muscle training alone. Another trial examined whether or not including daily residence electrical stimulation would improve the effectiveness of biofeedback-assisted behavioral coaching for stress incontinence. Combining Behavioral Treatments and Medications for Fecal Incontinence Although recommendation on diet and stool consistency is often part of biofeedback trials, just one trial studied the independent impact of an academic intervention compared with biofeedback and pelvic ground muscles workouts. In distinction, 168 women and men with extreme fecal incontinence defined as no much less than one teaspoon of stool a minimum of as quickly as per week were first treated with medical management (loperamide and/or fiber supplementation) to enhance stool consistency and education on healthy bowel habits for 4 weeks. After three months, 76% of the biofeedback handled patients reported adequate relief compared with 41% of the pelvic floor muscle train only group in an intention-to-treat analysis. This examine confirmed a major advantage of pelvic flooring muscle workout routines over schooling and medical administration, but biofeedback was more practical. The few studies of long-term outcomes are inconsistent, however promising in that many patients are capable of sustain enhancements in bladder management over time. They have been used for decades to deal with urinary and fecal incontinence, different decrease urinary tract symptoms, and defecatory dysfunction in girls of all ages. They may be carried out by advanced practice nurses, physical therapists, physicians, or different suppliers in outpatient practice. Behavioral remedies are secure and reversible, making them acceptable as first-line therapies for urinary and fecal incontinence and other pelvic floor dysfunction in ladies. Therefore, the greatest challenge for the clinician becomes tips on how to inspire sufferers to be actively concerned of their care, to observe their day by day program consistently, and to persist for long sufficient to expertise significant change of their signs. Progress in behavioral packages is often gradual that makes compliance even more troublesome for sufferers who anticipate quick results. Clinically, we will optimize patient adherence by making it clear that progress will be gradual and that it might be irregular, with "good" days and "unhealthy" days. We can encourage participation by communicating that improvement will rely largely on constant practice and use of new skills. Most research provide little details about how adherent patients are with pelvic flooring muscle train, behavioral strategies, voiding schedules, or different parts of behavioral treatment. Efficacy of pelvic flooring muscle workouts in girls with stress, urge, and mixed urinary incontinence. Comparative efficacy of behavioral interventions in the management of female urinary incontinence. The effect of behavioral therapy on urinary incontinence: a randomized managed trial. Predictors of end result in the behavioral remedy of urinary incontinence in girls. Long-term efficacy of nonsurgical urinary incontinence therapy in aged girls. Interdisciplinary approach to the assessment and behavioral remedy of urinary incontinence in geriatric outpatients. Effects of pelvic flooring muscle training on strength and predictors of response in the remedy of urinary incontinence. Reliability assessment of the bladder diary for urinary incontinence in older women. Progressive resistance train within the practical restoration of the perineal muscle tissue. Behavioral training with and without biofeedback within the treatment of urgency incontinence in older girls: a randomized managed trial. Randomized managed trial exhibits biofeedback to be superior to pelvic flooring muscle exercises for fecal incontinence. A randomized-controlled trial evaluating an academic intervention alone versus schooling and biofeedback within the administration of faecal incontinence in ladies. Randomized, controlled trial of biofeedback with anal manometry, transanal ultrasound, or pelvic floor retraining with digital guidance alone within the remedy of gentle to average fecal incontinence. A comparability of effectiveness of biofeedback and pelvic muscle exercise therapy of stress incontinence in older community-dwelling ladies. Urinary incontinence in the aged: bladder-sphincter biofeedback and toileting abilities training. The function of biofeedback in Kegel train training for stress urinary incontinence.
Discount 20mg geodon with mastercard
Bladder outlet obstruction nomogram for women with lower urinary tract symptomatology borderline depression definition generic geodon 80mg line. Efficacy of sacral nerve stimulation for urinary retention: results 18 months after implantation anxiety vs adhd 80mg geodon purchase with visa. Botulinum toxin urethral sphincter injection to restore bladder emptying in women and men with voiding dysfunction. Management of practical bladder neck obstruction in women: use of alphablockers and pediatric resectoscope for bladder neck incision. The impact of terazosin on useful bladder outlet obstruction in women: a pilot study. The position of uroflowmetry biofeedback and biofeedback coaching of the pelvic floor muscular tissues in the treatment of recurrent urinary tract infections in ladies with dysfunctional voiding: a randomized managed prospective research. The use of botulinum toxin A injection for the management of external sphincter dyssynergia in neurologically normal youngsters. Transurethral incision of the bladder neck to treat bladder neck dysfunction and voiding dysfunction in patients with high-level spinal twine accidents. Effectiveness of intravesical resiniferatoxin in treating detrusor hyper-reflexia and exterior sphincter dyssynergia in sufferers with chronic spinal twine lesions. Rehabilitation in follow: neurogenic lower urinary tract dysfunction and its administration. Effects of botulinum A toxin on detrusor-sphincter dyssynergia in spinal twine injury patients. Treatment of detrusor sphincter dyssynergia by transperineal injection of botulinum toxin. Botulinum A toxin therapy for detrusor-sphincter dyssynergia in spinal twine disease. Botulinum toxin as a new remedy option for voiding issues: current state-of-the-art. It is a socially isolating, physically and psychologically disabling condition that often has profound penalties on all elements of high quality of life. Epidemiologic data counsel that women and men are equally affected,2,four,5 which is stunning given that most research is focused on anal incontinence within the female population. Simple, low-cost interventions can often improve signs in a massive quantity of patients. For refractory sufferers, more sophisticated second-line investigations and treatments have turn out to be available in recent years. This article will evaluate the etiology, pathophysiology, and administration of anal incontinence, with explicit attention targeted on the evolving areas of our increased understanding by way of investigation and administration. Other danger elements include the impact of aging, declining estrogen help of the pelvic flooring connective tissue after menopause, or development of neuropathy and anal sphincter atrophy. Drugs Idiopathic Anal continence is maintained by a fancy integration and coordination of the operate of the pelvic ground, rectum, and anal sphincters. Understanding of the physiologic roles of every of those organs is important to find a way to perceive the mechanisms of defecation and maintaining continence. As stool enters the lower rectum, spontaneous giant rectosigmoid contractions are initiated, pushing stool through the relaxed anal canal. As the stool passes by way of the anal canal, it stretches the external anal sphincter making a traction pressure upon it. Mechanism of Defecation Defecation commences when stool is propelled into the rectum after peristaltic colonic contractions. If this phenomenon occurs in a socially applicable setting, the puborectalis and exterior anal sphincter muscular tissues loosen up, thereby straightening the anorectal angle. In order for evacuation to occur, the intra-abdominal and rectal strain should exceed that throughout the anal canal. This is achieved by performing the Valsalva maneuver or holding the breath and Central Control of Continence Defecation commences with rectal sensory consciousness at a critical level of filling, which is relayed to the cerebral cortex as the notion of the want to evacuate the rectum. Fecal urgency and urge incontinence occur in illnesses affecting the higher motor neuron pathway; nonetheless, reflex defecation will nonetheless stay potential supplied the lower motor pathway is still intact. Traction injury of the pudendal nerve secondary to persistent straining at stool or childbirth is the most typical explanation for decrease motor neuron injury. Pudendal nerve harm ends in progressive denervation of the pelvic floor-anal sphincter advanced leading to weakness and atrophy of these muscle tissue. It measures roughly 3 cm in size and three mm in thickness, being slightly longer in males and increased thickness with age. It contributes about 85% of the resting anal sphincter strain, which measures between 50 and a hundred and twenty mm Hg in health. The Rectum the rectum comprises the terminal portion of the colon and acts as a reservoir for stool. The rectum is innervated by the extrinsic autonomic nerves, which act upon the enteric nerves at submucosal plexuses, integrating together to allow rectal lodging of fecal content material, which is measurable as rectal compliance. After rectal filling sensation reaches consciousness, the parasympathetic pushed defecation reflex is initiated except voluntarily inhibited. Normal rectal perform consists of sensory perception co-ordinating fine motor management that may either store or expel luminal contents permitting for well timed defecation. The reflex is unbiased of central control, being mediated by the myenteric plexus, which is itself modulated by the autonomic nervous system. Discriminatory sensory perception allows the opportunity to distinguish solids from liquids from gasoline. This resting strain coupled with contraction of the external anal sphincter and puborectalis results in the bowel contents being returned to the rectum and sigmoid following the sampling course of. This phenomenon of compliance is the quantity response to a strain distension of the rectum and is most pronounced at decrease volumes of rectal filling representing lively rectal relaxation to accommodate fecal material. Reduced rectal compliance has been shown in sufferers with fecal urgency and incontinence, inflammatory circumstances such as colitis, pouchitis, or proctitis, fibrosing circumstances corresponding to scleroderma and as a long-term consequence of pelvic radiotherapy. The pelvic diaphragm is a striated muscular layer, with a central ligamentous structure surrounding the rectum, vagina, and urethra. It is composed of numerous muscular tissues all of which work synergistically with one another. This muscle varieties an 80� to 90� sling across the anorectal junction and inserts into the pubic bone. Voluntary contraction of the puborectalis causes closure of the anal canal or decreases in the anorectal angle. Therefore, the puborectalis can keep continence even in the absence of both inner and external anal sphincter perform. Levator ani avulsion defects happen in 15% to 35% of parous ladies delivering vaginally.
Geodon 80 mg generic without a prescription
Ultrasound Ultrasound has the benefit of being simply accessible depression brain scan order 40mg geodon otc, cost-effective depression definition psychology buy discount geodon 40mg online, and free of radiation and therefore can be used in childbearing girls. It can be utilized to delineate the contours of the kidneys and assess obstruction and bladder emptying in addition to different pelvic anatomy. The use of abdominal ultrasound is restricted in the visualization of the midportion of the urethra solely and is limited in patients of excessive physique mass index. Ultrasound is beneficial for the detection of parenchymal tumors but it has low specificity for the detection of urothelial tumors of the renal pelvis or urinary tract. Ultrasound can be used to measure postvoid residual volume which may be helpful if poor bladder emptying and a excessive residual urine are thought to underlie infection. If voiding dysfunction is suspected, a circulate price should be carried out with measurement of residual urine. Contrast injected into the accumulating system is present in the kidneys two to three minutes after injection and imaging may be carried out at totally different stages of distinction enhancement to delineate areas of low or abnormal attenuation similar to seen with damaged parenchyma. Plain Abdominal Radiograph this can be utilized to supplement ultrasound to detect stones or international bodies. If stones are current, 90% might be visualized as they contain calcium or cystine and so are radio-opaque. In mixture with ultrasound, it has been shown to be superior to an intravenous urogram and incurs much less radiation exposure. If diabetes is suspected, then a fasting glucose check or glucose toleration test should be carried out. It can be used to determine any predisposing elements for infection such as a bladder tumor or stone. Antimicrobial remedy ought to be instituted appropriately and if an underlying cause is discovered, such as obstruction, this should be handled. In these with voiding dysfunction, timed voiding or a double voiding method could also be of benefit and they want to be instructed accordingly. In circumstances of extreme infection/septicemia extra intensive supportive measures and monitoring are required. Intravenous fluids, vasoactive medication, and remedy of the septicemia should then be initiated. Antimicrobial Therapy the goal of antimicrobial therapy is to eradicate pathogenic organisms with minimal native and systemic unwanted effects. An perfect antibiotic would have a low potential to select for bacterial resistance and to give rise to unwanted effects, and be cheap and easily administered. Selection of antibiotics for empirical treatment ought to take account of local resistance patterns, which can range geographically and are also dependent on whether or not the an infection is hospital or neighborhood acquired. Side effects include anaphylaxis, skin rashes, gastrointestinal disturbances, fungal an infection, and Clostridium difficile colitis (particularly in the elderly). Local pointers want regular review to account for these changing microbial patterns. Many antibiotics administered systemically reach much higher concentrations in urine than in serum. These embody beta-lactams, aminoglycosides, fluoroquinolones, and trimethoprim, so massive doses of those brokers are rarely required. The ranges of resistance in laboratory isolates from sufferers locally may be an overestimate because of biases in the way clinicians send samples to laboratories. For instance, samples may only be sent to the laboratory when patients return to a doctor after failure of empirical treatment. Estimates of the degrees of antibiotic resistance for hospital infections may be more accurate due to the relative ease of use of the laboratory. Alternatives to amoxicillin or trimethoprim for oral use embrace nalidixic acid, penicillin/enzyme inhibitor combinations (such as amoxicillin with clavulanate), nitrofurantoin, oral cephalosporins, and quinolones. The British National Formulary is a wonderful supply of reference on antibiotic choice and remedy durations for particular scientific situations. The period of therapy has come beneath some debate with a move to shorter regimes to increase compliance and as these will have much less effect on the fecal and vaginal flora and scale back the risk of resistant strains. Additional information on use of antibiotics is offered in the part "Specific Clinical Situations. There are specific scientific situations that warrant further comment and consideration. If left untreated, 60% to 80% of sufferers will spontaneously clear an infection without long-term sequelae. In obstetric and gynecological apply these situations include pregnancy and urogenital surgical procedure. However, the optimal interval and frequency of screening after this preliminary visit is uncertain. It is the most common condition requiring hospital admission for intravenous antibiotics. In general, acute pyelonephritis resolves without long-term renal injury within the majority of women but failure in diagnosis can lead to gramnegative bacteremia, endotoxic shock, disseminated intravascular coagulation, and renal abscess formation. If chronic pyelonephritis develops, this will result in hypertension and renal failure. In the presence of obstruction, such as with stones, infection could lead to papillary necrosis, renal or perinephric abscess, or xanthogranulomatous pyelonephritis. Treatment consists of aggressive supportive remedy together with rehydration and intravascular volume growth. Drugs of alternative for parenteral therapy include cephalosporins, fluoroquinolones, or an aminoglycoside. After results of culture are available, therapy may be modified to the suitable antibiotic, if essential in consultation with a microbiologist or infectious disease doctor. Those who carry out urinary tract catheterization ought to have obtained applicable training in technique and catheter sort. Policies to limit Acute Pyelonephritis Acute pyelonephritis is an an infection of the renal parenchyma and pelvis and is assessed as uncomplicated if it is brought on by a typical pathogen in an Chapter 17 Urinary Tract Infections 309 the use of unnecessary catheterization, adoption of acceptable catheterization methods, and expediting catheter removal as soon as clinically appropriate should be practiced. The underlying reason for this is the development of a pathogenic biofilm on the surface of an indwelling catheter. The rate of bacteriuria is 3% to 10% per day and approaches 100% in those with long-term catheters. Treatment is required when the patient develops systemic signs or symptoms of infection. There is conflicting evidence on the advantage of antibiotics on the time of catheter removal or insertion. Blood-borne spread occurs from the preliminary main website, normally the lung however occasionally the gut. This type of tuberculosis tends to have an result on young adults and presents as a miliary tuberculosis or a nodular or cavitating tuberculosis affecting one kidney.
Geodon 40 mg buy free shipping
There are cases of permanent dysfunction from neurological injury/disease that can lead to impaired contractility depression zoloft not working geodon 40mg buy amex, but in addition improve resistance of the bladder outlet depression symptoms hindi 40 mg geodon discount overnight delivery. This state of affairs may end up in impaired compliance, which ends up in unsafe storage pressures and requires extra aggressive treatment (see treatment of Detrusor External Sphincter Dyssenergia section). Failure of Sphincteric Relaxation Sacral neuromodulation has been investigated as a potential remedy for Fowler Syndrome. A whole of 177 sufferers underwent a three- to seven-day percutaneous nerve analysis or check stimulation. Those that had a greater than 50% improvement in symptoms were randomized to implantation, or no implantation. The major voiding diary parameter evaluated by diary was catheterized quantity per catheterization. There was an 83% success price in those handled with implantation in comparability with a 9% success in the control group at six months. Others have looked at neuromodulation for otherwise unexplained urinary retention. Three of the sufferers developed transient stress incontinence and no patient had symptomatic profit. Prior to sphincteric injection, 19 of 21 patients (eight men and 13 women) used an indwelling or intermittent catheterization; after injection, all however 1 affected person was able to void with out catheterization. By removing the obstruction, (eg, chopping a sling or urethrolysis, uretheral diverticulectomy, urethroplasty, restore of pelvic organ prolapse, or pessary insertion), patients stand the best probability of regaining decrease urinary tract perform. It is feasible that the bladder will become decompensated from long-standing obstruction, and the new symptoms similar to frequency or urgency will persist, or the unique symptoms of stress incontinence will return. Stress incontinence was famous as a potential aspect impact of the incision of the bladder neck. The method has been described by making a single endoscopic incision or bilateral incision. A prospective study was undertaken with sufferers with dysfunctional voiding randomized to endure uroflow with biofeedback, muscle biofeedback, a mix of each, and no therapy. Here, 14 of the 16 sufferers were experiencing urgency incontinence, and, after injection of the external sphincter, 12 of the 16 patients were cured of incontinence. In extra excessive instances of sexual abuse, more invasive intervention can be profitable. Although that is much less likely to occur in ladies than in males due to general much less outlet resistance Treatment of Functional Obstruction Primary Bladder Neck Obstruction this consists of watchful ready, and therapy with pharmacotherapy, and surgical intervention. Patients with none trouble and no medical or urodynamic proof of upper or decrease urinary tract decompensation may be noticed relying on the severity and trouble of the signs. This was initially based on a research of 24 women with obstructive voiding signs or retention who had been all initially positioned on clear intermittent catheterization and -blocker remedy. After eight weeks of therapy, sufferers also had an enchancment in maximum move price (10. The rules of treatment are to keep or restore low storage pressures and facilitate emptying. Antimuscarinic brokers are the first-line remedy to treat neurogenic detrusor overactivity and/or impaired compliance. Because the most important outcome is lower storage pressures, that is truly a desired consequence and sometimes finally results in decision of incontinence with appropriate emptying. In cases the place antimuscarinic brokers fail to lower bladder stress, consideration could be given to intradetrusor injection of botulinum toxin and even lower urinary tract reconstruction with bladder augmentation or urinary diversion. Indications could embody extreme detrusor overactivity, poor bladder compliance, or continued upper urinary tract deterioration regardless of aggressive conservative remedy. The duration of the impact of this remedy in this skeletal muscle is reported to vary between 50 and ninety days. The standardisation of terminology of decrease urinary tract operate: Report from the standardisation sub-committee of the International Continence Society. Risk factors for growing voiding dysfunction after abdominoperineal resection for adenocarcinoma of the rectum. Vesical dysfunctions after radical hysterectomy for cervical most cancers: a crucial evaluate. Lower urinary tract dysfunction as persistent complication of radical hysterectomy. Recent advances in understanding the biology of diabetesassociated bladder issues and novel remedy. Myogenic bladder decompensation in boys with a history of posterior urethral valves is caused by secondary bladder neck obstruction A comparability of spontaneous and nerve-mediated exercise in bladder muscle from man, pig and rabbit. Effect of tamsulosin on spontaneous bladder contraction in aware rats with bladder outlet obstruction: Comparison with impact on intraurethral pressure. Are feminine decrease urinary tract signs alleviated by -adrenoreceptor antagonists An experimental study of urodynamic effects of epidural morphine and of naloxone reversal. Drug effects on urinary bladder tone during spinal morphine-induced inhibition of the micturition reflex in unanesthetized rats. Association of stage of damage and bladder behavior in sufferers with post-traumatic spinal wire damage. Urodynamic analysis of surgical outcome in patients with urinary retention due to central lumbar disc prolapse. Urethral sphincter volumes in ladies with obstructed voiding and irregular sphincter electromyographic exercise. Urinary retention after tension-free vaginal tape procedure: incidence and therapy. Managing the urethra at transvaginal pelvic organ prolapse restore: a urodynamic method. Voiding dysfunction following incontinence surgery: analysis and treatment with retropubic or vaginal urethrolysis. Diagnosis and remedy of obstuction following incontincence surgery- urethrolysis and other strategies. Bulking brokers for stress urinary incontinence: short-term results and problems in a randomized comparison of periurethral and transurethral injections. Sonographic findings in acute urinary retention secondary to retroverted gravid uterus: pathophysiology and preventive measures. Videourodynamic characteristics and lower urinary tract symptoms of feminine bladder outlet obstruction.
20mg geodon otc
Subjective and objective end result of botulinum toxin sort A therapy in vulvodynia: pilot data depression recurrence symptoms discount geodon 20mg without a prescription. Evidence-based criteria for pain of interstitial cystitis/painful bladder syndrome in women anxiety 8 months postpartum geodon 20 mg purchase without prescription. Effect of amitriptyline on symptoms in treatment na�ve sufferers with interstitial cystitis/painful bladder syndrome. A potential, randomized, placebo controlled, double-blind research of amitriptyline for the therapy of interstitial cystitis. Oral cimetidine offers efficient symptom reduction in painful bladder disease: a prospective, randomized, double-blind placebo-controlled trial. A pilot medical trial of oral pentosan polysulfate and oral hydroxyzine in sufferers with interstitial cystitis. A prospective double-blind clinically controlled multicenter trial of sodium pentosanpolysulfate in the remedy of interstitial cystitis and related painful bladder disease. A quantitatively managed methodology to research prospectively interstitial cystitis and show the efficacy of pentosanpolysulfate. Randomized, doubleblind, dose-ranging study of pentosan polysulfate sodium for interstitial cystitis. Cyclosporine A and pentosan polysulfate sodium for the treatment of interstitial cystitis: a randomized comparative examine. The twin serotonin and noradrenaline reuptake inhibitor duloxetine for the therapy of interstitial cystitis: outcomes of an observational research. Intravesical bacillus Calmette�Guerin and dimethyl sulfoxide for remedy of classic and non-ulcer interstitial cystitis: a potential, randomized double-blind research. Intravesical resiniferatoxin for the remedy of interstitial cystitis: a randomized, double-blind, placebo managed trial. A randomized managed trial of intravesical bacillus Calmette�Guerin for remedy refractory interstitial cystitis. The efficacy of intravesical Tice strain bacillus Calmette�Guerin in the treatment of interstitial cystitis: a double-blind, potential, placebo managed trial. A randomized, double-blind crossover trial of sertraline in girls with continual pelvic ache. Chronic pelvic pain handled with gabapentin and amitriptyline: a randomized managed pilot study. Mesendieck somatocognitive therapy as remedy method to persistent pelvic pain: outcomes of a randomized controlled intervention examine. Flashlamp excited dye laser remedy of idiopathic vulvodynia is secure and efficacious. Are patient symptoms predictive of the diagnostic and/or therapeutic value of hydrodistention Changes in urine markers and signs after bladder distention for interstitial cystitis. A potential, singleblind, randomized crossover trial of sacral vs pudendal nerve stimulation for interstitial cystitis. A randomized scientific trial on the advantage of adhesiolysis in patients with intraperitoneal adhesions and chronic pelvic ache. They have an result on 50% of grownup girls of their lifetime and 25% to 30% may have a recurrent an infection. Cystitis and pyelonephritis are inflammations of the bladder and renal parenchyma, respectively, and are most regularly, but not all the time, attributable to microbial invasion (usually by bacteria) (Table 17-1). Most infections are sporadic, happen in patients with out identified comorbidities or anatomical abnormalities of the urinary tract, and involve the decrease urinary tract. Key Points � Asymptomatic bacteriuria is outlined because the presence of micro organism with out associated irritation in the urinary tract. A variety of sexually transmitted organisms similar to Chlamydia trachomatis and herpes can colonize the urinary tract causing symptoms of cystitis. Foreign our bodies corresponding to urinary catheters are a serious danger factor for an infection via mechanisms that embody urethral trauma, compromise of local immunity, and by providing protected niche(s) for microbial proliferation and a floor for biofilm production. Bacterial Virulence Factors the power of bacteria to adhere to uroepithelial cells is a prerequisite for an infection to occur. This adherence reduces the chance of the bacteria being cleared from the urinary tract throughout voiding. These adhesins connect to complementary buildings on the uroepithelial cell wall and act not only to promote infection but additionally to assist promote development and toxin manufacturing. Other virulence elements that will facilitate infection are specific to each pathogen. These are inclined to originate from the gastrointestinal tract and ascend into the genitourinary system. Escherichia coli is the most typical organism and accounts for as much as 70% of community-acquired infections. The remainder of bacterial infections are predominantly brought on by Staphylococcus saprophyticus, and quite a lot of gram-negative rods within the genus enterobacteriaceae. This reservoir can then serve as a pool of micro organism that will reinitiate an infection. The vaginal flora is predominantly lactobacilli and this maintains an acidic pH within the vagina. Periurethral lactobacilli and uromucoid within the urine are thought to intervene with bacterial adherence and colonization of the decrease urinary tract. Examples of host factors that improve the danger of infection embrace impaired bladder emptying, urethral trauma, foreign bodies, pelvic tumors, glycosuria, genetic components, hypoestrogenic states, sexual activity, and use of spermicides (Table 17-2). Impaired bladder emptying can occur with neurogenic problems similar to diabetes, a quantity of sclerosis, cerebrovascular occasions, and anatomical abnormalities. Anticholinergic medication and prior anti-incontinence surgical procedures may also impair bladder emptying. Significant vaginal prolapse can lead to impaired emptying as the urethra is kinked. Pelvic tumors and inflammatory bowel issues could immediately invade the bladder and have an result on bladder emptying. Glycosuria that occurs in diabetes mellitus is a potent tradition medium for bacterial development. Pelvic tumors Glycosuria Genetic Hypoestrogenic state Sexual intercourse Spermicides Genetic components have been postulated to enhance the chance of recurrent infection. Women with recurrent infection are extra likely to be nonsecretors of histo-blood group antigens and E. The mucosal lining of the urinary tract has a selection of immune surveillance molecules that operate to recognize invading pathogens. These receptors function to provoke applicable host immune defenses when triggered by a pathogen and promote cytokine and chemokine responses to gram-negative pathogens.
Syndromes
- Deafness (gets worse over time)
- Fever
- Some infections
- Brain
- It is hard to tell high-pitched sounds (such as "s" or "th") from one another.
- What drugs you are taking, even drugs, supplements, or herbs you bought without a prescription
- Levothyroxine
- Have more than one sexual partner
Purchase geodon 40mg with amex
Several veins drain the kidney and unite in a variable fashion to kind the renal vein mood disorder vs borderline personality disorder cheap geodon 80mg on-line. The arteries to the ureters arise primarily from three sources: the renal artery depression definition australia 20mg geodon trusted, testicular or ovarian arteries, and belly aorta. The endocrine operate of the suprarenal glands makes their plentiful blood supply essential. Lymphatic vessels from the superior a half of the ureter may be a part of those from the kidney or move directly to the lumbar (caval and aortic) nodes. Lymphatic vessels from the middle part of the ureter often drain into the frequent iliac lymph nodes, whereas vessels from its inferior half drain into the widespread, exterior, or internal iliac lymph nodes. The suprarenal lymphatic vessels arise from a plexus deep to the capsule of the gland and from one in its medulla. The nerves to the belly part of the ureters derive from the renal, stomach aortic, and superior hypogastric plexuses. Visceral afferent fibers conveying ache sensations comply with the sympathetic fibers retrograde to spinal ganglia and cord segments T11�L2. The nerves are mainly myelinated presynaptic sympathetic fibers that derive from the lateral horn of the spinal cord and traverse the paravertebral and prevertebral ganglia, without synapse, to be distributed to the chromaffin cells within the suprarenal medulla. The transpyloric airplane passes via the superior pole of the best kidney, which is roughly 2. The ranges of the kidneys change throughout respiration and with modifications in posture of Median plane Scapular line Diaphragm Liver Spleen T10 T11 Transpyloric aircraft Left kidney twelfth rib Right kidney Ureter Iliac crest Ilium Dimple indicating posterior superior iliac spine (A) Posterior view L4 L5 T12 L1 5cm 2�3 cm in a vertical course. In lean adults, the inferior pole of the best kidney is palpable by bimanual examination as a agency, smooth, somewhat rounded mass that descends during inspiration. The ureters occupy a sagittal airplane that intersects the ideas of the transverse processes of the lumbar vertebrae. For instance, the fascia at the renal hilum firmly attaches to the renal vessels and ureter, often stopping spread of pus to the contralateral facet. However, pus from an abscess (or blood from an injured kidney) might pressure its method into the pelvis between the loosely hooked up anterior and posterior layers of the pelvic fascia. Intraperitoneal Injection and Peritoneal Dialysis the peritoneum is a semipermeable membrane with an extensive floor area, much of which (subdiaphragmatic portions in particular) overlies blood and lymphatic capillary beds. For this reason, anesthetic agents, corresponding to options of barbiturate compounds, may be injected into the peritoneal cavity by intraperitoneal injection. In renal failure, waste merchandise similar to urea accumulate within the blood and tissues and in the end attain deadly ranges. Diffusible solutes and water are transferred between the blood and the peritoneal cavity on account of focus gradients between the 2 fluid compartments. Renal Transplantation Renal transplantation is now a longtime operation for the therapy of chosen instances of chronic renal failure. The renal artery and vein are joined to the adjacent exterior iliac artery and vein, respectively, and the ureter is sutured into the nearby urinary bladder. Accessory Renal Vessels During their "ascent" to their final website, the embryonic kidneys obtain their blood supply and venous drainage from successively extra superior vessels. Usually, the inferior vessels degenerate as superior ones take over the blood supply and venous drainage. Failure of a few of these vessels to degenerate results in accessory (or polar) renal arteries and veins. Variations in the number and place of these vessels occur in about 25% of people. Congenital Anomalies of Kidneys and Ureters Bifid renal pelvis and ureter are pretty widespread. These anomalies outcome from division of the metanephric diverticulum (ureteric bud), the primordium of the renal pelvis and ureter. The extent of ureteral duplication is dependent upon the completeness of embryonic division of the metanephric diverticulum. The bifid renal pelvis and/or ureter may be unilateral or bilateral; nonetheless, separate openings into the bladder are uncommon. Incomplete division of the metanephric diverticulum leads to a bifid ureter; complete division ends in a supernumerary kidney. In roughly 1 in 600 fetuses, the inferior poles (rarely, the superior poles) of the kidneys fuse to kind a horseshoe kidney. This U-shaped kidney usually lies on the level of the L3�L5 vertebrae as a end result of the foundation of the inferior mesenteric artery prevented normal relocation of the kidneys. Horseshoe kidney often produces no symptoms; nonetheless, related abnormalities of the kidney and renal pelvis may be present, obstructing the ureter. Sometimes, the embryonic kidney on one or either side fails to reach the stomach and lies anterior to the sacrum. Although uncommon, awareness of the potential for an ectopic pelvic kidney ought to stop it from being mistaken for a pelvic tumor and eliminated. Depending on the level of obstruction, the ache may be referred to the lumbar (loin) or inguinal regions (groin), the proximal anterior aspect of the thigh, or the external genitalia and/ or testis. The pain is referred to the cutaneous areas innervated by the spinal cord segments and sensory ganglia, which provide the ureter-mainly T11�L2. Another approach, lithotripsy, focuses a shock wave by way of the body that breaks the stones into fragments, which then move with the urine. The sympathetic a part of the autonomic nervous system within the stomach consists of � Abdominopelvic splanchnic nerves consisting of decrease thoracic splanchnic nerves (greater, lesser, and least) from the thoracic part of the sympathetic trunks and lumbar splanchnic nerves from the lumbar a part of the sympathetic trunks � Prevertebral sympathetic ganglia � Abdominal aortic plexus and its extensions, the periarterial plexuses. The plexuses are combined, shared with the parasympathetic nervous system and visceral afferent fibers. These presynaptic sympathetic fibers originate from cell our bodies within the intermediolateral cell column, or lateral horn, of the gray matter of spinal twine segments T7� L2 or L3. The fibers move successively by way of the anterior roots, anterior rami, and white communicating branches of thoracic and upper lumbar spinal nerves to attain the sympathetic trunks. They move through the paravertebral ganglia of the sympathetic trunks without synapsing to enter the abdominopelvic splanchnic nerves, which convey them to the prevertebral ganglia of the abdominal cavity. The abdominopelvic splanchnic nerves embrace the decrease thoracic splanchnic nerves and the lumbar splanchnic nerves. The larger splanchnic nerve (from the sympathetic trunk from the T5�T9 or T10 vertebral levels), lesser splanchnic nerve (from the T10�T11 levels), and least splanchnic nerve (from the T12 level) are the specific thoracic splanchnic nerves that arise from the thoracic part of the sympathetic trunks and pierce the corresponding crus of the diaphragm to convey the presynaptic sympathetic fibers to the celiac, aorticorenal, and superior mesenteric (prevertebral) sympathetic ganglia and plexuses, respectively. The lumbar splanchnic nerves come up from the abdominal a part of the sympathetic trunks. Medially, the lumbar sympathetic trunks give off three or four lumbar splanchnic nerves, which cross to the intermesenteric, inferior mesenteric, and superior hypogastric plexuses, conveying presynaptic sympathetic fibers to the associated prevertebral ganglia of those plexuses. The cell our bodies of postsynaptic sympathetic neurons constitute the main prevertebral ganglia that cluster across the roots of the most important branches of the stomach aorta-the celiac, aorticorenal, superior mesenteric, and inferior mesenteric ganglia-and minor, unnamed prevertebral ganglia that happen inside the intermesenteric, belly, aortic, and superior hypogastric plexuses. The synapse between presynaptic and postsynaptic neurons happens within the prevertebral ganglia. Postsynaptic sympathetic nerve fibers cross from the prevertebral ganglia to the stomach viscera by way of the periarterial plexuses related to the branches of the stomach aorta.
Discount 80 mg geodon overnight delivery
Free vascularized fibulas have been used to restore skeletal integrity to limbs by which congenital bone defects exist and to exchange segments of bone after trauma or excision of a malignant tumor mood disorder questionnaire-adolescent geodon 80 mg cheap mastercard. The periosteum and nutrient artery are usually eliminated with the piece of bone so that the graft will stay alive and grow when transplanted to another site mood disorder facility generic 20 mg geodon. The transplanted piece of fibula, secured in its new web site, ultimately restores the blood supply of the bone to which it has been attached. Tibial fractures in youngsters are more critical in the event that they involve the epiphysial plates because continued regular development of the bone may be jeopardized. All such fractures of the immature skeleton are routinely characterized by the Salter-Harris classification that describes the pattern of involvement. The tibial tuberosity normally varieties by inferior bone development from the superior epiphysial middle at approximately 10 years of age, but a separate middle for the tibial tuberosity might appear at approximately 12 years of age. Metatarsal and phalangeal fractures are a common injury in endurance athletes and may also happen when a heavy object falls on the foot. Metatarsal fractures are additionally common in dancers, especially feminine ballet dancers using the demi-pointe approach. Its place is simple to find because it lies at the bottom of a skin dimple, approximately 4 cm lateral to the midline, demarcating posteriorly the placement of the sacro-iliac joint. The thick gluteus maximus and fat obscure the tuberosity when the hip joint is prolonged. The gluteal fold, a outstanding pores and skin fold containing fats, coincides with the inferior border of the gluteus maximus muscle. Because it lies close to the skin, the greater trochanter causes discomfort whenever you lie in your facet on a hard surface. In the anatomical place, a line joining the information of the higher trochanters usually passes by way of the centers of the femoral heads and pubic tubercles. The medial and lateral condyles of the femur are subcutaneous and simply palpated when the knee is flexed or prolonged. The patellar surface of the femur is where the patella slides during flexion and extension of the knee joint. The lateral and medial margins of the patella can be palpated when the knee joint is flexed. The adductor tubercle, a small prominence of bone, could additionally be felt at the superior part of the medial femoral condyle. The prominence at the ankle, the medial malleolus, is subcutaneous, and its inferior end is blunt. The medial and lateral tibial condyles could be palpated anteriorly at the sides of the patellar ligament, especially when the knee joint is flexed. The head of the fibula may be palpated at the level of the superior a half of the tibial tuberosity because its knob-like head is subcutaneous at the posterolateral side of the knee. Note that the tip of the lateral malleolus extends farther distally and more posteriorly than does the tip of the medial malleolus. The tuberosity of the fifth metatarsal varieties a outstanding landmark on the lateral aspect of the foot and may be palpated simply on the midpoint of the lateral border of the foot. The shafts of the metatarsals and phalanges could be felt on the dorsum of the foot between the extensor tendons. Lateral malleolus Medial malleolus Head of talus (indicated by thumb) Tuberosity of navicular Bones of Foot the top of talus is palpable anteromedial to the proximal a part of the lateral malleolus when the foot is inverted and anterior to the medial malleolus when the foot is everted. Eversion of the foot makes the head of talus more distinguished because it moves away from the navicular. The head of talus occupies the area between the sustentaculum tali and the tuberosity of navicular. The sustentaculum tali is the one a part of the medial facet of the calcaneus which may be palpated as a small prominence simply distal to the tip of the medial malleolus. The tuberosity of the navicular is definitely seen and palpated on the medial facet of the foot, infero-anterior to the tip of the medial malleolus. Usually, palpation of bony prominences on the plantar floor of the foot is tough because of the thick skin, fascia, and pads of fat. The cuboid may be felt on the lateral aspect of the foot, posterior to the bottom of the 5th metatarsal. The medial cuneiform can be indistinctly palpated between the tuberosity of the navicular and the base of the first metatarsal. The head of the first metatarsal forms a prominence on the medial facet of the foot. The subcutaneous tissue of the hip and thigh is steady with that of the inferior a part of the anterolateral abdominal wall and buttocks. At the knee, the subcutaneous tissue loses its fats anteriorly and laterally, and blends with the deep fascia, but fat is present posteriorly in the popliteal fossa and again distal to the knee within the subcutaneous tissue of the leg. This fascia limits outward extension of contracting muscles, making muscular contraction more environment friendly in compressing the veins to push blood towards the heart. The fascia lata attaches to and is continuous with � the inguinal ligament, pubic arch, physique of pubis, and pubic tubercle superiorly. The membranous layer of subcutaneous tissue (Scarpa fascia) of the inferior abdominal wall also attaches to the fascia lata just inferior to the inguinal ligament. This broad band of fibers can be the aponeurosis of the tensor fasciae latae and gluteus maximus muscle tissue. The thigh muscular tissues are separated into three fascial compartments: anterior, medial, and posterior. The lateral intermuscular septum is robust; the opposite two septa are relatively weak. The transverse intermuscular septum divides the plantarflexor muscles within the posterior compartment into superficial and deep parts. Venous Drainage of Lower Limb the decrease limb has superficial and deep veins; the superficial veins are within the subcutaneous tissue, and the deep veins are deep to the deep fascia and accompany the most important arteries. The nice saphenous vein is fashioned by the union of the dorsal digital vein of the nice toe and the dorsal venous arch of the foot. Its medial margin is clean, however its superior, lateral, and inferior margins type a sharp edge, the falciform margin. The nice saphenous vein and some lymphatics cross through the saphenous opening and cribriform fascia to enter the femoral vein and the deep inguinal lymph nodes, respectively. The crural fascia is thick within the proximal part of the anterior aspect of the leg, where it varieties part of the proximal attachments of the underlying muscle tissue. Although thin in the distal part of the leg, the crural fascia is thickened the place it forms the extensor retinacula. Anterior and posterior intermuscular septa pass from the deep surface of the crural fascia and fasten to the corresponding margins of the fibula. Great saphenous vein and superficial lymphatic drainage with inset of saphenous opening. Small saphenous vein and superficial lymphatic drainage (arrow) to the popliteal lymph nodes.
Geodon 40mg discount
Within the lung depression keeping me from working geodon 20mg discount with amex, every artery descends posterolateral to the principle bronchus and divides into lobar and segmental arteries anxiety knee pain geodon 20 mg discount. Consequently, an arterial branch goes to every lobe and bronchopulmonary phase of the lung, often on the anterior facet of the corresponding bronchus. The pulmonary veins, two on both sides, carry well-oxygenated (arterial) blood from the lungs to the left atrium of the guts. Beginning in the pulmonary capillaries, the veins unite into bigger and bigger vessels. Intrasegmental veins drain blood from adjoining bronchopulmonary segments into the intersegmental veins in the septa, which separate the segments. The veins from the parietal pleura be part of the systemic veins in adjoining elements of the thoracic wall. The left bronchial arteries come up from the thoracic aorta; nonetheless, the best bronchial artery may come up from � A superior posterior intercostal artery � A common trunk from the thoracic aorta with the best third posterior intercostal artery � A left superior bronchial artery the small bronchial arteries present branches to the superior esophagus and normally then move alongside the posterior features of the primary bronchi, supplying them and their branches as far distally as the respiratory bronchioles. The most distal branches of the bronchial arteries anastomose with branches of the pulmonary arteries within the walls of the bronchioles and within the visceral pleura. The right bronchial vein drains into the azygos vein, and the left bronchial vein drains into the accent hemi-azygos vein or the left superior intercostal vein. The superficial lymphatic plexus lies deep to the visceral pleura and drains the lung parenchyma (tissue) and visceral pleura. Lymphatic vessels from the plexus drain into the bronchopulmonary (hilar) lymph nodes within the hilum of the lung. Inferior view Lobes of right lung: Superior lobe Apical Posterior Anterior Middle lobe Lateral Medial Inferior lobe Superior Anterior basal Medial basal Lateral basal Posterior basal Lobes of left lung: Superior lobe Apical Posterior ** Anterior Superior lingular Inferior lingular Inferior lobe Superior Anterior basal Medial basal Lateral basal Posterior basal Lateral view (C) Right lung Medial view Ant. The bronchopulmonary segments are demonstrated after injection of different color latex into every tertiary segmental bronchus as proven in (E). The deep lymphatic plexus is located in the submucosa of the bronchi and in the peribronchial connective tissue. Lymphatic vessels from this plexus drain into the pulmonary lymph nodes positioned along the lobar bronchi. Lymph from the superficial and deep plexuses drains from the bronchopulmonary lymph nodes to the superior and inferior tracheobronchial lymph nodes, superior and inferior to the bifurcation of the trachea, respectively. Note that the right pulmonary artery passes underneath the arch of the aorta to attain the best lung and the left pulmonary artery lies completely to the left of the arch. Lymph from the tracheobronchial lymph nodes passes to the best and left bronchomediastinal lymph trunks. These trunks usually terminate on each side on the venous angles (junction of the subclavian and inner jugular veins); however, the proper bronchomediastinal trunk might first merge with different lymphatic trunks, converging here to kind the proper lymphatic duct. The superficial (subpleural) lymphatic plexus drains lymph from the visceral pleura. Lymph from the parietal pleura drains into the lymph nodes of the thoracic wall (intercostal, parasternal, mediastinal, and phrenic). A few lymphatic vessels from the cervical pleura drain into the axillary lymph nodes. Parasympathetic ganglion cells- cell our bodies of postsynaptic parasympathetic neurons-are in the pulmonary plexuses and alongside the branches of the bronchial tree. The sympathetic fibers are inhibitory to the bronchial muscle (bronchodilator), motor to the pulmonary vessels (vasoconstrictor), and inhibitory to the alveolar glands of the bronchial tree. The lymphatic vessels originate from superficial subpleural and deep lymphatic plexuses. E, esophagus; T, trachea; green, parasympathetic; purple, plexus; yellow, sympathetic. The pleural cavity is positioned between the parietal pleura and the visceral pleura. One lung could additionally be collapsed after surgery, for instance, with out collapsing the opposite as a result of the pleural sacs are separate. Pleural cavity Trachea Trajectory of bullet Air Parietal pleura Visceral pleura Parietal pleura Collapsed lung Inflated lung Air Visceral pleura irritation of the pleurae-pleuritis (pleurisy)-makes the lung surfaces rough. Acute pleuritis is marked by sharp, stabbing pain, particularly on exertion, corresponding to climbing stairs, when the speed and depth of respiration may be elevated even barely. Variation in Lobes of Lungs Occasionally, an extra fissure divides a lung or a fissure is absent. The commonest "accent" lobe is the azygos lobe, which appears in the proper lung in roughly 1% of people. In these cases, the azygos vein arches over the apex of the right lung and not over the right hilum, isolating the medial a half of the apex as an azygos lobe. Lung External intercostal Internal intercostal Innermost intercostal 9th rib Intercostal nerve Excess fluid in pleural cavity Diaphragmatic parietal pleura Diaphragm 10th rib Costal parietal pleura Liver Diaphragmatic parietal peritoneum Collateral department of intercostal nerve Pneumothorax, Hydrothorax, Hemothorax, and Chylothorax Entry of air into the pleural cavity-pneumothorax- ensuing from a penetrating wound of the parietal pleura or rupture of a lung from a bullet, for instance, results in partial collapse of the lung. This can also occur as a end result of leakage from the lung via a gap within the visceral pleura. The accumulation of a significant quantity of fluid within the pleural cavity- hydrothorax-may outcome from pleural effusion (escape of fluid into the pleural cavity). With a chest wound, blood can also enter the pleural cavity (hemothorax); this situation results extra typically from damage to a significant intercostal vessel than from laceration of a lung. Chyle is a pale white or yellow lymph fluid within the thoracic duct containing fat absorbed by the intestines (see Chapter 2). Auscultation and Percussion of Lungs Auscultation of the lungs (assessing air flow via the tracheobronchial tree into the lung with a stethoscope) and percussion of the lungs (tapping the chest over the lungs with the finger) all the time embody the root of the neck to detect sounds in the apices of the lungs. Percussion helps set up whether the underlying tissues are air-filled (resonant sound), fluid-filled (dull sound), or strong (flat sound). To auscultate this area, physicians apply a stethoscope to the inferoposterior side of the thoracic wall at the stage of the T10 vertebra. In addition to observation, biopsies may be taken and a few thoracic situations could be handled. Aspiration of Foreign Bodies Because the best bronchus is wider and shorter and runs more vertically than the left bronchus, aspirated international bodies usually have a tendency to enter and lodge in it or considered one of its branches. A potential hazard encountered by dentists is an aspirated foreign physique, similar to a piece of tooth or filling materials. Forceps Pleura Cauterizing thoracoscope Lung Monitor displaying excision of pleura (pleurectomy) Lung Resections Knowledge of the anatomy of the bronchopulmonary segments is important for precise interpretations of diagnostic pictures of the lungs and for surgical resection (removal) of diseased segments. When resecting a bronchopulmonary phase, surgeons comply with the interlobar veins to move between the segments. Bronchial and pulmonary disorders such as tumors or abscesses (collections of pus) often localize in a bronchopulmonary segment, which may be surgically resected. During the remedy of lung cancer, the surgeon may take away a whole lung (pneumonectomy), a lobe (lobectomy), or one or more bronchopulmonary segments (segmentectomy).
20mg geodon order free shipping
As a rule depression symptoms forum buy geodon 20 mg online, the tumor is richly vascular mood disorder klonopin geodon 20mg generic visa, causing pulsation or a distinctly audible bruit in some instances; massive hemorrhage could additionally be encountered during surgical removing. Local management of synovial sarcoma is clearly associated to the adequacy of initial surgical excision. Simple native excision with out ancillary therapy is incapable of checking the growth and unfold of the tumor. Most suggest intensive surgery because the therapy of alternative, together with radical native excision, typically with removing of a whole muscle or muscle group, and amputation, relying primarily on the dimensions of the tumor and its location. Because radical native excision is often unimaginable with tumors situated near a big joint-the favored location of synovial sarcoma-adjunctive radiotherapy along with native excision of the tumor is really helpful over amputation. Frequently, the tumor is surrounded by quite a few tortuous vessels of huge caliber. In reality the uniformity of the microscopic image is certainly one of its characteristic options. These cellular aggregates are separated from each other by thin-walled, sinusoidal vascular channels lined by a single layer of flattened endothelial cells. The particular person cells are large, rounded, or extra often polygonal and display little variation in measurement and form. B, Higher-power view reveals cell nests that are separated by thin-walled, sinusoidal vascular areas. At the margin of the tumor, there are usually quite a few dilated veins, in all probability the results of multiple arteriovenous shunts within the neoplasm. A, Typical cytologic appearance, with relatively uniform nuclei and distinguished nucleoli. C, High-magnification view of crystalline materials, diagnostic of alveolar delicate part sarcoma. The stories in regard to staining for muscle markers differ somewhat, however most have demonstrated muscle markers in less than 50% of tumors. Cytogenetic research of this tumor have identified a specific alteration, der(17)t(X;17) (p11. Both the crystals and the dense granules are membrane bound and encompass crystallized and uncrystallized filaments four to 6 nm in diameter, suggesting transitions between the two buildings. Primary renal cell carcinomas are normally demonstrable radiographically within the retroperitoneum. Paraganglioma and malignant granular cell tumor mainly have an result on patients older than 40 and are uncommon in patients younger than 25. Of the 91 patients with follow-up within the examine from Memorial SloanKettering Cancer Center (New York), only 15% of sufferers had been alive after 20 years. In contrast, the median survival for patients with metastases was 40 months, with 5-year total survival of 20%. All patients who had brain metastases had evidence of metastatic illness at different websites. Metastases are inclined to happen early within the disease course, with many reviews of sufferers who present with pulmonary or mind metastasis. Improved prognosis in children could also be partly associated to the situation of the tumor, early scientific detection, small measurement, and higher resectability. Most research advocate radical surgical excision of major and metastatic lesions mixed with radiotherapy or chemotherapy (or both), although success is limited with systemic therapies. Differential Diagnosis the differential prognosis chiefly contains metastatic renal cell carcinoma, paraganglioma, and granular cell tumor (Table 33. The cells of granular cell tumor are less properly outlined, have distinctly granular cytoplasm, and show robust S-100 protein expression. B, Higher-magnification view exhibiting shut simulation of renal cell carcinoma by this alveolar soft half sarcoma. This lesion has had a selection of names, including desmoplastic small cell tumor with divergent differentiation,427 intraabdominal desmoplastic small round cell tumor,428 malignant small cell epithelial tumor of the peritoneum coexpressing mesenchymal-type intermediate filaments,429 intraabdominal neuroectodermal tumor of childhood with divergent differentiation,430 and desmoplastic small cell tumor with multiphenotypic differentiation. Typically, the mobile aggregates are surrounded and separated by plentiful fibrous connective tissue with solely a scattering of spindle-shaped fibroblasts and myofibroblasts. Occasionally, the tumor cells have extra plentiful cleared-out or vacuolated cytoplasm or even a signet-ring look. Other unusual features embrace Homer Wright�like rosettes, papillary areas, zones that resemble transitional cell carcinoma, and areas composed predominantly of cells with a spindled morphology. Occasionally, immunostains for keratin reveal a dotlike sample of cytoplasmic immunoreactivity. The most typical complaint is belly distention, often associated with pain and constipation. Other signs and symptoms include intestinal or ureteral obstruction, ascites, issue with urination, and impotence. Rare cases are merely composed of solid sheets of round cells, making recognition of this uncommon tumor even more troublesome. The tumor cells seem undifferentiated and have small hyperchromatic nuclei with inconspicuous nucleoli. Cords of cells are surrounded by dense fibrous stroma mimicking lobular carcinoma of the breast. The immunohistochemical coexpression of epithelial, mesenchymal, and neural antigens, particularly the perinuclear dotlike or globular pattern of desmin staining, is beneficial for arriving at a diagnosis. Given that the immunophenotypic options overlap with many of the aforementioned tumors, a panel of immunostains is generally required. As talked about beforehand, a mixture of immunohistochemical and molecular assays should allow for these distinctions. The tumor mainly impacts younger adults; its principal websites are the fingers, palms, and forearms. Clinical Findings Epithelioid sarcoma is most prevalent in adolescents and younger adults 10 to 35 years of age, with a median age within the mid-20s. The tumor most frequently arises on the flexor surfaces of the fingers, hands, and forearm, followed by the knee and lower leg, especially the pretibial region, the buttocks and thigh, the shoulder and arm, and the ankle, foot, and toe. It is rare within the trunk and head and neck area, with the exception of the scalp. In a 1998 follow-up research, 25 of 35 sufferers with available follow-up died of widespread metastasis, and the remainder have been alive with illness. Radiographic examination sometimes reveals a gentle tissue mass with an occasional speckled sample of calcification. Cortical thinning and erosion of underlying bone may be present, but invasion and destruction of adjacent bone are uncommon. Deepseated tumors, attached to tendons or fascia, are probably to be bigger and present as firm, multinodular plenty with irregular outlines. The reduce floor has a glistening, gray-white or gray-tan, mottled floor with focal yellow or brown areas caused by focal necrosis or hemorrhage. Proximaltype epithelioid sarcoma tends to be larger and more infiltrative than the distal type.