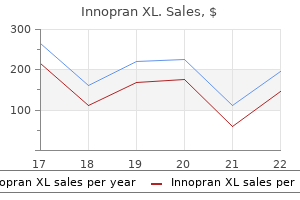
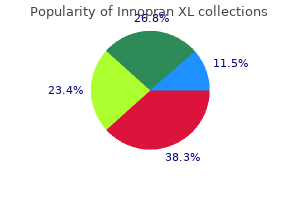
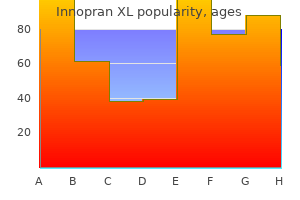
Innopran XL
Innopran XL dosages: 80 mg, 40 mg
Innopran XL packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Innopran xl 40 mg buy cheap
Parents attempt to pulse pressure 46 cheap 40 mg innopran xl amex comfort the children at evening and this can end result in parental sleep deprivation and daytime exhaustion heart attack types generic 40 mg innopran xl with mastercard. Sleep deprivation also has consequences for school-age kids (patients and siblings), affecting cognitive perform and behavior. Prognosis Most patients with atopic dermatitis improve with time, however a subset progresses to persistent skin illness and allergic rhinitis and/or bronchial asthma. Differential Diagnosis Cutaneous fungal infections: Tinea corporis could present in round plaques but these are usually annular (ring-shaped with central clearing). Atopic dermatitis: Individuals with atopic dermatitis usually have a personal or family history of atopic dermatitis (childhood eczema), allergic rhinitis, or bronchial asthma. Uncommon conditions might embody cutaneous T-cell lymphoma, subacute cutaneous lupus, granuloma annulare, psoriasis, or squamous cell carcinoma in situ. Pathophysiology the pathophysiology of nummular dermatitis is unknown, but thought to be linked to impaired skin barrier operate. Clinical Presentation History the patient sometimes complains of an itchy rash on the extremities. Some consultants consider dyshidrotic dermatitis and pompholyx to be distinct situations, although the terms are sometimes used interchangeably. Dyshidrotic dermatitis is widespread, affecting roughly 1% of the overall population,18 whereas pompholyx is rare. Pathophysiology the term "dyshidrosis" (meaning "tough sweating") is a misnomer. A few research have discovered a hyperlink between flares of vesicular palmoplantar dermatitis and oral ingestion of nickel in nickel-allergic sufferers. Laboratory Findings Skin biopsies are normally not diagnostic and are solely helpful to rule out different disorders. Clinical Presentation History the patient typically complains of pruritic or painful blisters on the palms and soles. Diagnosis the necessary thing diagnostic features of dyshidrotic dermatitis are small, grouped vesicles on the palms and/or soles. The most typical locations embrace lateral fingers, central palms, insteps, and lateral borders of the ft. Scabies: this may present with vesicles and papules on the palms and soles, but often there are burrows and extra widespread lesions. Vesiculobullous illnesses such as pemphigoid and pemphigus: Dyshidrotic eczema is usually noninflammatory and solely affects the palms and soles, whereas different vesiculobullous conditions have vital surrounding erythema and generally affect a number of physique sites. Clinical Presentation History the patient typically complains of localized areas of intensely pruritic pores and skin. In some cases, the continual rubbing and scratching turns into a subconscious or compulsive habit. Physical Examination Common places for primary lichen simplex chronicus embrace the lateral neck, scrotum/vulva, and dorsal foot. Secondary lichen simplex chronicus happens on the sites of the underlying pores and skin circumstances corresponding to in the antecubital and popliteal fossae in atopic dermatitis. A prurigo nodule is a term used for a lichenified papule that has been chronically picked and manipulated. Secondary prurigo nodularis might present with many widespread lichenified papules in patients with generalized pruritus as a outcome of systemic diseases such as liver or kidney disease. Management Dyshidrotic dermatitis is managed with mid- to highpotency topical corticosteroids (Table 8-3) twice a day. In people where sweat is a big aggravating issue, iontophoresis or onabotulinumtoxin (Botox) injections could also be helpful. Dyshidrotic dermatitis could not fully clear with therapy and recurrences are common. Diagnosis the key diagnostic features of lichen simplex chronicus are persistent, intensely pruritic, lichenified plaques, mostly commonly found on the neck, genitals, or dorsum of the foot. As a secondary analysis, it results after years of scratching because of another situation, most commonly atopic dermatitis. Chronic rubbing and scratching of the pores and skin leads to thickening of the dermis and fibrosis of the dermis. Psychological disorders: Usually different indicators of psychological disease are present. Management Primary lichen simplex chronicus is typically managed with class 1 or 2 excessive to superpotent topical corticosteroid ointments or lotions twice a day (Table 8-3). Corticosteroid-impregnated tapes, similar to Cordran Tape which could be applied immediately over the plaque, are often useful. Oral antidepressants or antihistamines, particularly doxepin, may profit people with nighttime itching and sleep disturbance. It is essential that patients turn out to be conscious of the habit or compulsion to scratch or rub, replacing these actions with pushing on the pores and skin. For generalized prurigo nodularis, ultraviolet mild remedy is often very useful. Contact dermatitis in the United States: epidemiology, financial impression, and office prevention. Hand dermatitis: a evaluate of scientific options, therapeutic options, and long-term outcomes. Development of the Childhood Atopic Dermatitis Impact Scale: preliminary validation of a quality-of-life measure for young children with atopic dermatitis and their households. Calcineurin inhibitors in pediatric atopic dermatitis: a evaluate of present evidence. Steven Padilla Pityriasis Rosea / 67 Lichen Planus / 68 References / 69 Psoriasis, seborrheic dermatitis, pityriasis rosea, and lichen planus are ailments that present with papulosquamous lesions (scaly papules and plaques). Although these ailments may have a similar morphology, their underlying etiologies range. Secondary syphilis, cutaneous T-cell lymphomas, and connective tissue disease may present with papulosquamous lesions and should be included in the differential prognosis. Patient typically are selfconscious, depressed, or annoyed over the appearance of their skin. Psoriasis spans all socioeconomic groups, and its prevalence varies by geographic location. The fee of psoriatic disease is lower in African Americans compared with that in European Americans. This dysregulation is likely triggered by hyperactivity of the innate immunological surveillance system to environmental antigens. In genetically predisposed people, the Th1 pathway response is overstimulated. Diets high in fish oils seem to be protecting towards the event of psoriasis. Although most medical literature prior to Willan (1757-1812) lumped psoriasis, leprosy, eczema, and different inflammatory dermatoses in to a complicated menagerie, Celsus gave a convincing account of psoriasis vulgaris nearly 2000 years in the past. His description included many of the morphologic options that physicians at present make the most of to diagnose psoriasis, including the "ruddy" or salmon-colored plaques with silvery scales that usually are associated with punctate hemorrhage or "erosions" when eliminated.
40 mg innopran xl generic
Excludes: Lichen planus blood pressure record chart innopran xl 40 mg buy free shipping, frictional keratosis hypertension jnc8 buy 80 mg innopran xl with mastercard, tobacco pouch keratosis, nicotine stomatitis, linea alba, leukoedema, actinic cheilitis, hypertrophic candidiasis, bushy leukoplakia, white sponge nevus, and squamous cell carcinoma. Also, combination of heavy smoking and alcohol abuse results in a synergistic effect and increases the risk further. In the concept of oral premalignancy/squamous cell carcinoma one should embody erythroplakia. However, this definition is deceptive as a end result of at the time of biopsy lesions of erythroplakia present severe dysplasia, carcinoma in situ, or invasive squamous cell carcinoma. It occurs in middle aged to older adults and the sites of predilection are the ground of mouth, tongue, and taste bud. The gold normal for the diagnosis of clinically recognized suspicious oral lesions is surgical biopsy. Such is the case of lesions seen in association with dental prostheses or Management Surgical excision is the treatment of choice for leukoplakic lesions. Photodynamic therapy15 using 5-aminolevulinic acid is a promising alternative for remedy of dysplastic lesions. Cryosurgery and administration of 13-cis-retinoic acid have been used with limited outcomes. Oral Squamous Cell Carcinoma Introduction Oral most cancers accounts for lower than 3% of all cancers in the United States. Management Diagnostic biopsies should be obtained of all lesions that current with the aforementioned traits. Treatment of oral most cancers entails a staff of physicians that embrace ear, nose, and throat/oral surgery and maxillofacial specialists, oncologists, and prosthodontists. Oral papilloma is a typical benign epithelial proliferation much like widespread warts of the pores and skin. Occasionally, a couple of site could be simultaneously affected (papillomatosis) particularly within the immunocompromised patients. Condyloma acuminatum can happen in the oral mucosa and has similar clinical and histopathologic traits of genital lesions. When recognized in the mouth of youngsters, sexual abuse is a concern and must be investigated. Although trauma has been traditionally regarded as the reason for oral fibrous overgrowths, the etiology is unknown. Most lesions arise on the buccal mucosa, tongue, and lips, and their size hardly ever exceeds 1. Most instances are seen in the 4th to 6th many years of life and females are twice as incessantly affected as males. The observed higher frequency in females may be due to the reality that women are extra concerned about their esthetics or oral health compared to males. Also, fibrous hyperplastic lesions could also be seen on the alveolus of sufferers with ill-fitting dentures. Surgical excisional biopsy to affirm the prognosis and to exclude other gentle tissue tumors is recommended. Mucocele17 refers to a clinically fluctuant nodular mass containing salivary mucus. It is both of extravasation kind due to severing of a salivary gland excretory duct and spillage of mucus in the connective tissue, or retention kind, resulting from obstruction of a salivary duct, the latter being less common. Retention-type mucoceles are seen in older adults on the higher lip, floor of mouth, and buccal mucosa. Thus, for a fluctuant lesion on the decrease lip of a kid or young grownup, the prognosis is most likely that of a mucocele till confirmed histopathologically otherwise. These lesions are sometimes retention mucoceles, or benign or malignant cystic salivary gland tumors. There is an unusual variant referred to as superficial mucocele seen on the posterior palate and buccal mucosa. They appear as single or multiple small translucent vesicles filled with clear saliva. Multiple lesions, clustered or not, may be encountered in association with lichenoid issues. Epulides are nodular gentle tissue lesions usually on the gingiva and the alveolar mucosa. As a rule, fibrovascular inflammatory hyperplasias and peripheral big cell granulomas are normally erythematous and hemorrhagic. Also, sure systemic medicines may cause pigmented lesions within the oral mucosa by either a rise in melanin pigment or deposition of medication metabolites within the soft tissues. Melanin pigmentation presenting as hyperpigmentation on the tips of the fungiform papillae in African American individual. Females are extra incessantly affected most likely due to interplay with sex hormones. In most instances the sufferers are conscious of their situation and its medical manifestations. Among such situations one should embody Laugier� Hunziker (Laugier�Hunziker�Baran) syndrome seen extra frequently in females, by which patients develop a quantity of oral melanocytic macules and less frequently nail and vaginal lesions. As is the case on the skin, there are three widespread histologic sorts, junctional, compound, and intramucosal, the latter being probably the most frequent kind. Other uncommon forms, for example, Spitz, halo, mixed, and congenital nevi have additionally been reported. Most oral melanomas are clinically and histologically just like acral lentiginous or nodular melanomas of the pores and skin or a combination of the 2. Hyperpigmentation occurs because of disruption of the basal cell layer resulting in Non-melanin-Related Hyperpigmentations these lesions are brought on by either exogenous or endogenous pigments. Lesions are usually situated on the gingiva, alveolar mucosa, buccal mucosa, ground of mouth, and fewer usually the tongue. The shade is gentle to darkish gray and even black relying on the quantity and depth of the metal inside the tissues. Particles of amalgam may be imbedded inside the tissues during restorative procedures. Occasionally, metallic particles can be identified in dental radiographs as small radiopaque particles. Similar discolorations can occur from incidental or voluntary introduction of other metals similar to graphite from pencil suggestions, tattoo ink, and chronic contact with charcoal toothpaste. Rare systemic conditions related to non-melanin-associated hyperpigmented lesions of tooth and delicate tissues include hemochromatosis, erythroblastosis fetalis and biliary atresia associated hyperbilirubinemia, beta thalassemia, and congenital erythropoietic porphyria. Chronic exposure to heavy metals such as bismuth, lead, gold, or silver could cause oral hyperpigmented lesions, but nowadays, such cases are uncommon. Finally metabolites of certain drugs, the most frequent being minocycline, could trigger diffuse discoloration of tooth, oral delicate tissues, and bone. In most situations in minocycline-related hyperpigmentation the lesions are related to iron-chelated metabolites. Direct trauma to a tooth or tooth might lead to pulpal necrosis and discoloration of affected teeth.
Best innopran xl 80 mg
Vaginal hysterectomy could additionally be accomplished selectively (stage I blood pressure medication good for kidneys innopran xl 80 mg generic, with well-differentiated tumor) in patients with uterovaginal prolapse or with extreme weight problems blood pressure unsafe levels innopran xl 80 mg safe. Contraindications of radiotherapy: Presence of a pelvic mass, pelvic kidney, pyometra, pelvic abscess, previous laparotomies and/or adhesions with bowel and prior pelvic radiation. External pelvic and intracavitary radiation followed by prolonged hysterectomy 6 weeks later in instances of: - iN stagE ii carciNoMa administration choices are: A. Radical hysterectomy bilateral salpingooophorectomy with pelvic and para-aortic lymphadenectomy (see p. Combined radiation and surgical procedure: Radiation (external and intracavitary) adopted in 6 weeks by whole stomach hysterectomy and bilateral salpingo-oophorectomy. Initial surgery (modified radical hysterectomy) adopted by external and intravaginal radiation. The response is sweet in well-differentiated carcinoma with 360 TexTbook of GynecoloGy of endometrial cancer is a debatable issue. In a affected person with severe postmenopausal symptoms progestin (medroxy progesterone acetate, 5�10 mg daily) may be a alternative. ProgNosis: the poorly differentiated tumor, the greater diploma of myometrial penetration, lymphovascular area invasion and the superior stages are prognostically poor. Histologically non-endometrioid tumors are aggressive and carry increased danger of recurrence. The medication commonly used are adriamycin, cisplatin, carboplatin, paclitaxel and cyclophosphamide (see ch. The extrapelvic metastases are seen within the lung, lymph nodes (aortic), liver, brain and bones. Evaluation of signs, thorough clinical examination and X-ray chest (annual) are essential. Histologic kind (typical adenocarcinomas - better prognosis, papillary serous, clear cell carcinoma - poor prognosis). Ploidy standing - aneuploid tumors have gotten poor prognosis in comparability with diploid tumors. This is clinically recognized when the affected person presents with (a) Irregular vaginal bleeding. More than 50 % occur after molar pregnancy, about 25 % after abortion and/or ectopic pregnancy and some after normal being pregnant. Non-metastatic (locally invasive) lesions develop in 15 percent and metastatic lesions develop in about four % of sufferers after molar evacuation. Placental Site Trophoblastic Tumor the tumor arises from the trophoblast of the placental bed. Syncytiotrophoblast cells are generally absent, as a substitute intermediate trophoblast cells are predominant. The outstanding options of this type of mole are invasive and damaging potentialities. Invasive mole reveals abnormal penetration through the muscle layers of � Persistent hydatidiform mole � invasive mole � choriocarcinoma � Placental web site trophoblastic tumor Non-metastatic illness (confined to the uterus) Metastatic illness: a. The uterine wall could also be perforated at multiple areas showing purple, fungating development with massive intraperitoneal hemorrhage. The neoplasm might invade the pelvic blood vessels and metastasizes to vagina or distant websites as like these in choriocarcinoma. The supplies for uterine curettage are often misleading as the lesion could additionally be deep contained in the myometrium. Ovarian choriocarcinoma (non-gestational) may be related to malignant teratoma or dysgerminoma. The nodular sort could additionally be located deep in the myometrium with overlying endometrium intact. The widespread sites of metastases are lungs (80%), anterior vaginal wall (30%), brain (10%), liver (10%) and others. Amongst all patients with choriocarcinoma, around 50 % develop following a hydatidiform mole, 30 percent happen after a miscarriage or an ectopic pregnancy and 20 percent after an apparently regular being pregnant. Rarely, its relation with a term being pregnant, abortion or ectopic pregnancy may be established. Other signs as a end result of metastatic lesions are: Lung: Cough, breathlessness, hemoptysis. There may be a purplish pink nodule within the lower-third of the anterior vaginal wall. Unilateral or bilateral enlarged ovaries could additionally be palpable by way of lateral fornices. It is emphasized that, the curetted materials may not reveal the analysis in all of the instances, because the lesion could also be deep within the myometrium or the uterus may not be the first site. One must be very cautious and alert while doing uterine curettage as brisk hemorrhage might occur for which a life saving hysterectomy might have to be done. Massive hemorrhage following resection may have packing or selective embolization. Chest: Metastases to different sites are uncommon when pelvic examination and chest X-ray are normal. In general, sufferers with non-metastatic (low risk) and good prognosis disease are handled successfully with single agent remedy (Methotrexate or Actinomycin). Whatever drugs are used, the essential formalities are to be followed as tabulated in Table 23. Disadvantage of routine chemotherapy is unnecessary publicity of the toxic medicine to all ladies who could not need it. Meticulous follow up following evacuation of hydatidiform mole is essential for no much less than 6 months to detect early proof of trophoblastic reactivation. Diagnostic uterine curettage in unexplained irregular bleeding, eight weeks following term delivery or abortion. Increased danger for the development of secondary malignancies after treatment with a quantity of agent chemotherapy has been observed. The ovaries are normally not concerned and if involved, can be effectively cured with postoperative chemotherapy. Intrathecal excessive dose methotrexate may be administered to prevent hemorrhage and for tumor shrinkage. Liver metastasis: Interventional radiology (hepatic artery ligation or embolization) or complete liver radiation (2000 cGy over 10 days) together with chemotherapy could additionally be effective. Prognosis: the treatment price is nearly 100% in low risk and about 70 p.c in high risk metastatic groups. Depending on mitotic activity endometrial stromal tumors are of three types: (i) endometrial stromal nodule (mostly benign), (ii) endolymphatic stromal myosis (low grade malignancy) and (iii) endometrial stromal sarcoma (high grade malignancy). Intravenous leiomyomatosis - where benign easy muscle grows in to venous channels throughout the broad ligaments, uterine and iliac veins. It is thought to arise from the metaplasia of subperitoneal mesenchymal stem cells to smooth muscle, fibroblasts, myofibroblasts under the affect of estrogen and progesterone. The cut part exhibits yellowish look with hemorrhage and cystic degeneration. Histologically, three types of cells are seen - spindle, spherical or combination of the two together with giant cells.
80 mg innopran xl purchase overnight delivery
Paravagial defect may be because of: full detachment of pubocervical fascia from the arcus tendineus fascia blood pressure medication makes me tired innopran xl 40 mg cheap without a prescription. The size of the anterior vaginal wall is 7 cm and that of posterior wall is 9 cm blood pressure chart exercise 80 mg innopran xl quality. Isthmus is bounded above by the anatomical inner os and under by the histological internal os. Fallopian tube has received 4 parts-interstitial (1 mm diameter), isthmus, ampullary (fertilization takes place) and infundibulum (6 mm diameter). The cortex is studded with follicular buildings and the medulla accommodates hilus cells that are homologous to the interstitial cells of the testes. It is relatively constricted (i) where it crosses the brim, (ii) the place crossed by the uterine artery, and (iii) within the intravesical part. The ureter is more probably to be broken throughout hysterectomy on the infundibulopelvic ligament, by the aspect of the cervix, at the vaginal angle and during posterior peritonization. Superficial perineal pouch is shaped by the deep layer of the superficial perineal fascia and inferior layer of the urogenital diaphragm. The deep perineal pouch is shaped by the inferior and superior layer of the urogenital diaphragm. Obstetrical perineum is the fibromuscular structure, pyramidal-shaped with the bottom coated by the perineal skin and situated in between the vaginal and anal canal. Pelvic cellular tissues (endopelvic fascia), ligaments, perineal body, pelvic flooring muscle tissue (leavtor ani), support the pelvic organs and counter acts the downward thrust of elevated intra-abdominal pressure (see p. Broad ligament has obtained 4 elements - infundibulopelvic ligament, mesovarium, mesosalpinx and mesometrium. Broad ligament incorporates Fallopian tube, spherical ligament, ovarian ligament, parametrium, utero-ovarian anastomotic vessels, nerves, lymphatics of the uterus, tubes and ovaries and vestigial structures-duct of Gartner, epoophoron and paroophoron. One finish is hooked up to cornu of the uterus and the other finish terminates within the anterior third of the labium majus. Uterine artery Origin: the uterine artery arises both instantly from the interior iliac artery or in common with the obliterated umbilical artery. Course: It runs downwards and forwards along the lateral pelvic wall virtually in the same direction because the ureter until it reaches the bottom of the broad ligament. It then turns medially and crosses the ureter anteriorly from above and at proper angle to it; about 1. On reaching the side of the uterus, it runs upwards and takes a spiral course alongside the lateral uterine wall between the layers of broad ligament. It in the end anastomoses end on with the tubal department of the ovarian artery within the mesosalpinx. Branches the following branches are given off: Ureteric-as it crosses it Descending cervical Circular artery to the cervix: this is fashioned by anterior and posterior branches of the artery to the cervix of either side Segmental arcuate arteries: these are the branches from the ascending half. These pierce about one-third of the myometrium after which divide in to anterior and posterior branches. These anastomose with the corresponding branches of the opposite side within the midline. From the arcuate arteries, a collection of radial arteries come up virtually at right angles, which stretch by way of the whole size of the myometrium. Near the myoendometrial junction, the radial arteries are divided into: (a) Short basal artery-supplies the basal endometrium. Vaginal artery Origin: the vaginal artery arises both from the uterine artery or instantly from the anterior division of Chapter 2 Blood Vessels, lymphatiC drainage and innerVation of pelViC organs 27 the inner iliac artery. It is in relation to the lateral fornix and then runs down along the lateral wall of the vagina. Numerous transverse branches are despatched off anteriorly and posteriorly, which anastomose with the same branches of the opposite aspect to form azygos arteries of the vagina-one anterior and one posterior. Other arteries contributing to azygos arteries are: (i) Descending cervical, (ii) Circular artery to the cervix, (iii) Inferior vesical, and (iv) Internal pudendal. Beyond the infundibulopelvic ligament, there are two ovarian veins on each side, which ascend up along the course of the corresponding artery. Higher up, the veins become one and ultimately drains in to left renal vein on the left facet and inferior vena cava on the right side. The middle and inferior rectal veins drain in to the interior pudendal vein and thence to the inner iliac vein. Applied Anatomy x the free anastomosis between the superior rectal veins of the portal, the center and inferior rectal veins of the systemic system explains the liver metastases from the genital organ. Middle rectal: It arises both instantly from the anterior division of the inner iliac or in frequent with inferior vesical artery. Internal pudendal artery: It is among the parietal branches of the anterior division of the internal iliac artery. Thereafter, it sends quite a few branches to supply the perineal and vulval buildings, including the vestibular bulb and clitoris. The terminal branches of the artery anastomose with superficial and deep pudendal arteries-branches of the femoral artery. This will assist in maintaining the blood provide of the bladder when the vesical department of the interior iliac artery is ligated. Ovarian artery Each ovarian artery arises from the front of the aorta, slightly beneath the renal artery. It then runs medially alongside the infundibulopelvic ligament to enter the mesovarium. As it enters the hilum of the ovary, it breaks up in to quite a few branches to provide the organ. Branches given to buildings aside from the ovary are: Ureter Uterine tube Round ligament Uterine anastomotic. Superior rectal artery this artery is a continuation of the inferior mesenteric artery and descends right down to the base of pelvic mesocolon. It then divides in to two and each programs down on both side of the rectum to supply it by quite a few branches. One lying horizontally and parallel to the inguinal ligament and the other is placed vertically along the lengthy saphenous vein. The efferents from the superficial inguinal lymph nodes drain in to the deep inguinal nodes and external iliac lymph nodes passing by way of the inguinal canal. Deep inguinal lymph nodes: these nodes obtain afferents from deep femoral vessels, glans clitoris and few from superficial inguinal nodes. The uppermost gland of this group is called the gland of Cloquet or the gland of Rosenm�ller, which lies beneath the inguinal ligament within the femoral canal. Internal iliac nodes obtain afferents from all of the pelvic viscera, deeper perineum, muscle tissue of the thigh and buttock.
Quality innopran xl 80 mg
Fortunately hypertension goals buy discount innopran xl 40 mg on line, the vast majority of sufferers may be helped by using one or more of the cures out there (Table 1 heart attack exo lyrics generic 40 mg innopran xl fast delivery. The majority of patients shall be fitted with a postauricular listening to help which is comparatively unobtrusive. A similar occasion will happen if the mould is incorrectly inserted, as is frequently seen in elderly individuals affected by arthritic joints. Such circumstances may profit from a bone conducting aid worn as a headband with the microphone abutting firmly on to the mastoid. The exterior stimulator units the aid in vibration either throughout the intervening pores and skin or by a direct percutaneous attachment facility. A processor converts speech in to electrical indicators that are transmitted to the electrode. These are: Poor background lighting Sitting in shade Covering face and lips with arms Speaking with cigarette, cigar or pipe in mouth Beard and moustache. The gadget is employed to stimulate any residual cochlear nerve fibres through the electrode implanted within the scala tympani of the cochlea. Manual communication is just possible with each events having the requisite expertise. Lipreading and manual communication Most sufferers with hearing loss requiring aiding will benefit from the development of lipreading abilities. A deafened particular person is best able to lipread if the speaker assists in ensuring sure optimal conditions. This oral method is Environmental aids There are many merchandise available that may assist the deafened affected person in routine day by day life. Local causes of otalgia are often identified by examination of the pinna, ear canal and tympanic membrane. The pathophysiology is a spreading osteomyelitis of the temporal bone brought on by the organism Pseudomonas pyocyaneus. A very handy ear dressing is the otowick, which after insertion in to the ear canal will increase if topical drops are applied. Water exclusion Patent meatus Gross meatal oedema Remove canal debris Insert ear dressing. The eardrum becomes retracted as the tube is blocked, and an inflammatory center ear exudate develops. Pressure within the middle ear produces extreme ache, and the eardrum becomes congested and bulging. Eardrum rupture could then happen, producing a bloodstained discharge with reduction of the pain. Antibiotic therapy of acute otitis media is considerably controversial as many circumstances are of viral origin. After 24�48 hours, if spontaneous decision has not occurred, a broad-spectrum antibiotic to cover Haemophilus and streptococci is indicated. However, suppuration in the mastoid (acute mastoiditis) is severe and potentially life threatening. Upper respiratory tract infections are additionally commonly related to otalgia because of Eustachian tube dysfunction. Acute otitic barotrauma Acute otitic barotrauma might occur throughout descent in plane. It results in severe otalgia and sometimes rupture of the eardrum with a bloody otorrhoea. Herpes zoster oticus (Ramsay Hunt syndrome) the facial nerve ganglion could additionally be affected by shingles. Referred otalgia in adults Dental pathology is a standard explanation for referred otalgia. All these potential peripheral areas have to be examined in all circumstances of referred otalgia. Soft wax can be mistaken for a discharge, however, on the other extreme, every day offensive otorrhoea could also be ignored by some patients with a critical underlying middle ear illness. Chronic suppurative otitis media (tubotympanic disease) Rupture of the tympanic membrane in acute otitis media produces a bloodstained, mucopurulent otorrhoea. Persistent or recurrent mucoid discharge might then happen, especially if water enters the middle ear or in episodes of higher respiratory tract infections. The preliminary treatment of a discharging perforation is aural toilet mixed with topical steroid eardrops. This will dry up most discharging ears so that an Pars tensa perforation Furunculosis Furunculosis (p. Otorrhoea from ear canal disease Acute otitis externa Acute an infection of the exterior ear canal has already been mentioned (p. It is helpful to emphasize that early relapse after remedy with eardrops is usually because of inadequate aural rest room, or colonization of the canal by a secondary fungal progress. Otorrhoea from center ear illness There are two primary types of persistent otitis media. Both produce otorrhoea and hearing loss, and are invariably associated with a defect of the eardrum. One is a mucosal illness; the other Eustachian tube Otorrhoea Chronic otitis externa Chronic otitis externa is usually bilateral and painless, and tends to relapse. Manipulation of the pinna or tragus is painful, and chewing commonly produces discomfort because of the temporomandibular joint inflicting motion of the cartilaginous portion of the exterior ear canal. The otorrhoea is normally profuse and mucoid in the lively infection, and exacerbated by any dysfunction of the Eustachian tube. Attic perforation Cholesteatoma Cholesteatoma (b) Discharging mastoid cavities Many patients have both persistent or recurrent otorrhoea from surgically created mastoid cavities. Uncontrolled an infection of the middle ear or mastoid cavities could over many years predispose to carcinoma. It is invariably accompanied by the development of progressive otalgia and a facial paralysis. Use of antibiotic eardrops is now not recommended routinely as many include ototoxic aminoglycosides. These are associated with cholesteatoma (keratinizing epithelium in the center ear). Because of the dangerous nature of this disease, surgical procedure is invariably recommended. Excision of disease with preservation of listening to involves surgery on the mastoid and middle ear (mastoidectomy; p. The drum defect may be grafted to minimize postoperative mucous discharge and optimize the listening to.
80 mg innopran xl cheap free shipping
Diuretics are a very common trigger due to arrhythmia uti order innopran xl 80 mg mastercard related will increase in distal tubular Na+ supply and distal tubular circulate rate along with hypertension purchase 80 mg innopran xl visa secondary hyperaldosteronism. Thiazides impact plasma K+ focus larger than that of loop diuretics regardless of their lesser natriuretic impact. Finally, several renal tubular toxins trigger renal K+ and magnesium wasting, leading to hypokalemia and hypomagnesemia; these medication include aminoglycosides, amphotericin, foscarnet, cisplatin, and ifosfamide (see also "Magnesium Deficiency and Hypokalemia," later). In consequence, will increase in aldosterone bioactivity and/or features in operate of aldosterone-dependent signaling pathways are related to hypokalemia. Hypertension and hypokalemia as a result of will increase in circulating 11-deoxycorticosterone happen in patients with congenital adrenal hyperplasia attributable to defects in both steroid 11-hydroxylase or steroid 17-hydroxylase; deficient 11-hydroxylase leads to associated virilization and other indicators of androgen extra, whereas reduced sex steroids in 17-hydroxylase deficiency lead to hypogonadism. They might have a rise in urinary calcium excretion, and 20% are hypomagnesemic. Other options embody marked activation of the renin-angiotensin-aldosterone axis. Regardless of the dominant mechanism(s), hypomagnesemic patients are clinically refractory to K+ substitute in the absence of Mg2+ repletion. Notably, magnesium deficiency can also be a standard concomitant of hypokalemia, since many problems of the distal nephron might trigger both potassium and magnesium wasting (Chap. Bicarbonate retention and other acidbase results of hypokalemia can contribute to the technology of metabolic alkalosis. Hypokalemia also predisposes to acute kidney damage and can lead to end-stage renal illness in sufferers with long-standing hypokalemia as a result of eating issues and/or laxative abuse. Correction of hypokalemia is especially important in hypertensive patients treated with diuretics, in whom blood strain improves with the establishment of normokalemia. Diagnostic approach the cause for hypokalemia is normally evident from history, physical examination, and/or primary laboratory tests. The presence of a non-anion-gap acidosis suggests a distal, hypokalemic renal tubular acidosis or diarrhea; calculation of the urinary anion gap might help differentiate these two diagnoses. Renal K+ excretion may be assessed with a 24-h urine collection; a 24-h K+ excretion of <15 mM is indicative of an extrarenal cause of hypokalemia. The urgency of remedy is decided by the severity of hypokalemia, associated scientific factors (cardiac illness, digoxin remedy, and so forth. When excessive activity of the sympathetic nervous system is thought to play a dominant function in redistributive hypokalemia, as in thyrotoxic periodic paralysis, highdose propranolol (3 mg/kg) must be thought of; this nonspecific -adrenergic blocker will right hypokalemia without the danger of rebound hyperkalemia. Potassium bicarbonate or potassium citrate must be thought of in sufferers with concomitant metabolic acidosis. Notably, hypomagnesemic sufferers are refractory to K+ substitute alone, so concomitant Mg2+ deficiency ought to at all times be corrected with oral or intravenous repletion. The deficit of K+ and the rate of correction ought to be estimated as accurately as attainable; renal operate, medications, and comorbid conditions such as diabetes must be considered to gauge the risk of overcorrection. In the absence of abnormal K+ redistribution, the whole deficit correlates with serum K+ in order that serum K+ drops by approximately zero. However, because of the difficulty in assessing the deficit precisely, plasma K+ concentration should be monitored fastidiously throughout repletion. The use of intravenous administration should be restricted to sufferers unable to utilize the enteral route or in the setting of severe problems (paralysis, arrhythmia, and so forth. Intravenous K+-Cl� should always be administered in saline solutions rather than dextrose because the dextrose-induced increase in insulin can acutely exacerbate hypokalemia. The peripheral intravenous dose is normally 20�40 mmol of K+-Cl� per liter; larger concentrations may cause localized ache from chemical phlebitis, irritation, and sclerosis. Femoral veins are preferable, since infusion through inner jugular or subclavian central strains can acutely improve the local concentration of K+ and have an result on cardiac conduction. These measures may embody minimizing the dose of non-K+-sparing diuretics, restricting Na+ consumption, and using clinically appropriate combinations of nonK+-sparing and K+-sparing medicines. Cellular efflux: thrombocytosis, erythrocytosis, leukocytosis, in vitro hemolysis B. Lysine, arginine, and e-aminocaproic acid (structurally related, positively charged) G. Succinylcholine; thermal trauma, neuromuscular harm, disuse atrophy, mucositis, or prolonged immobilization H. Inhibition of the renin-angiotensin-aldosterone axis; threat of hyperkalemia when utilized in mixture 1. Blockade of the mineralocorticoid receptor: spironolactone, eplerenone, drospirenone 5. Although redistribution and reduced tissue uptake can acutely cause hyperkalemia, a lower in renal K+ excretion is the most common underlying cause (Table 6-5). Excessive consumption of K+ is a uncommon trigger due to the adaptive capability to enhance renal secretion; however, dietary consumption can have a significant effect in susceptible patients. Drugs that have an effect on the renin-angiotensin-aldosterone axis are additionally a serious explanation for hyperkalemia. Pseudohyperkalemia can happen in the setting of excessive muscle activity during venipuncture (fist clenching, etc. Cooling of blood after venipuncture is one other trigger, because of lowered mobile uptake; the converse is the increased uptake of K+ by cells at high ambient temperatures, resulting in regular values for hyperkalemic sufferers and/or to spurious hypokalemia in normokalemic sufferers. Finally, there are multiple genetic subtypes of hereditary pseudohyperkalemia attributable to will increase within the passive K+ permeability of erythrocytes. Redistribution and hyperkalemia Several different mechanisms can induce an efflux of intracellular K+ and hyperkalemia. Hyperkalemia because of hypertonic mannitol, hypertonic saline, and intravenous immunoglobulin usually is attributed to a "solvent drag" effect as water strikes out of cells alongside the osmotic gradient. Cationic amino acids-specifically lysine, arginine, and the structurally related drug e-aminocaproic acid-cause efflux of K+ and hyperkalemia via an effective cation-K+ exchange of unknown id and mechanism. Structurally related glycosides are present in specific vegetation (yellow oleander, foxglove, and so forth. Hyperkalemia due to extra consumption or tissue necrosis Increased intake of even small amounts of K+ might provoke severe hyperkalemia in patients with predisposing components; therefore, an assessment of dietary intake is essential. Foods wealthy in potassium embody tomatoes, bananas, and citrus fruits; occult sources of K+, significantly K+containing salt substitutes, additionally could contribute significantly. Iatrogenic causes embrace easy overreplacement with K+-Cl� and the administration of a potassiumcontaining medicine. Finally, tissue necrosis, as in acute tumor lysis syndrome and rhabdomyolysis, predictably causes hyperkalemia from the discharge of intracellular K+. Hyporeninemic hypoaldosteronism is a quite common predisposing think about a number of overlapping subsets of hyperkalemic patients: diabetic patients, the aged, and sufferers with renal insufficiency. Renal disease and hyperkalemia Chronic kidney disease and end-stage kidney illness are very common causes of hyperkalemia due to the related deficit or absence of functioning nephrons. Medication-associated hyperkalemia Most drugs related to hyperkalemia trigger inhibition of some element of the renin-angiotensinaldosterone axis. Notably, most medication that affect the reninangiotensin-aldosterone axis additionally block the local adrenal response to hyperkalemia, thus attenuating the direct stimulation of aldosterone launch by elevated plasma K+ concentration. Clinical options Hyperkalemia is a medical emergency because of its effects on the center. Cardiac arrhythmias related to hyperkalemia embody sinus bradycardia, sinus arrest, gradual idioventricular rhythms, ventricular tachycardia, ventricular fibrillation, and asystole.

Buy generic innopran xl 40 mg
Idiopathic central diabetes insipidus is associated with selective destruction of the vasopressin-secreting neurons in the supraoptic and paraventricular nuclei and could be inherited as an autosomal dominant trait or occur spontaneously blood pressure medication with little side effects innopran xl 40 mg order. A plasma vasopressin stage is really helpful as one of the best technique for distinguishing between central and nephrogenic diabetes insipidus blood pressure medication and ed order innopran xl 80 mg amex. Fogo Key diagnostic options of selected ailments in renal biopsy are illustrated, with mild, immunofluorescence, I Eric G. In minimal-change disease, gentle microscopy is unremarkable (A), whereas electron microscopy (B) reveals podocyte damage evidenced by complete foot course of effacement. There is a well-defined segmental improve in matrix and obliteration of capillary loops, the sine qua non of segmental sclerosis not in any other case specified (nos) sort. There is segmental collapse of the glomerular capillary loops and overlying podocyte hyperplasia. This lesion typically happens as a secondary response when nephron mass is misplaced as a result of. There is segmental sclerosis of the glomerular capillary loops at the proximal tubular outlet (arrow). Membranous glomerulopathy is as a result of of subepithelial deposits, with resulting basement membrane response, resulting in the look of spikelike projections on silver stain (A). By electron microscopy, the subepithelial location of the deposits and early surrounding basement membrane response is obvious, with overlying foot process effacement (C). By immunofluorescence, chunky irregular mesangial and capillary loop deposits are evident, with a few of the peripheral loop deposits having a easy, molded outer contour as a result of their subendothelial location. These deposits usually stain for all three immunoglobulins (IgG, IgA, IgM) and both C3 and C1q (B). By electron microscopy, subendothelial, mesangial, and rare subepithelial dense immune complicated deposits are evident, together with in depth foot course of effacement (C). This pauciimmune necrotizing crescentic glomerulonephritis reveals quite a few breaks within the glomerular basement membrane with related segmental fibrinoid necrosis, and a crescent fashioned by proliferation of the parietal epithelium. Amyloidosis reveals amorphous, acellular enlargement of the mesangium, with material usually also infiltrating glomerular basement membranes, vessels, and within the interstitium, with apple-green birefringence by polarized Congo pink stain (A). The deposits are composed of randomly organized 9- to 11-nm fibrils by electron microscopy (B). Monoclonal light chains precipitate in tubules and result in a syncytial big cell reaction surrounding the casts, and a surrounding continual interstitial nephritis with tubulointerstitial fibrosis. There is mesangial growth, usually nodular by mild microscopy (A), with immunofluorescence showing monoclonal staining, extra generally with kappa than lambda mild chain, of tubules (B) and glomerular tufts. By electron microscopy (C), the deposits present an amorphous granular look and line the within of the glomerular basement membrane and are also found along the tubular basement membranes. These deposits may be immediately visualized by electron microscopy (B), where the glycosphingolipid appears as whorled so-called myeloid our bodies, particularly within the podocytes. In barely extra advanced stages, more marked mesangial growth with early nodule formation develops, with evident arteriolar hyaline (B). There are characteristic intraglomerular fibrin thrombi, with a chunky pink appearance (thrombotic microangiopathy). The remaining portion of the capillary tuft reveals corrugation of the glomerular basement membrane due to ischemia. Cholesterol emboli trigger cleft-like areas the place the lipid has been extracted during processing, with easy outer contours, and surrounding fibrotic and mononuclear cell reaction in these arterioles. There is in depth interstitial lymphoplasmocytic infiltrate with delicate edema and associated tubular harm (A), which is frequently associated with interstitial eosinophils (B) when attributable to a drug hypersensitivity reaction. Calcium oxalate crystals have triggered intensive tubular harm, with flattening and regeneration of tubular epithelium (A). There is extensive acute tubular harm with intratubular nonpolarizable calcium phosphate crystals. There is chronic interstitial nephritis with numerous, confluent, non-necrotizing granulomas. While this amount of protons, 40�60 mmol/d, is small, it have to be secreted to stop continual optimistic H+ stability and metabolic acidosis. The metabolic and respiratory parts that regulate systemic pH are described by the Henderson-Hasselbalch equation: pH = 6. More complicated scientific situations can provide rise to blended acid-base disturbances. Nevertheless, manufacturing and excretion are once more matched at a new steady-state Paco2. Physiologic compensation can be predicted from the relationships displayed in Table 5-1. Shown are the 90% confidence limits (range of values) of the normal respiratory and metabolic compensations for major acid-base disturbances. When metabolic acidosis and metabolic alkalosis coexist in the identical patient, the pH could also be regular or close to normal. Care ought to be taken when measuring blood gases to get hold of the arterial blood pattern without utilizing extreme heparin. After verifying the blood acid-base values, the precise acid-base disorder can then be identified. For example, patients with metabolic acidosis because of alcoholic ketoacidosis might develop metabolic alkalosis due to vomiting and superimposed respiratory alkalosis as a outcome of the hyperventilation of hepatic dysfunction or alcohol withdrawal. For instance, an alcoholic who has been vomiting may develop a metabolic alkalosis with a pH of 7. A combination of high-gap acidosis and metabolic alkalosis is recognized easily by evaluating the differences (values) within the regular to prevailing patient values. The fall in blood pH is accompanied by a attribute enhance in air flow, particularly the tidal quantity (Kussmaul respiration). Unrecognized bowel ischemia or infarction in a patient with extreme atherosclerosis or cardiac decompensation receiving vasopressors is a standard cause of lactic acidosis. Alkali therapy is mostly advocated for Chronic alcoholics can develop ketoacidosis when alcohol consumption is abruptly curtailed and diet is poor. As the circulation is restored by administration of isotonic saline, the preferential accumulation of -hydroxybutyrate is then shifted to acetoacetate. This explains the frequent clinical remark of an more and more optimistic nitroprusside response because the patient improves. Excessive insensible fluid losses may trigger extreme volume depletion and hypernatremia. If renal failure prevents rapid clearance of salicylate, hemodialysis may be performed towards a bicarbonate dialysate. Hypophosphatemia, hypokalemia, and hypomagnesemia might coexist and must be corrected. Hypophosphatemia normally emerges 12�24 h after admission, may be exacerbated by glucose infusion, and, if severe, might induce rhabdomyolysis. Upper gastrointestinal hemorrhage, pancreatitis, and pneumonia may accompany this disorder. Under most physiologic conditions, sodium, urea, and glucose generate the osmotic pressure of blood.
Innopran xl 80 mg order mastercard
Stage of Vascularization Within 24 hours of rupture of the follicle heart attack reasons discount 80 mg innopran xl fast delivery, small capillaries develop in to granulosa layer in path of the lumen accompanied by lymphatics and fibroblasts blood pressure information purchase innopran xl 80 mg online. Approximately about 7�8 days following ovulation, the corpus luteum attains a dimension of about 1�2 cm and reaches its secretory peak. The cells persist within the periphery and within the septa and are called paralutein cells. The lutein cells turn into greatly enlarged and develop lipid inclusion, giving the cells a distinctive yellowish shade. There is deposition of fats in the lutein cells and appearance of hyaline tissue between them. Adequate folliculogenesis within the preovulatory phase with increased secretion of estradiol and of 17-hydroxy progesterone is a prerequisite for adequate corpus luteum formation. Regression occurs following low levels of chorionic gonadotropin and the degenerative adjustments happen most regularly at about 6 months of gestation. Hormone secretion Hormones-predominantly progesterone is secreted by the corpus luteum to support the endometrium of the luteal phase. It has been suggested that prostaglandin F2 liberated from the ovary is luteolytic. Note the tendency of tortuosity of the glands and the characteristic subnuclear vacuolation in early secretory part (cf compare with those of proliferative phase) Chapter 8 Menstruation inhibin and relaxin. Progesterone along with estrogen from corpus luteum preserve the expansion of the fertilized ovum. This flip over of function from corpus luteum of being pregnant to placenta known as lutealplacental shift. However, the following descriptions are associated to atretic changes of a maturing follicle which is finally ignored in the race of a dominant follicle. Note the marked tortuosity of the glands with secretion within the lumen within the midsecretory section. After shedding of the superficial half during menstruation, the regeneration of all of the components occurs from this zone. The cubical surface epithelium is derived from the gland lumina and stromal cells. The glands and the stromal cells are regenerated from the remnants left within the basal zone. There is proliferation of all the elements-at first slowly however in a while at a speedy pace. Hyaline tissue is deposited beneath the membrana granulosa to form the glass membrane which is the traditional characteristic of follicular degeneration. Liquor folliculi is steadily absorbed with growing formation of hyaline tissue within the glass membrane. Eventually, the follicle collapses; its cavity is obliterated when the opposing surfaces of the glass membranes are available in contact. In the periphery, deep staining theca interna cells persist and are called interstitial cells of the ovary. The following are the attainable explanations for follicular degeneration and atresia: Oogonia having no granulosa cell layer envelope. Two distinct divisions are established- basal zone (stratum basalis) and the superficial useful zone. Chapter 8 Menstruation under the epithelium the place they type loose capillary community. The endometrium incorporates receptors for progesterone that are induced by estrogen. Thus, the progesterone can only act on the endometrium previously primed by estrogen. There is appearance of vacuoles because of secretion of glycogen between the nuclei and the basement membrane. This known as subnuclear vacuolation, which is the earliest (36�48 hours) evidence of progesterone effect (ovulation). The intracellular secretion then enters the gland lumina on the way in which to the uterine cavity pushing the nuclei again in the path of the basement membrane. The fluid has got nutritive worth for any fertilized ovum reaching the uterus during that point. The deeper spongy layer is composed of convoluted glands, coiled arterioles and relatively few stromal cells in edematous stroma. Histological staining is eosinophilic the thickness of the endometrium reaches its highest (6�8 mm). The endometrial progress ceases 5�6 days previous to menstruation (22nd or twenty third day of cycle) in an infertile cycle. The regressive adjustments in the endometrium are pronounced 24�48 hours prior to menstruation. There is marked spiralling of the arteries and the withdrawal of hormones estrogen and progesterone causes intense spasm of the spiral arterioles on the basal half. Regression of corpus luteum with fall in the degree of estrogen and progesterone is an invariable previous feature. Stasis of blood and spasm of the arterioles result in damage of the arteriolar partitions. Phase of rest leads to escape of blood out of the vessels by way of the broken partitions. The degenerative process is rapid and entails all of the elements of the useful damaged layer. There is local tissue destruction by release of proteolytic enzymes from the breakdown of lysosomes. The bleeding happens from the broken arteries, veins and capillaries and likewise from the stromal hematoma. The blood along with the superficial useful layer is shed in to the uterine cavity. Granulosa cells now utilize the increased androgen produced from the theca cells for the synthesis of estrogen. It stimulates aromatase activity and progesterone synthesis within the granulosa cells. The menstrual flow stops as a result of mixed effect of prolonged vasoconstriction, myometrial contraction and local aggregation of platelets with deposition of fibrin around them. Endothelin and platelet activating issue present in the endometrium are potent vasoconstrictors. Resumption of estrogen secretion results in clot formation over the decapitated stumps of endometrial vessels. The endometrium and partly the myometrium, synthesize the prostaglandins from arachidonic acid by the enzyme cyclo-oxygenase. Thus, the menstrual ache and blood flow are most likely related to the relative proportion of various prostaglandins present within the endometrium. The lysis of the corpus luteum happens and so the secretion of progesterone and estrogen falls. In the luteal part, progesterone acts on the estrogen primed endometrium having sufficient number of receptors and produces secretory adjustments.