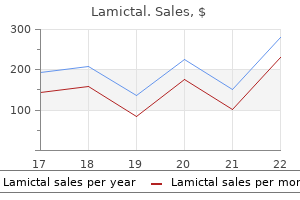
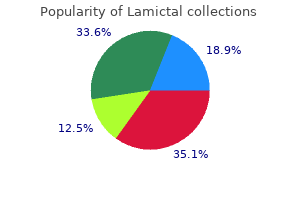
Lamictal
Lamictal dosages: 200 mg, 100 mg, 50 mg, 25 mg
Lamictal packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

25 mg lamictal order visa
The aircraft between the transversalis fascia and peritoneum is developed with blunt dissection, and the parietal peritoneum is freed from the lateral belly wall treatment for depression discount 25 mg lamictal with amex. The abdominal contents and peritoneum, together with the kidney and ureter, are mirrored medially to show the ventral lumbar backbone medications john frew lamictal 200 mg purchase with amex. Dissecting the peritoneum off the ventral abdominal wall permits full mobilization of the peritoneal contents. The the rest of the dissection is just like the ventrolateral retroperitoneal method. TranspsoasApproach(L1-5) In recent years the field of minimally invasive surgery has expanded to contain surgical approaches to the spine as surgeons and sufferers seek novel methods to reduce tissue trauma throughout surgical procedure, lessen postoperative discomfort, and shorten hospital stays. To this finish, a novel approach via the psoas muscle offers a lateral method that might be completed through one or two small (3- to 4-cm) incisions using tubular retractors and avoids the need for either a transperitoneal or retroperitoneal anterior strategy. A second mark is made posteriorly at the border between the erector spinae and abdominal oblique muscles. Blunt dissection is used to unfold the muscle fibers until the retroperitoneal house is reached. The index finger is then used to sweep the peritoneum anteriorly while palpating down to the psoas muscle. Alternatively, a single, barely larger incision may be made in the flank via the muscle layers and blunt retroperitoneal dissection used to dissect medially to the psoas muscle. The dissection happens between the center and anterior third of the psoas muscle to keep away from the lumbar plexus, which lies dorsally. Sequentially larger dilators are introduced through the psoas muscle to the annulus of the disk, adopted by the retractor blades. If no response is obtained with careful stimulation, the muscle may then be divided and, if needed, eliminated throughout the confines of the retractor. When the surface of the disk is exposed, the position of the retractor is reconfirmed by fluoroscopy. Further retraction, if needed, must be directed anteriorly to prevent further strain on the posterior portion of the psoas and the neural components inside it. On closure the retractor blades are removed slowly while hemostasis is rigorously confirmed, and the 2 small incisions closed in the usual fashion. The distal limit of the transpsoas method is determined by the peak of the iliac crest. Access to more than two adjacent intervertebral disks requires further incisions. The superior hypogastric plexus is the terminal extension of the preaortic sympathetic plexus. This nice, skinny collection of nerves is most commonly found arching over the left iliac artery crossing the L5-S1 disk house. The superior hypogastric plexus offers innervation to the interior vesicle sphincter; injury to those nerves can result in retrograde ejaculation. Great care must due to this fact be taken in clearing prevertebral tissue from the ventral L5-S1 disk house. The use of electrocautery superficial to the anterior longitudinal ligament is avoided. All prevertebral tissues, together with the hypogastric plexus, are bluntly swept to the proper. The middle sacral artery and vein are recognized inferior to the aortic bifurcation and are ligated and divided. L4-5 is best approached laterally to the vessels as a outcome of the origin of the vena cava and the bifurcation of the aorta are sometimes ventral to L5. If the origins of the vena cava and aortic bifurcation are abnormally excessive, an interiliac method could additionally be attempted. The iliolumbar vein should also be recognized, ligated, and divided throughout exposure of L4-5 to permit medial retraction of the iliac vein and entry to the disk space. Once the procedure is completed, the stomach contents are returned to their regular anatomic place, and the fascial and muscular layers are closed separately. When the spinal process is completed, the posterior peritoneum is closed with absorbable suture. The abdominal contents are then returned to their anatomic position to forestall intestinal torsion and obstruction. The individual fascial and muscular layers are reapproximated with absorbable sutures. This component resists the compressive forces created by axial loading of the lumbar spine. Their effect on lateral flexion is variable and is decided by the scale and shape of their interfaces with the vertebral end plates. To obtain larger rigidity of the general construct, fixation of the vertebral bodies is usually performed. This may be both with anterior vertebral fixation with a screw rod or plate instrumentation, or posterior pedicle screw fixation. Pedicle fixation is mentioned elsewhere; so the focus of this transient discussion is structural anterior interbody grafting and anterior vertebral fixation. Most anterior lumbar fixation constructs are variations on the rigid cantilever beam design. The screws are hooked up rigidly to longitudinal members, usually both a rod or a plate. Similar to the interbody grafts, the cantilever beam assemble functions in distraction most of the time by resisting compressive forces. Because of its rigid attachment to the vertebrae, nonetheless, it additionally resists extension, axial rotation, and lateral bending. Ideally, the axial compressive forces (load) ought to be shared between the cantilever beam instrumentation and the interbody graft. If extreme drive is borne by the instrumentation, the bone graft material may resorb and a pseudarthrosis might end result. The interbody graft or gadget ought to due to this fact be placed beneath gentle compression. Care must be taken, however, if compression is directly utilized to the instrumentation; important ventrolateral compression can create a segmental kyphosis or scoliosis. Anterior lumbar instrumentation, together with the usage of appropriately sized and positioned grafts, can successfully appropriate some spinal deformities. Small grafts positioned within the ventral disk space or larger lordotic grafts covering most of the vertebral end plates can enhance segmental lordosis and proper a relative or frank kyphosis. Correction of a lumbar scoliosis can be achieved through the placement of small structural grafts in the concavity of the intervertebral disk spaces and compressing throughout lateral vertebral physique screws. Proper graft selection and placement are important in this scenario to keep away from simultaneously creating a relative lumbar kyphosis through ventral compression. A kyphoscoliosis or important kyphotic deformity is a relative contraindication to an anterior-only correction procedure. Higher lumbar ranges may be uncovered however appreciable vessel retraction could also be required.
Discount lamictal 50 mg
The practice of initiating oral agents59,113,121 after a chronic course of intravenous antibiotics is widespread for osteomyelitis in varied areas but finds little support from any comparative evaluation of their efficacy in treating spinal infections treatment uti infection lamictal 25 mg discount with visa. In sufferers with outstanding disk space or bone infection, spontaneous fusion on the affected level might occur treatment brachioradial pruritus order lamictal 100 mg fast delivery. Radiographic findings respond very slowly to profitable remedy, in distinction to the scientific response, and are therefore not immediately useful in assessing the response to therapy. Infections have been reported in neonates123 and infants124,a hundred twenty five and occur throughout childhood into early adolescence. The predilection for these infections seems to be a results of the frequent bacteremia that happens in childhood. The distinct sample of infection is thought to outcome from the peculiarities of the pediatric spinal vascular anatomy. Until the age of about 7 years, profuse anastomoses exist between the intraosseous spinal arteries and thereby stop devascularization and infarction of enormous parts of the metaphysis when septic emboli occlude a metaphyseal artery. This tends to limit the extent of metaphyseal and osseous infection to the cartilaginous finish plate at either end of the vertebra. Hence, hematogenous spread to the pediatric spine tends to be limited more to the disk area. Additionally, the pediatric disk retains vascularity, in distinction to disks in adults, and infrequently blood-borne pathogens might lodge instantly in the disk space in children with none involvement of the metaphyseal end plates. It has been postulated that some cases could happen secondary to partial dislocation of the epiphysis because of a hyperflexion damage. Nonetheless, a few of these sufferers may show substantial improvement in neurological function over time, thus justifying an aggressive therapeutic stance even when extreme deficits are encountered. In sufferers in whom no organisms are isolated, management with immobilization alone could additionally be reasonable, however patients managed in this method ought to be monitored intently for medical and radiographic evidence of decay. In all instances during which an infection is suspected or confirmed, applicable antibiotic therapy based on the outcomes of culture ought to be initiated. In the long run, these sufferers could additionally be at excessive threat for the event of block vertebrae and vertebrae magnae. The prevalence and management of most of those infections are significantly affected by whether or not instrumentation and bone grafting have been carried out. The true scope of the time period "iatrogenic" additionally consists of infections resulting from hematogenous inoculation of the spine precipitated by the manipulation of a remotely contaminated or contaminated web site, corresponding to dental manipulation, urologic instrumentation, or drainage of a noncontiguous abscess. Infections resulting from such iatrogenic bacteremia are similar in most aspects to "spontaneous" pyogenic infections, which are mentioned in the first part of this chapter. The present discussion deals specifically with infections that result from direct spinal interventions. These procedures can render the backbone susceptible to infection by the implantation of instrumentation, devascularized bone graft, suture, or hematoma and by the creation of ischemic or necrotic tissue via dissection and retraction. Infections after Surgery with out Instrumentation or Bone Grafts the incidence of an infection after lumbar laminectomy or diskectomy is roughly 1%. Infection often occurs after intraoperative contamination,147 and the everyday causative organisms are pores and skin flora- generally S. Rarely, nonetheless, gram-negative organisms and anaerobes could produce fulminant infections within the surgical mattress. A historical past of a small quantity of drainage soon after surgical procedure is occasionally obtained. However, each the acute-phase reactants and the imaging adjustments have to be distinguished from the expected postoperative changes. Measurement of a specific acute-phase reactant, such as elastase� 1-proteinase inhibitor, doubtlessly allows the detection of an an infection even earlier, but it has not been proven to be related outdoors of a research setting. Depending on the number of ranges operated on and the dimensions of the postoperative fluid collection, the an infection may be managed either with antibiotics alone or with surgical d�bridement as well as. Postoperative Spinal Infections Postoperative spinal infections can often be catastrophic occasions that lead to extended (and expensive) hospital stays and vital long-term disability. In collection reported after the advent of Harrington instrumentation, the an infection fee rose to between 1% and 12%, with a mean of 6%. Contamination of the surgical wound by pores and skin commensals happens in as many as half of all surgical cases. Patient factors that predispose to an infection include earlier surgical procedure, earlier irradiation, preexisting neoplasm, chronic steroid therapy, diabetes, malnutrition, paraplegia, smoking, rheumatoid arthritis, nutritional state, and intercurrent infection. The use of Bovie monopolar cauterization has been implicated in an elevated threat for postoperative infection. Instrumentation offers quick spinal stabilization, early mobilization of the patient, and the next price of bone fusion. Data demonstrating the impact of instrumentation on the chance for postoperative infection first turned out there with the series of Harrington rod instrumentation. Prolonged retraction is known to trigger disruption of regular muscle physiology and compromise of perfusion, so the length and extent of retraction should be minimized. The causative organism can usually be cultured from the wound if materials for culture is obtained earlier than starting antibiotic remedy. Distinction must be made between early infections which are limited to the pores and skin and subcutaneous tissue and those who extend beneath the fascia. Superficial infections usually occur in obese sufferers with large amounts of subcutaneous fats and in these with impaired wound healing. Such infections necessitate thorough d�bridement of the wound, removal of suture material and necrotic tissue, and intravenous antibiotic remedy. To accomplish this, some surgeons advocate the utilization of continuous suction-irrigation methods to deliver antibiotics to the wound. This method is regularly successful, though long-term oral suppressive antibiotic therapy may be essential. Such infections are nearly always attributable to indolent organisms such as Propionibacterium acnes, S. If sufficient time has elapsed since bone grafting and rigid bone fusion is found at surgical procedure, a case may be made for removing of the infected hardware. It has been shown, nonetheless, that if the intraoperative tissue cultures are maintained within the laboratory for at least 7 days, slow-growing organisms corresponding to those listed earlier can be isolated. Additionally, the glycocalyx prevents really representative organisms from detaching in sufficient numbers to be detected by easy aspiration and culture. Because such infections usually occur late, elimination of the instrumentation might not compromise the bony fusion. Hardware removing is the most effective way of eradicating the glycocalyx and thereby the nidus of the infection. Management is chiefly medical, with antibiotics tailored to the staphylococcal species, the commonest causative organisms, or to the culture outcomes if an organism can be aspirated from the disk.
Diseases
- Light chain disease
- Mixed connective tissue disease
- Osteosclerose type Stanescu
- Mental retardation short stature ocular and articular anomalies
- Scleredema
- Chromosome 3, Trisomy 3q2
- Fetal minoxidil syndrome
- Thrombocytopenia Robin sequence
- Sex chromosome disorders
- CATCH 22 syndrome
Cheap 100 mg lamictal with mastercard
Sublaminar wiring around C1 and below requires visualization of the underlying dura, which is achieved by making laminotomies and removing the ligamentum flavum symptoms 8 days after ovulation generic lamictal 25 mg otc. The lamina can be notched the place the wire is handed to optimize visualization of the dura medicine woman cast purchase lamictal 50 mg line. The wire is passed under the lamina by feeding and pulling simultaneously to prevent neurological damage. Facet wiring may be performed if decompression with a laminectomy is indicated and requires the facet joints to be opened and the articular cartilage to be removed. A drill gap is made at a 90-degree angle to the inferior facet and the wire is passed by way of the opening. Facet wiring alleviates the chance of neurological harm related to sublaminar wires. However, each os odontoideum and odontoid agenesis could result in incompetence of the cruciate ligament, leading to subsequent atlantoaxial instability. These patients should remain in a flat or semirecumbent place whereas present process awake fiberoptic endotracheal intubation to attenuate the risk of neurological harm. Preparation for intraoperative somatosensory and brainstem auditory evoked potentials for steady monitoring throughout the operation is completed earlier than positioning. Evoked potentials are measured following induction of general anesthesia and compared with those measured after the patient is placed prone. The patient is fastidiously placed in the prone place and craniocervical alignment is assessed with fluoroscopic steerage before removal of any cervical orthosis. Recent studies counsel that positioning sufferers with cervical instability may be safer on a rotating mattress rather than with conventional logrolling. The skin and subcutaneous tissue are incised right down to the dorsal fascia, followed by improvement of an avascular midline airplane between the paraspinal muscle tissue. Soft tissue dissection is sustained until the occipital squamosa, foramen magnum, and posterior components of the primary three cervical vertebrae are clearly uncovered. The exposure ought to extend to the lateral margin of the aspect joints bilaterally, whereas the occipital floor ought to be broad sufficient to help the chosen construct. All gentle tissue should be meticulously removed from the bony surfaces of the segments chosen, adopted by use of a high-speed bur drill to decorticate these similar ranges to promote fusion before placement of instrumentation. Steinmann Pin Fusion Sonntag and Dickman43,forty four have described a rod and wire method using a contoured 5 32-inch diameter threaded Steinmann pin. After acquiring the specified curvature and length, the pin is wired to the occiput and cervical lamina or aspects. If a suboccipital craniotomy or cervical laminectomy is carried out, a plate of cortical iliac crest bone is wired to the central portion of the pin to protect the positioning of decompression. Although these strategies are technically simple and require no special intraoperative gear, corresponding to fluoroscopy, all of them require inflexible postoperative immobilization to acquire successful fusion. Occipital screw placement requires each cautious measurement of the thickness of the occipital bone and identification of the proximity of the dural sinuses preoperatively. Anatomic studies44-47 evaluating occipital bone morphology have proven that the occipital protuberance is the world of biggest bone thickness and was consistently situated midline on the superior nuchal line. The bone thickness additionally decreases radially in both lateral and inferior directions from the occipital protuberance. Haher and associates45 examined the pullout strength of unicortical and bicortical screws relative to occipital bone morphology and reported that on common, the pullout power of bicortical fixation was 50% higher that unicortical screw fixation. However, unicortical screw pullout power at the occipital protuberance was not considerably totally different than that of bicortical screws at different anatomic places. Zipnick and associates47 confirmed that the outer cortex contributed 45% of the entire thickness of the occipital bone but the inside cortex solely contributed 10%, so unicortical fixation on the occipital protuberance might offer acceptable pullout power to secure the occiput to prevent the complications of bicortical screw placement. Gallie Fusion In 1930, Gallie5 first described the stabilization of a subluxed atlantoaxial complex by utilizing a sublaminar wire positioned around the posterior arch of C1 and looped around the spinous process of C2, holding in place a median bone graft notched over the spinous means of C2. Although the process is technically easy, it stays the poorest biomechanical assemble, subsequently requiring supplementation with different techniques. Brooks-Jenkins Fusion the Brooks-Jenkins fusion uses doubled 20-gauge wires, that are passed underneath the laminae of the atlas and axis bilaterally. Two posterolateral autologous iliac crest bone grafts are beveled in to each interlaminar areas and held in place with the overlying wire. A single bicortical bone graft is fit into the interlaminar space by wiring the C1-2 interlaminar house and notched to accommodate the spinous process of C2. This technique offers elevated stability without using two ranges of sublaminar wires seen in the Brooks-Jenkins approach. To acquire optimal anatomic realignment, patients are kept in a halo vest preoperatively and intraoperatively. The C1-2 interlaminar house is widened with a high-speed bur drill and the spinous course of and lamina of C2 are decorticated. Iliac crest graft (4 cm long) is formed to suit the interlaminar house, putting the concave cortical floor towards the dura. The inferior facet of the graft is notched to lie over the spinous means of C1 and two strands of no. Patients are beneficial to remain in a halo for three months postoperatively, and then changed to a hard collar for 4 to six weeks thereafter. Inside-Outside Technique In 1999 Pait and associates48 addressed the problems of outside-inside screw fixation by creating an progressive modification to previous methods. Their inside-outside method uses lateral mass plating with a cranial bolt that connects the plate to the cervical portion of the construct. The occipitocervical plate is held in place to mark the location of the cranial bolt. An elliptic bur gap is then made approximately 1 cm superior to the marked cranial bolt location. The bur hole is linked to the placement of the cranial bolt by drilling a trough the same width because the bolt. The bolt (or flathead screw) is then positioned within the bur hole with the threads going through outward and slid down the trough to the designated location. The plate is placed over the bolt and loosely held in place with nuts to safe the screws until the specified cervical stabilization is done before completion of the occipitocervical fusion. Rigid Screw Fixation Previous wiring strategies introduce the risk of neurological harm by passage of the wire adjacent to unprotected dura, and in some sufferers with incompetent or absent cervical lamina, may show to be a suboptimal methodology of stabilization. Therefore, over the previous decade, rigid fixation with plate-screw or screw fixation with rod constructs have been studied and popularized. Biomechanical studies41-43 also suggest superiority of screwbased fixation over wiring-based stabilization strategies. Increased rigidity of screw-based constructs present resistance to fatigue and vertical settling, whereas permitting fusion over fewer segments and lowering the size of exterior immobilization after surgical procedure.
Lamictal 50 mg order with visa
Numerous studies have demonstrated that irreversible muscle harm happens on account of muscle stripping and retraction and could be associated with poor medical outcomes treatment rosacea generic 50 mg lamictal with mastercard. Contemporary advances in interbody gadgets and instrumentation techniques, particularly within the minimally invasive extent, have endowed the modern-day spine surgeon with an expanded armamentarium to provide circumferential fusion via anterior, posterior, and transforaminal routes medicine vs nursing 50 mg lamictal order fast delivery. Allograft implants for posterior lumbar interbody fusion: results evaluating cylindrical dowels and impacted wedges. Minimally invasive transforaminal lumbar interbody fusion: indications, technique, and issues. Comparison of the mini-open versus laparoscopic method for anterior lumbar interbody fusion: a retrospective review. Transforaminal lumbar interbody fusion: technique, issues, and early outcomes. Comparison of two interbody fusion cages for posterior lumbar interbody fusion in a cadaveric model. Kalfas Image-guided spinal navigation is a computer-based surgical expertise designed to improve intraoperative orientation to the unexposed anatomy throughout complex spinal procedures. Stereotaxy is outlined because the localization of a selected level in area utilizing three-dimensional coordinates. However, the evolution of computer-based technologies has eradicated the necessity for this frame and has allowed for the enlargement of stereotactic technology into other surgical fields, specifically, spinal surgical procedure. The management of complex spinal disorders has been tremendously influenced by the increased acceptance and use of spinal instrumentation gadgets in addition to the development of more complex operative exposures. In particular, the various fixation strategies that require placing bone screws into the pedicles of the thoracic, lumbar, and sacral backbone into the lateral lots of the cervical spine and across joint spaces within the higher cervical spine require visualization of the unexposed spinal anatomy. Consequently, the surgeon is required to extrapolate the third dimension based on an interpretation of the images and information of the pertinent anatomy. This so-called useless reckoning of the anatomy can end result in varying levels of inaccuracy when inserting screws into the unexposed spinal column. Several studies have proven the unreliability of routine radiography in assessing pedicle screw placement within the lumbosacral backbone. The rate of disruption of the pedicle cortex by an inserted screw ranges from 21% to 31% in these research. Although the lateral view can be comparatively simple to evaluate, the anteroposterior or oblique view may be tough to interpret. This aircraft finest demonstrates the position of the screw relative to the neural canal. This study demonstrated an enchancment in pedicle screw insertion accuracy with an error fee of only 5. It improves the pace, accuracy, and precision of complex spinal surgery while, generally, eliminating the necessity for cumbersome intraoperative fluoroscopy. Using outlined mathematical algorithms, a particular point within the picture data set may be matched to its corresponding point within the surgical field. This course of is called registration and represents the critical step of image-guided navigation. At least three factors have to be matched, or registered, to permit for correct navigation. The widespread elements of most of these methods embrace an image-processing laptop workstation interfaced with a two-camera optical localizer. When positioned throughout surgical procedure, the optical localizer emits infrared light toward the operative subject. A handheld navigational probe mounted with a exhausting and fast array of passive reflective spheres serves because the hyperlink between the surgeon and the computer workstation. Alternatively, passive reflectors may be hooked up to standard surgical devices. The spacing and positioning of the passive reflectors on every navigational probe or custom-made trackable surgical instrument is thought by the pc workstation. This information is then relayed to the computer work-station, which might then calculate the exact location of the instrument tip within the surgical field in addition to the placement of the anatomic point on which the instrument tip is resting. The initial software of navigational principles to spinal surgery was not intuitive. The utility of navigational expertise to spinal surgery includes using the inflexible spinal anatomy as a body of reference. Bone landmarks on the uncovered floor of the spinal column provide the factors of reference necessary for image-guided navigation. Specifically, any anatomic landmark that might be recognized intraoperatively as properly as within the preoperative picture information set can be utilized as a reference point. The tip of a spinous or transverse course of, a aspect joint, or a prominent osteophyte can function a potential reference level. If the patient is moved after registration, this spatial relationship is distorted, making the navigational information inaccurate. This downside can be minimized by the elective use of a spinal monitoring gadget consisting of a separate set of 4 passive reflectors mounted in a recognized configuration on a small frame. This reference body may be hooked up to the exposed spinal anatomy and its place in house tracked by the infrared digital camera system. Movement of the spinal anatomy and the hooked up body alerts the navigational system, which might then make the appropriate correctional calculations to take care of accuracy and remove the want to repeat the registration course of. It is particularly cumbersome when image-guided navigation is used during cervical procedures. Alternatively, image-guided spinal navigation can be performed and not using a monitoring gadget. Patient motion can probably occur with respiration, from the surgical group leaning on the desk, or from a change of desk place. Although movement associated with leaning on the desk or repositioning the desk or the patient will affect registration accuracy, it can be simply avoided during the quick navigational procedure. If inadvertent patient movement does happen, the registration course of may be repeated. Three different registration techniques can be utilized for spinal navigation: paired point registration, surface matching, and automated registration. The registration approach is performed immediately after surgical exposure and earlier than any deliberate decompressive process. The tip of the probe is then positioned on the corresponding level in the surgical field, and the reflective spheres on the probe deal with are aimed towards the digicam. This initial step of the registration process effectively links the purpose chosen in the picture data with the purpose selected in the surgical field. When no much less than three such factors are registered, the probe may be positioned on another level in the surgical field, and the corresponding level in the picture data set might be identified on the computer workstation. Alternatively, a second registration technique known as surface matching can be used. This technique entails choosing a number of, random (nondiscrete) points on the exposed floor of the spine in the surgical area. The time wanted for floor mapping is for a lot longer, with troublesome cases requiring as much as 10 to 15 minutes.
Lamictal 200 mg buy with amex
To establish the extent of interest, lateral radiographs are obtained with a bayonetted spinal needle in the disk area or a Caspar distracting pin in an adjoining vertebral body treatment centers for alcoholism cheap lamictal 25 mg fast delivery. Once the right degree is identified, the longus colli muscle is dissected laterally off the anterior vertebral body with bipolar cauterization and periosteal elevators medications dogs can take purchase lamictal 100 mg. The muscle is mobilized from its medial insertion in a rostrocaudal course to provide about 20 mm of exposure of the anterior facet of the vertebral body, disk, or each. Aggressive dissection of the muscle can disrupt the sympathetic fibers that course along its medial edge or inadvertently injure the vertebral artery. Placing the retractors incorrectly could cause excessive retraction on the esophagus and carotid artery. A second set of retractors can be placed in a rostrocaudal course to realize full publicity of the world of interest. Alternatively, Caspar distracting pins may be placed on the midlevel of the vertebral physique to acquire enough publicity and supply distraction to facilitate identification of the intervertebral area. DiskectomyandCorpectomy Once the anterior side of the spine is exposed, the microscope is introduced into the surgical area for the diskectomy. The diskectomy begins by eradicating the anterior aspect of the annulus fibrosis circumferentially with a sharp knife. A mental picture of the midline is critical to avoid wandering too far laterally. Sometimes, resection and drilling of the Luschka joint have to be prolonged laterally. Central disk-osteophyte complexes can be eliminated safely through the use of thin-plated Kerrison punches and minimizing their protrusion into the spinal canal. Alternatively, osteophytes can be thinned, elevated, and removed with upgoing curets. Distraction is applied and the posterior longitudinal ligament is resected with curets or thin-plated Kerrison rongeurs. The posterior longitudinal ligament has been removed to decompress the spinal canal. Nerve root decompression can be confirmed by palpating the pedicle of the lower cervical vertebrae with a blunt hook. When a corpectomy is carried out, diskectomies are carried out above and beneath the corpectomy sites to acquire a visible gauge of the place the spinal canal lies. The longus colli muscle is dissected laterally until the physique begins to curve laterally and posterolaterally. The vertebrectomy can start by using a narrow Leksell rongeur spanning from one disk to a different. The rest of the corpectomy can be carried out by utilizing a high-speed drill and drilling deep into the posterior cortex. The allograft is full of autologous bone particles obtained through the corpectomy to promote fusion. Large emissary and epidural veins are rigorously controlled with bipolar coagulation. At levels of extreme compression, osteophytic ridges that could be adherent to the underlying dura are dissected fastidiously. Once the central decompression is accomplished, thin-plated Kerrison punches are used to widen the canal from pedicle to pedicle. At the level of the vertebral physique, intensive lateral dissection is unnecessary as a result of myelopathy is a central phenomenon and radiculopathy, a extra lateral phenomenon, is addressed during the diskectomy portion of the decompression. Fusion Once the diskectomy or corpectomy is carried out, the tip plates are prepared to reinforce bony fusion. After diskectomy, three kinds of fusion strategies, which have been modified during the last a long time, can be used. The Cloward technique makes use of a cylindric bone dowel from the iliac crest or a specifically ready iliac allograft. The bone graft largely sits on soft cancellous bone, which predisposes it to a slight degree of collapse in comparison to the other methods. Despite this minor drawback, the Cloward method effectively deals with cervical disk disease. Another technique, popularized by Simmons and Bhalla,70 uses a keystone-shaped graft. The graft is seated in a triangularly shaped notch situated at every finish plate and oriented posteriorly. With the use of intraoperative traction, the graft is fitted and locked into place to forestall it from migrating posteriorly or anteriorly. The mostly used process is the Smith and Robinson method with numerous modifications. This approach uses a horseshoe-shaped graft seated on stronger subchondral bone, which resists settling to some extent. Initially, the top plates have been ready by perforating them with curets to enhance fusion throughout the graft. New modifications use a drill to create bleeding surfaces without complete resection of the end plates. A 1- to 2-mm posterior shelf of bone is created within the superior aspect of the inferior vertebral body to forestall migration of the graft into the spinal canal. For corpectomy sites, the tip plates are ready similarly as for diskectomy. More recently, multiple research have highlighted the morbidity related to harvesting autografts. Allograft is associated with fusion rates similar to those of autograft and is less expensive than many artificial options. Careful preparation of the top plate ensures profitable incorporation of the graft and prevents it from being dislodged. In each diskectomy and corpectomy, the grafts are positioned while the top plates are distracted. Lateral radiographs are obtained to assess for proof of overdistraction, which could cause postoperative ache, and to confirm good boneto-graft surface contact. The intention of this chapter is not to promote or focus on any explicit plating system intimately. Rather, the basic rules of anterior instrumentation and plating will be mentioned. Some of the benefits of cervical plating embrace elevated segmental stiffness, prevention of graft-related complications, and restoration of cervical lordosis. Improvement in fusion success charges with anterior cervical plating for a one-level fusion has been questioned. Such elimination can be performed with a high-speed drill or with Leksell or pituitary rongeurs. Careful attention is required to avoid removing the anterior cortex of the vertebral physique as a outcome of it offers a significant quantity of resistance to screw pullout. When a corpectomy autograft is used, the graft itself can be secured to the plate with a bicortical screw. The screw ought to be placed in dense bone tissue within the subchondral region of the bone without violating the tip plate.
25 mg lamictal generic with amex
The lateral limb of the "hockey stick" incision is opened by transecting the transversely oriented thoracic muscles treatment quadricep strain 100 mg lamictal purchase amex. The myocutaneous flap is elevated to expose the longitudinally oriented erector spinae musculature medications metabolized by cyp2d6 50 mg lamictal order with mastercard. An prolonged midline incision can provide comparable access with less musculoligamentous harm and probably an improved cosmetic result. Once the transversely oriented muscle tissue are retracted, the lateral margin of the erector spinae is recognized and dissected medially to show the underlying ribs. Surgery is usually reserved for kyphosis larger than 30 levels, in addition to radiographic evidence of development of the deformity. Clinical indications for operative intervention embody intractable axial or radicular pain and progressive neurological deficits. At the thoracolumbar junction, instrumentation is critical to withstand the dynamic biomechanical forces encountered at this stage. Most of these rare lesions can be resected efficiently through a posterolateral method without the addition of fusion and fixation. Mobilization of the erector spinae muscle permits access to the lateral spinal compartment. The longitudinal muscle mass is wrapped in a moist sponge to avoid desiccation and positioned medially or laterally to permit the surgeon to work on both aspect. Complete dissection of the vertebral elements above and under the pathologic degree ensures adequate ventral publicity. The dorsal and lateral rib surfaces are uncovered with a Cobb elevator up to the articulation of the vertebral physique. The ventral gentle tissue is dissected free in subperiosteal trend with a Doyen rib dissector. The uncovered transverse course of on the level of the pathology, together with 6 to eight cm of the corresponding rib, is then resected with a rib cutter and rongeur. The costotransverse and costovertebral joints are disarticulated and transected sharply. Resection of the rib head exposes the anterolateral floor of the backbone, together with the pedicle and intervertebral foramen. Resection of 3 to four cm of the adjoining ribs can enhance ventral exposure; however, excessive rib resection can lead to a flail chest deformity. Once the rib and transverse processes are eliminated, the neurovascular bundle is identified throughout the endothoracic fascia, deep to the intercostal musculature. The segmental nerves above and at the level of the pathology are dissected free and divided, with the proximal stump elevated medially towards the intervertebral foramen. Unlike the situation on the lumbar ranges, nerves on the thoracic levels could be sacrificed with out incurring a functional deficit. Once the nerve is free, the parietal pleura is displaced ventrally to offer entry to the anterolateral spinal compartment. The parietal pleura is saved out of the operative subject with a table-mounted retractor system. The parietal pleura, diaphragm, or both are bluntly dissected free from the ventrolateral facet of the vertebral our bodies with a Cobb elevator. Sharp dissection may be required at the level of the disk space if extra adherent connective tissue is present. The sympathetic chain is recognized along the ventrolateral side of the vertebral bodies. The rami communicantes are transected on the involved spinal segments, and the sympathetic chain is mobilized by subperiosteal dissection. The beforehand elevated nerve stump facilitates dissection to the foramen and pedicle. A distinct benefit of the lateral extracavitary approach is the simultaneous access supplied to each the anterolateral and the posterior spinal compartments. The spinal canal can be decompressed by resection of both the posterior and anterior elements. A important leak mandates placement of a chest tube during the instant postoperative period. Multilayer wound closure is carried out while ensuring to reattach the appropriate muscle layers. RetropleuralThoracotomy Retropleural thoracotomy is appropriate for pathology extending up to two spinal segments. Unlike the lateral extracavitary strategy, the retropleural and transpleural approaches provide a greater diploma of ventral publicity at the expense of posterior entry. The patient is positioned in a lateral place with an axillary roll and acceptable padding to forestall stress neuropathies. Because of the caudal rib angulation, the incision for an anterolateral strategy should be made two ranges above the pathology. For instance, a lesion at T8 could be approached via an incision over the sixth rib. The incision for a retropleural method begins approximately 4 cm from the midline over the rib of interest and extends to the midaxillary line. C, the endothoracic fascia is incised consistent with the skin incision to achieve entry to the retropleural house. The surrounding soft tissue is detached from the dorsal aspect of the rib with an Addison dissector while preserving the intercostal neurovascular bundle. A Doyen dissector is used to free the ventral periosteum along the length of the rib. The dissection continues as far medially as possible, normally 1 to 2 cm lateral to the costotransverse joint. The endothoracic fascia is identified as the shiny tissue layer deep to the rib periosteum but superficial to the parietal pleura. The underlying parietal pleura is freed in all directions by blunt dissection with a finger or sponge dissector. This maneuver exposes the costotransverse joint and anterolateral side of the vertebral our bodies. For exposure of the decrease thoracic region and thoracolumbar junction, the lateral attachments of the diaphragm have to be divided so that the retropleural and retroperitoneal spaces are in communication. Instead of incising the diaphragm circumferentially from the anterior chest wall, the eleventh and twelfth rib attachments to the diaphragm are dissected subperiosteally via a smaller, more caudal diaphragmatic opening. The dissection continues medially to raise the lateral and medial arcuate ligaments from the underlying muscles. At the transverse process of L1, a cuff of muscle is left intact to assist reapproximate the diaphragm. Finally, the left crus is split to complete the communication of the retropleural and retroperitoneal cavities. The peritoneum is gently swept from the posterior abdominal wall, with special attention paid to the realm close to the central tendon, the place the peritoneum is thinner.
Guatemala Lemongrass (Lemongrass). Lamictal.
- Stomach and intestinal spasms, stomach ache, high blood pressure, convulsions, pain, vomiting, cough, rheumatism, fever, common cold, exhaustion, headache, use as an antiseptic and astringent, and other uses.
- Dosing considerations for Lemongrass.
- What is Lemongrass?
- How does Lemongrass work?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96704
Lamictal 100 mg order
The patient underwent L3 to S1 laminectomy, bilateral foraminotomy, durotomy, intradural lysis of adhesions, detethering of the spinal cord, and thoracolumbosacral reconstruction with instrumented fusion from T10 to the sacrum treatment kidney failure buy lamictal 200 mg otc. There were no perioperative neurological deficits, and the patient reported enchancment within the extent of her decrease limb neuropathic ache medicine 369 lamictal 50 mg generic with visa. AnewpostoperativeL3motordeficit, however, was observed (mild weak spot of the left quadriceps muscle). Insert, Flow voids demonstrating multiple dilated vessels in the neighborhood of the mass. Although current intraoperative monitoring strategies rely on electrode-based stimulation and recordings, it may be attainable to directly visualize the myelinated axonal constructions in vivo with improved microscopy strategies, especially with the recent advances in optics and laser expertise. Through a vibrationally resonant thirdorder nonlinear process (coherent anti�Stokes Raman scattering), a photon at a better frequency is emitted to provide lipid-based distinction. By advantage of being a nonlinear process, it advantages from three-dimensional sectioning and excessive spatial resolution similar to two-photon fluorescence excitation. In the lengthy run, a hybrid system consisting of electrode-based stimulation and microscopy imaging� based mostly recordings could possibly present spatially localized practical info of the spinal cord and nerve roots to the surgical staff. Despite the lack of degree I evidence to assist intraoperative monitoring, we advocate multimodality neurophysiologic recordings as an adjunct to assist the surgical staff throughout backbone and spinal twine surgery. The quantity and forms of monitoring modalities used rely upon the individual affected person and the experience and decision making of the electrophysiologist and the anesthesia and surgical teams. Multimodality intraoperative monitoring with an rising number of simultaneously recorded channels is turning into economically and technically possible and thus might present the optimum monitoring environment for complex backbone surgery, particularly for sufferers with preexisting spinal twine deficits. As with any approach that entails a quantity of disciplines, fixed communication, regular use, and attempts to completely integrate it into every day clinical apply will make intraoperative monitoring a valuable asset to spine surgery facilities. Insert, Cross-sectional picture (2� zoom), which can enable direct evaluation oftheGratioofmyelinatedfibers. �rik B�langer and Daniel C�t�, Universit� Laval, Centre de Recherche Universit� Laval Robert-Giffard,Centre for Optics, Photonics, and Lasers, Canada. Real-time steady intraoperative electromyographic and somatosensory evoked potential recordings in spinal surgery: Correlation of clinical and electrophysiologic findings in a potential, consecutive sequence of 213 circumstances. Comparison of transcranial electrical motor and somatosensory evoked potential monitoring throughout cervical spine surgical procedure. Intraoperative electrophysiologic monitoring: Considerations for complex spinal surgical procedure. Multimodality intraoperative neurophysiologic monitoring findings throughout surgical procedure for grownup tethered cord syndrome: Analysis of a collection of forty four patients with long-term follow-up. Multimodality neurophysiological monitoring during surgery for grownup tethered wire syndrome. Combined monitoring of motor and somatosensory evoked potentials in orthopaedic spinal surgical procedure. Neuro-physiological monitoring for safe surgical tethered twine syndrome release in adults. Mechanisms of sign change during intraoperative somatosensory evoked potential monitoring of the spinal twine. John Hurlbert the intervertebral disk undergoes structural modifications from birth via old age. The change in tissues to a lower or less functionally lively kind is defined as degeneration. Disk degeneration, due to this fact, refers back to the deterioration in disk high quality seen all through adult life. A extra expanded definition supplied by Batti� and Videman states that Conceptually, disc degeneration is a product of lifelong degradation with synchronized reworking of discs and neighboring vertebrae, together with simultaneous adaptation of the disc structures to changes in bodily loading and responses to the occasional damage. The price and extent of these modifications range between levels within the individual particular person and between individuals. There is little consensus about what constitutes pathologic or symptomatic degeneration. It has been proposed that Early degenerative changes should check with accelerated age-related modifications. Degenerative disc illness ought to be applied to a degenerate disc that can be painful. It should be emphasized that disk degeneration and disk herniation are intently associated but not synonymous. The annual spine-related health care expenditure in the United States for 2005 was estimated to be $86 billion, in the identical realm as cancer care ($89 billion) and accounting for 9% of all health care spending. The central, gelatinous nucleus pulposus is contained by the multilaminated annulus fibrosus. The superior and inferior elements of the disk are coated by cartilaginous vertebral finish plates. Significant changes in the anatomic construction and biochemical composition of these elements happen in growth and proceed throughout life. The nucleus has a very excessive water content material due to the hydrophilic nature of the proteoglycans. The annulus fibrosus consists of concentric lamellae of collagen fibers and a small quantity of elastic fibers certain together by a lesser quantity of proteoglycan gel. Within a lamella, the obliquely oriented collagen fibers are parallel to each other, but adjoining lamellae alternate the orientation of their fibers. The fibroblast-like cells of the annulus fibrosus are spindle-shaped and lengthen alongside the collagen fibrils, whereas the cells of the nucleus pulposus seem rounded and have been likened to chondrocytes. The fibers of the inner lamellae are steady with these of the vertebral end plate and kind an envelope around the nucleus pulposus. The vertebral end plates are largely fibrocartilage, with lesser amounts of hyaline cartilage found nearer the vertebral our bodies. The sources of those fibers within the anterior and lateral aspect of the annulus are direct branches from the ventral rami of the spinal nerve roots and the gray rami communicantes of the sympathetic trunk. The posterior annulus receives fibers from the sinuvertebral nerve, which varieties from the union of an autonomic root from the grey rami communicantes and a somatic root from the ventral rami. Hence, the metabolic needs of the disk are met passively by diffusion through the adjacent bony and cartilaginous finish plates, as nicely as by way of its personal matrix. This leads to a marked concentration gradient within the disk, with lowest oxygen tension, glucose concentration, and pH within the center. Disk chondrocytes are nicely tailored to this setting, with maximal proteoglycan manufacturing occurring at 5% oxygen and a pH of seven. Keratin sulfate and chondroitin sulfate present the excessive anionic cost densities needed for the osmotic properties of aggrecan. Through interaction with hyaluronan and link protein, aggrecan types large aggregates and functions to retain water within the nucleus. They may have a task within the mechanical behavior of the disk through their interaction with fibrillar collagen. The macroscopic look of lumbar disk degeneration has been classified into stages defined by the three parts of the disk (nucleus, annulus, and finish plates) from the angle of a midsagittal section by Thompson and coworkers.
Discount lamictal 25 mg mastercard
Reactive modifications within and across the wire could result in irreversible neurological compromise medicine for diarrhea lamictal 25 mg buy free shipping. Fungal sources of an infection, as well as mycobacterial sources, could also be much less common than bacterial pathogens but certainly have significant destructive potential 6mp medications lamictal 200 mg purchase on line. Although uncommon in many industrialized nations, fungal and Mycobacterium tuberculosis infections could usually be misdiagnosed and may result in significant neurological damage because of both bone destruction and neural compression. A variety of each medical and surgical choices are available for treating spinal fungal and tubercular infections. In this chapter we focus on all kinds of pathogens with significant emphasis on M. The spine is the most common bone web site, adopted by the cranium, ribs, tibia, and bones of the wrist and foot. Infection can unfold both through the intervertebral disk and alongside the anterior longitudinal ligament and affect other vertebral our bodies; it could possibly additionally result in psoas or different paravertebral abscesses. Osseous involvement develops in 10% to 20% of these with disseminated illness, and spine involvement occurs in 10% to 60% of those individuals. Because of their excessive blood flow, the vertebral bodies are particularly in danger for an infection from disseminated M. Infection can then unfold behind the anterior longitudinal ligament to infect the adjacent vertebral physique. The infection also can spread to adjacent native constructions and lead to a probably compressive epidural abscess. Extraspinal abscesses can erode native constructions such as ribs or can increase inside the psoas muscle and monitor down so far as the groin. First, the "stage of onset" consisted of localized infection and a warm tender space of swelling with significant osteoporosis however minimal bone destruction. The second stage, generally identified as the "stage of destruction," consisted of development of disease with bone destruction, deformity, subluxation, contracture, and abscess formation. The abscesses usually developed draining sinuses that have been vulnerable to superimposed pyogenic infection, which significantly taxed the host immune system. Those who survived this stage entered the part often known as the "stage of restore and ankylosis," in which the general situation incessantly improved. Unfortunately, frequent reactivation of the disease caused progression of signs and deformity. Surgeons then began to pursue operations at sites distant from the placement of an infection to avoid opening the positioning of illness. Albee as early as 1911 and Hibbs as early as 1912 developed the technique of posterior spinal fusion within the hope of shortening the interval of immobilization and bed relaxation by offering some degree of inside stability. Improved outcomes have been as a end result of the fact that antitubercular medicine prevented the dissemination of the disease at the time of surgical procedure that was frequent before the utilization of antitubercular brokers. As using antitubercular brokers was turning into extra commonplace, decision of the draining sinuses and abscesses without surgical intervention may happen. Surgeons then started to reserve surgical intervention for prevention and correction of deformity, for sufferers with neurological deterioration or progressive disease, and in an attempt to enhance performance and the quality of lifetime of severely affected sufferers. Treatment is required to each control the first source and tackle the sequelae of harmful backbone infections. For instance, a history of previous fungemia, immunosuppression, diabetes, central venous catheterization, intravenous drug abuse, parenteral diet, or implanted prosthetic units all place patients at larger danger for fungal infection of the backbone in the setting of again ache. This ache could additionally be associated with muscle spasm and has a mechanical nature in that it may be triggered by even the slightest of actions. This collection of signs has been described as inflicting the affected person to have an "aldermanic gait," or a rigid posture that induces the affected person to walk with brief deliberate steps to keep away from any jarring of the backbone. Mechanical instability or the formation of kyphosis as a end result of vertebral destruction, pathologic fracture, or subluxation can also contribute to neurological issues. The spinal wire itself might start to display some signs of irritation such as twine edema, or the disease burden might affect the meninges, which may set off reactionary inflammatory modifications in the twine that result in neurological compromise. In addition, vascular issues such as infective thrombosis or endarteritis of spinal vessels may result in twine infraction and thus neurological problems. After inhalation, Aspergillus can affect the spine by direct extension from lung tissue or by hematogenous unfold. Another essential supply of an infection for a few of these pathogens is direct contamination at the time of surgical procedure. Candida an infection can occur in patients with intravenous lines or monitoring gadgets and through implantation of prosthetic gadgets. Stretching of the wire over an anterior inner gibbus can result in spinal wire gliosis and ultimately neurological issues. Unfortunately, neurological sequelae can happen at much lesser levels of canal compromise within the setting of vascular complication or mechanical instability. The radiographic appearance of fungal infections of the spine is much like that of the pyogenic causes of spinal osteomyelitis. For instance, Williams and coauthors reported a case series of three immunocompromised sufferers with fungal infections of the spine. This lack of signal was considered the results of a depressed immune response in these immunocompromised individuals. Pyogenic infections sometimes present T2 hyperintensity within the intervertebral disk, whereas the absence of T2 hyperintensity within the intervertebral disk with preservation of the internuclear cleft is extra typical of pathogens similar to M. It can be believed that the lack of hyperintensity is a results of the absence of proteolytic enzymes in Mycobacterium. It is important to point out that although the lack of hyperintensity with fungal infections could additionally be the results of a blunted immune response, it could additionally symbolize the paramagnetic and ferromagnetic properties of the fungus itself, as seen in fungal sinusitis. However, they have a tendency to involve adjoining ribs and posterior elements and develop draining sinuses less regularly. Finding the correct prognosis could be aided by different testing methods, such as the carbohydrate assimilation check for Candida and the phenol oxidase reaction for Cryptococcus. Frequently, the draining exudate is colonized with bacteria or fungi, which when cultured could lead to an incorrect diagnosis. Nonsurgical administration is the mainstay of first-line treatment of some fungal infections of the backbone, but several pathogens are best handled by surgical intervention for evacuation of abscesses, which yields greater clearance charges. Surgery can be required for patients with spinal instability, neurological deficit, or sepsis. Amphotericin B is usually the first-line agent for many disseminated fungal infections. Many of those who undergo from disseminated fugal an infection will require long-term antifungal remedy. The morbidity of amphotericin B remedy includes the truth that it should be given intravenously, as well as its potential for nephrotoxicity. In some international locations, directly noticed treatment with fixed-dose multidrug combos has resulted in improved results. Moreover, the diagnosis is regularly troublesome to made with out open surgical d�bridement and culture of the offending pathogen. The goals of surgical intervention embody aggressive d�bridement, relief of neural compression, and return of spinal stability. Advancements in imaging modalities have improved the power to diagnose earlier phases of infections of assorted causes and have made nonoperative management more effective.
Lamictal 25 mg generic on line
These tumors even have important metastatic potential, with the liver, lung, bone, and delicate tissue being most popular sites for metastatic dissemination treatment yeast uti 200 mg lamictal cheap visa. However, at least two malignancies of the meninges, hemangiopericytoma and atypical or malignant meningioma, including meningiosarcoma, do exhibit options characteristic of malignant neoplasms medicine 20th century lamictal 50 mg for sale. In the World Health Organization classification, four histopathologic variables are assessed for meningiomas: grade, histologic subtype, proliferation index, and mind invasion. Malignant meningioma frequently has histologic proof of brain parenchyma invasion and, not often, evidence of distant metastases. Histopathologically, these neoplasms have vital vascular proliferation, increased cellularity, excessive charges of mitosis, and frequent occurrence of necrosis. Under mild microscopy, meningiosarcomas can be categorized as either fibrosarcomas, spindle cell sarcomas, or mixed sarcomas. Because of the rarity of those tumors, identification of the most effective therapeutic approaches has been difficult. Although the dose prescribed adjuvantly can vary,156 a dose within the 60-Gy vary in 30 to 33 fractions is really helpful primarily based on retrospective information. Accounting for lower than 1% of all mind tumors, these neoplasms are characterized by a excessive native response fee and metastatic potential. Nearly 300 instances of hemangiopericytoma have been described within the literature, and so they have arisen from just about every anatomic website. Surgical resection has been the historic and prevalent mode of therapy for these tumors. A total of eighty sufferers with meningeal hemangiopericytoma have been identified, and evaluation revealed a 90% 9-year actuarial risk for native recurrence after surgical resection only. Interestingly, less than 33% of these recurrences had been famous within the first 5 years, which may account for the false assumption that these tumors are extremely curable by surgical resection alone. Radiation responses have been famous to be dose dependent, with larger than 50 Gy providing superior longterm disease-free survival. With current technologies, these reactions are normally rare and clinically readily manageable. Such problems include acute skin reactions, sometimes dry desquamation and some extent of erythema, that are managed with local ointments. This is believed to outcome from retinal stimulation secondary to a phenomenon described as Cerenkov radiation. Nausea is rare until the realm postrema is handled with excessive doses or massive fractions. When large volumes of the mind are handled, particularly in youthful sufferers, lethargy and somnolence may be noticed in roughly 3 months. Rarely, localized demyelination resulting in nausea, vomiting, ataxia, dysphasia, and cerebellar ataxia may develop in some patients. Radiation necrosis can have a highly variable manifestation, from a purely imaging-based prognosis in asymptomatic sufferers to extremely symptomatic people with mass effect and subsequently elevated intracranial pressure, headaches, and symptoms traceable to the anatomic location. Discriminating radiation necrosis from metastases and recurrent glial neoplasms by imaging could be challenging because all can have areas with avid uptake of contrast material on T1-weighted images and can trigger mass impact with native edema. Both positron emission tomography166 and magnetic resonance spectroscopy167 have been advocated to distinguish radiation necrosis from recurrent tumor, although volumetric limitations exist and residual neoplasm interspersed with necrosis can confound the diagnosis. Surgical sampling, via either stereotactic biopsy or surgical excision, is regularly required to finally differentiate necrosis from recurrence. It happens as a consequence of radiation injury to small vessels and will clinically lead to impairment of intellectual function, particularly memory and mathematical ability. The scientific sequelae of these modifications are incessantly manifested as neurocognitive impairment. In addition, host components such as underlying ailments, particularly those characterised by microvascular modifications, including diabetes, hypertension, smoking, stroke, cardiovascular insufficiency, and different situations, also contribute to the larger incidence. More importantly, three-dimensional and conformal techniques cut back the amount of regular brain irradiated. The position of postoperative radiotherapy after resection of single brain metastases. Randomized trial of three chemotherapy regimens and two radiotherapy regimens and two radiotherapy regimens in postoperative remedy of malignant glioma. Benign intracranial tumors, regardless of typically being noninvasive and sluggish growing, incessantly occupy intracranial places that make surgical interventions highly morbid and preclude using highdose (or single-fraction) radiosurgery due to their proximity to critical neural buildings. In current clinical practice, surgery is the therapy of selection for almost all of meningiomas. Resection allows histologic prognosis, relieves mass impact and related symptoms, alleviates tumorinduced seizures, and achieves high local control rates. Safe and full resection is regularly precluded by tumor involvement of the cranial nerves or arteries or invasion of the venous sinuses. Resectability also is dependent upon the site and thus the surgical accessibility of the tumor. Progesterone and estrogen receptors have been recognized in larger than 70% and 30% of meningiomas, respectively. Therapy is due to this fact aimed toward relieving neurological signs and offering long-term tumor control. Meningiomas are neoplasms of the meningothelial cells of the arachnoid layer and occur most frequently at websites where arachnoid cells are most quite a few, specifically, within the arachnoid villi or granulations that lie along the dural venous sinuses. Other areas include the sylvian fissure, parasellar area, and olfactory grooves. Meningiomas can even come up intraventricularly from pia-arachnoid rests, and about 10% happen infratentorially along the free fringe of the tentorium, clivus, foramen magnum, petroclival ligament, and petrous ridge. Strojan and coauthors reviewed the case files of 170,000 meningioma sufferers treated in Slovenia over a 31-year period and reported the actuarial risk of a secondary meningioma developing after cranial irradiation to be zero. More latest sequence, however, demonstrate markedly improved native management rates and progression-free survival charges greater than 93% after 5 to 10 years of follow-up (see Table 251-1). It is worth noting, however, that serious unwanted facet effects of recent strategies of therapy planning and supply are already quite uncommon. The neurological deficits reported in the research included reduced imaginative and prescient, a model new visual area loss, and trigeminal neuropathy. Further analysis of the info by Goldsmith and associates permitted building of a model to foretell that optic nerve tolerance is 890 optic ret, equivalent to fifty four Gy in 30 fractions. Many neurosurgeons argue in favor of shut radiographic and medical follow-up after Simpson grade 1 and 2 resection, but not necessarily Simpson grade three. These rare tumors symbolize less than 2% of all meningiomas and come up from the meningeal lining of the optic nerves. Patients normally have progressive visual loss, though some might exhibit speedy lack of vision. Less widespread complaints embody visible subject defects, lack of or alterations in shade vision, and orbital ache.
Lamictal 100 mg purchase on line
A series of pituitary rongeurs, curets, and scrapers are used to take away the intervertebral disk medicine kit cheap lamictal 200 mg amex. On the aspect ipsilateral to the interbody fusion, pedicle screws can be positioned through the present incision medications keppra buy cheap lamictal 200 mg on line. The disadvantages embrace danger to the belly contents; threat to the lumbosacral plexus within the psoas muscle and the genitofemoral nerve, which lies on prime of the psoas muscle; and the shortcoming to carry out a direct neural decompression. This approach also has the potential to appropriate deformity in cases of flexible spine, though its role as a corrective technique is still being evaluated. The affected person is placed within the lateral position on a regular operating desk with the desk break centered between the iliac crest and the underside of the rib cage. In instances of scoliosis, graft placement is usually facilitated by an method from the convex side as a end result of it supplies better entry to the disk area. The table is broken to maximize the working area between the rib cage and the iliac crest, and the patient is immobilized using a beanbag and fabric tape. A lateral fluoroscopic x-ray is taken, and the table is adjusted to make sure that the target disk house is completely according to the fluoroscopic beam. A 2- to 3-cm transverse incision is made, and after subcutaneous tissue dissection, the criss-crossing fibers of exterior and inner obliques are identified, cut up, and retracted using Army-Navy retractors. After this, the transversalis fascia is seen and sharply divided to expose the fats throughout the retroperitoneal area. A separate, extra dorsal incision can be used to entry the retroperitoneum at a point at which the peritoneal contents are extra distant. Once contained in the retroperitoneum, blunt finger dissection mobilizes the peritoneal contents anteriorly as the surgeon develops a protected corridor to the psoas muscle. The first landmark palpated is usually a transverse course of, then the psoas muscle. A probe stimulator is introduced and advanced into the disk house beneath fluoroscopic steerage. The lumbosacral plexus tends to lie in the posterior third of the psoas muscle, so the surgical corridor is safest in the anterior third of the muscle, which approximates the anterior third of the disk space. The fluoroscope is shifted to the anteroposterior position, and successive dilators are positioned over the K wire. Cand D, the retractor is positioned, the blades are opened, and the retractor is secured over the disk area. K and L, An L1-5 fusion is carried out totally utilizing minimally invasive strategies. A important step is the disruption of the anulus and lateral osteophytes on the contralateral aspect of the disk area. This is successfully and shortly performed using a Cobb retractor guided by fluoroscopy. The graft ought to cover the complete width of the top plate and, ideally, sit in the anterior third of the disk area to maximise lordosis. Multiple disk spaces can often be accessed by way of the same small incision, however each requires a separate muscle dilation. The interbody fusion could be supplemented with vertebral physique screws or percutaneous pedicle screws. Such advances have opened the door for minimally invasive methods to have an effect on deformity. Currently, we place lengthy construct posterior lumbar instrumentation after a midline skin incision and suprafascial dissection. A mixture of minimally invasive posterior and interbody strategies can be used to generate 360-degree fixation over multiple vertebral segments. Although this method is pretty nicely tolerated, postlaminectomy deformities can occur at important rates in high-risk patients, notably if the publicity entails the thoracolumbar junction. This approach has been additional modified through the usage of muscle-splitting tubular retractors, which decrease damage to the paraspinal musculature, and guarded drills, which enable the safe removal of the bottom of the spinous process and inside table of contralateral lamina, growing visualization. The process requires a tubular, expandable retractor and has been applied to intradural tumor resections requiring a twolevel laminectomy (Video 307-1). The quick advantages for sufferers are much less postoperative ache and faster restoration occasions. The attendant preservation of the paraspinal gentle tissues may improve long-term outcomes and enhance the durability of many procedures. Hemilaminotomies are carried out, and the base of the spinous process and ventral portion of the contralateral lamina are drilled away. The contralateral pedicles are palpated with a Penfield 4 to ensure that the contralateral exposure is sufficient. The dura is opened within the midline and tacked to the soft tissues, and the tumor is removed using standard techniques. Specialized, minimally invasive dural closure devices are commercially out there, or a Castro-Viejo needle driver can be utilized. There are different alternative dural closure units and materials which will show to be useful for these circumstances. In our anecdotal experience, this strategy significantly decreases the speed of cerebrospinal fluid leak after intradural surgery as a outcome of the muscle naturally expands into the void created by the retractor, eliminating the useless house by way of which the surgery was carried out. The blades are opened in a rostral-caudal fashion, and additional lateral and medial retractors are added. The soft tissues are dissected off of the ipsilateral laminae and the base of the spinous processes. The base of the spinous process is drilled away together with the ventral cortex of the contralateral lamina. After hemostasis, the dura is opened within the midline, and the tumor is eliminated using normal techniques. The dura is closed primarily, in this case with clips, though we usually use a working 4-0 suture. Minimally invasive operative management for lumbar spinal stenosis: overview of early and long-term outcomes. Perioperative results following lumbar discectomy: comparability of minimally invasive discectomy and normal microdiscectomy. Open versus minimally invasive lumbar microdiscectomy: comparability of operative times, size of hospital keep, narcotic use and issues. Clinical outcomes after minimal-access surgery for recurrent lumbar disc herniation. Minimally invasive far lateral microendoscopic discectomy for extraforaminal disc herniation at the lumbosacral junction: cadaveric dissection and technical case report. Menezes the craniovertebral junction is a biomechanical and anatomic unit that contains the clivus, foramen magnum, and higher two cervical vertebrae. These patients have a fluctuating neurological course, and an erroneous prognosis is widespread owing to the anatomic complexities of the decussation of the sensory and motor tracts.