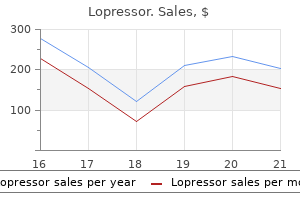
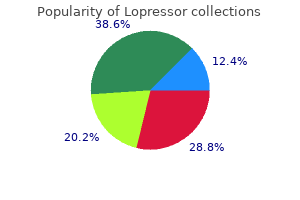
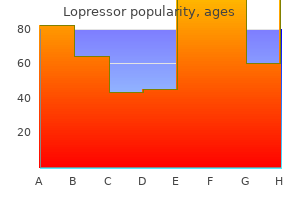
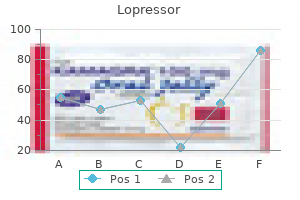
Lopressor
Lopressor dosages: 100 mg, 50 mg, 25 mg, 12.5 mg
Lopressor packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 30 pills

Purchase lopressor 100 mg without a prescription
Sundstrom J arterial dissection cheap lopressor 12.5 mg, Arima H blood pressure chart usa generic lopressor 12.5 mg without a prescription, Jackson R, et al: Effects of blood pressure discount in delicate hypertension: a systematic review and metaanalysis. Research Group: Prevention of stroke by antihypertensive drug therapy in older persons with isolated systolic hypertension. Benetos A, Safar M, Rudnichi A, et al: Pulse pressure: a predictor of long-term cardiovascular mortality in a French male inhabitants. Garg R, Yusuf S: Overview of randomized trials of angiotensinconverting enzyme inhibitors on mortality and morbidity in sufferers with heart failure. Persson F, Rossing P, Reinhard H, et al: Renal results of aliskiren in contrast with and in combination with irbesartan in patients with sort 2 diabetes, hypertension, and albuminuria. Bellet M, Sassano P, Guyenne T, et al: Converting-enzyme inhibition buffers the counter-regulatory response to acute administration of nicardipine. Os I, Bratland B, Dahl�f B, et al: Female preponderance for lisinopril-induced cough in hypertension. Results from the Third National Health and Nutrition Examination Survey, 1988-1991. Mulatero P, Stowasser M, Loh K-C, et al: Increased analysis of main aldosteronism, including surgically correctable types, in facilities from five continents. Redolfi S, Yumino D, Ruttanaumpawan P, et al: Relationship between in a single day rostral fluid shift and obstructive sleep apnea in nonobese males. Brinker S, Pandey A, Ayers C, et al: Therapeutic drug monitoring facilitates blood stress control in resistant hypertension. Schulz V: Clinical pharmacokinetics of nitroprusside, cyanide, thiosulphate and thiocyanate. The major transport targets for diuretic medicine have been outlined and their genes cloned. The effects of illness on diuretic kinetics are mentioned as a result of they predict the required dosage modifications. Loop diuretics and thiazides are the most broadly used diuretics, and the physiologic diversifications to their prolonged use are described. Diuretic resistance, its administration, and the main adverse effects of remedy are discussed. This discussion offers a framework for the design of methods to maximize the desired actions whereas minimizing the unwanted effects. An additional, extra modest, impact alongside the distal nephron, nevertheless, can additionally be noticed. The biochemical, morphologic, and practical properties of carbonic anhydrase have been reviewed. Distal convoluted tubule diuretics (thiazides) Distal potassium sparing diuretics 5. Distal potassium sparing diuretics Mineralocorticosteroid antagonists Carbonic anhydrase inhibitors 6. This agent has less renal effect and due to this fact is preferred for therapy of glaucoma. Chlorideresponsive metabolic alkalosis is best treated by administration of Cl- with K+ or Na+. Metabolic alkalosis as a result of loop diuretics or thiazides can depress respiration in patients with continual respiratory acidosis, for instance, because of continual obstructive pulmonary disease. Acetazolamide is useful in a dose of 250 mg daily as prophylaxis against mountain illness, most likely by way of stimulating respiration and diminishing cerebral blood move and cerebrospinal fluid formation. In the water-permeable nephron segments of the proximal nephron and the skinny limbs of the loop of Henle, fluid reabsorption concentrates filtered mannitol sufficiently to diminish tubular fluid reabsorption. Ongoing Na+ reabsorption lowers the tubular fluid [Na+] and creates a gradient for again flux of reabsorbed Na+ into the tubule. Mannitol increases the medullary blood circulate and reduces the medullary solute gradient, thereby stopping urinary concentration. A trial of mannitol remedy for cerebral edema complicating hepatic failure demonstrated a markedly higher survival of 47%, compared with only 6% within the control group. Normally these electrolyte changes are quickly corrected by the kidney, supplied that renal perform is enough. In fact, when mannitol-induced hypernatremia exceeds serum sodium ranges of one hundred fifty mmol/L, its optimistic effects are outweighed by untoward results, together with renal failure, and better mortality. Circulatory overload, pulmonary edema, central nervous system melancholy, and extreme hyponatremia require urgent hemodialysis. Notethatthetransepithelial voltage along the thick ascending limb is oriented with the lumen positiverelativetoblood(circledvalue,giveninmillivolts[mV]). Increased delivery to the unsaturated distal tubule reabsorption process will increase Na+ reabsorption. Its inhibition by loop diuretics impairs both free water excretion throughout water loading and free water reabsorption during dehydration. Only the unmetabolized and secreted fraction is on the market to inhibit NaCl reabsorption. These variations could also be clinically related,106,107 but giant managed trials finding out this issue are lacking. Therefore, a low serum albumin focus enhances furosemide metabolism113 but decreases tubular secretion of lively diuretic. The relationship between fractional sodium excretion and the log of the serum diuretic focus is sigmoidal. Subsequent to their development, non-thiazide drugs with comparable activities have been developed. First, Beaumont and colleagues showed that [3H]metolazone binds avidly to kidney membrane proteins; its binding is inhibited competitively by Cl-, suggesting that Cl- and diuretic compete for a similar binding website. They conclude that thiazide diuretic affinity is conferred by transmembrane segments 8 through 12, whereas transmembrane segments 1 via 7 affect chloride affinity. It was discovered to not have any impact on urinary Na+ or K+ immediately, but as a substitute to competitively block the mineralocorticoid receptor. These medicine have been employed for a couple of years primarily to scale back the excretion of K+ and web acid, particularly when utilized in mixture with other diuretics. Under sure circumstances, however, their natriuretic efficacy can be significant. For instance, spironolactone is more effective than furosemide in reducing cirrhotic ascites. Spironolactone is metabolized to canrenones (t1/2 = sixteen hr) and to sulfur-containing metabolites, predominantly 7 alpha-thiomethylspirolactone (t1/2 = thirteen hr). Eplerenone is indicated to stop cardiac reworking and systolic dysfunction within the setting of latest myocardial infarction. Impaired net acid excretion can cause metabolic acidosis,199 which worsens hyperkalemia. Amiloride and triamterene accumulate in renal failure,170,200 and triamterene accumulates in cirrhosis.
12.5 mg lopressor free shipping
Preparation of the dialysate and its composition is important to the success of dialysis blood pressure chart new lopressor 25 mg order amex. The answer must be ready from properly handled water (see later) that features lowering the focus of endotoxin to prevent pyrogenic reactions within the patient blood pressure quiz pdf generic lopressor 100 mg overnight delivery. The concentrations of important solutes added to the dialysate replicate those normally maintained within the body by the native kidneys (Table 65. The dialysate is essentially a physiologic salt answer that creates a gradient for removing of undesirable solutes and maintains a continuing physiologic concentration of extracellular electrolytes (see later). A full review of this topic is past the scope of this chapter, and readers are referred to evaluations on the topic. A second filtration process removes particulate matter in addition to microbiologic organisms. Alternatively, chloramine might happen naturally or could additionally be added on to municipal water as a bactericidal agent. Unfortunately, in distinction to the beneficial results of chlorine, direct publicity of the blood to chloramine causes acute hemolysis and methemoglobinemia. Water temperatures under 77� F cut back the circulate fee and thus the efficiency of the reverse osmosis system, and temperatures above 100� F might injury the membrane. Using cationexchange resins that comprise sodium, the water softener then removes calcium, magnesium, and other polyvalent cations from the feed water, stopping these cations from depositing on and damaging the reverse osmosis membrane. Next, granular activated carbon in the carbon filtration tank absorbs chlorine, chloramines, and different natural substances from the water. Activated carbon could be very porous and has a high affinity for natural materials, but when not serviced correctly or exchanged frequently, it can be contaminated with micro organism. Downstream, the water is then filtered through a 5-�m cartridge filter to forestall carbon particles from fouling up the reverse osmosis pump and membrane. Finally, the water is delivered to the reverse osmosis unit, which applies high hydrostatic pressure to pressure water via a extremely selective semipermeable membrane that rejects 90% to 99% of monovalent ions, 95% to 99% of divalent ions, and microbiologic contaminants bigger than 200 Da. The water exiting the reverse osmosis unit is termed the permeate or product water and, in most clinics, can be utilized safely for dialysis. The cationic resin exchanges hydrogen ions for different cations in descending order of affinity: calcium, magnesium, potassium, sodium, after which hydrogen. The anionic resin exchanges hydroxyl ions for other anions in descending order of affinity: nitrites, sulfates, nitrates, chloride, bicarbonate, hydroxyl, and fluoride. When the resin is exhausted, beforehand adsorbed ions, particularly these of lower affinity, can elute into the effluent, resulting in levels which may be more than 20 times their ordinary concentration in tap water and cause severe toxicity and even demise. Therefore, stricter standards for water high quality as nicely as high-level disinfection to kill all microorganisms (except bacterial spores) are essential. For ultrapure dialysate, much more stringent criteria are in place, including a bacterial count lower than zero. Instead, bacterial pyrogens similar to lipopolysaccharide, peptidoglycans, exotoxin, and their fragments are thought to be the culprits. Although the bigger pore dimension in hi-flux dialyzers might improve backfiltration and allow endotoxins to enter the blood compartment from the dialysate, artificial membranes also adsorb endotoxin, thereby attenuating the effect of moderately contaminated dialysate. The supply water and the product water must be assayed routinely to ensure that product water meets requirements for heavy metal and different ionic contaminants. The frequency of scheduled testing is determined by the standard of the water supply, the sort of water remedy system used, and the seasonal variation in chemicals added to municipal water to ensure its potability. If the patient was awake and performing at any level, the dialysis was deemed profitable. In light of discussions in regards to the scope of dialysis adequacy, it is very important distinguish the adequacy of the remedy itself. The clinician must treat the whole patient, including giving such remedies as psychotherapy for melancholy, management of anemia, nutrition, blood ldl cholesterol, and utility of recent strategies for prophylaxis and treatment of cardiovascular threat components. The focus of the following discussion is on solute and water removal; standards established for other features of kidney replacement are discussed within the part "Management of Patients on Maintenance Hemodialysis. For native kidney operate, the latter is achieved by collecting timed urine specimens. The relationship between the syndrome and kidney disease was not obvious in antiquity, and even after the relationship was recognized, lack of non-excretory capabilities of the kidney might be equally implicated as the trigger, particularly as a end result of urine volume and content material, which mirror oral intake, differ little from normal as the disease progresses. This growth confirmed suspicions of an accumulation disease, but it was not until dialysis reversed the syndrome that this hypothesis could be thought-about proven. In addition to the change in urea volume and urea technology, this model can be prolonged to embody the interdialysis interval and the effects of residual kidney function (Kr). The latter, in contrast to the dialyzer clearance, is a steady clearance that has little effect during dialysis however supplies a marked profit between treatments when the dialyzer clearance is zero. Efforts must be made to pattern after access-related rebound is full but before cardiopulmonary rebound begins. Accumulation of urea in the patient results from each amino acid catabolism, a measure of protein nutrition, and failure of renal excretion. Although these dual effects on urea concentrations complicate interpretation of any single measured degree, mathematical modeling of urea mass steadiness permits each separation of the two and an estimate of urea distribution quantity. Toxic solute focus levels are the web effect of solute technology and elimination. If one attributes uremic toxicity to the concentrations of amassed solutes (concentration-dependent toxicity), then it might seem logical that the clearance (Kt/V) ought to sufficiently stability the technology price to maintain a secure low concentration. Control of solute concentrations by dialysis clearly improves outcomes, however control by limiting of dietary intake is commonly unwell advised. Consuming a vegetarian or high-fiber food regimen might alter intestinal flora and cut back the generation of gut-derived toxins. Because the prescribed K ought to be the same as the delivered K, and prescribed K can be determined from Equation 5, modeled V is easily decided. Because body dimension expressed as V is the size-normalizing issue for urea clearance in the Kt/V expression, larger sufferers require higher clearances and are therefore at greater threat for underdialysis. Although mortality was not affected by administering a better dialysis dose for the 1846 randomized sufferers as a complete, when ladies were analyzed separately, a borderline important enchancment in mortality and secondary outcomes was seen on the larger dose. However, gender was troublesome to separate from dimension as a end result of the two are so carefully linked, especially with regard to V. Paradoxically, shortening the therapy accentuates these symptoms because the rate of elimination should increase if the affected person is to remain in solute and water balance. Many hours have been spent by nephrologists and dialysis nurses in attempts, often unsuccessful, to persuade sufferers that extending Td would be beneficial. Sometimes a brief trial of both an prolonged Td or increased frequency is enough to persuade the affected person. Other efforts to report the reciprocal of Kt/V as a concentration equal,344 focusing on low concentrations instead of excessive clearances, has not been applied, partly as a end result of Kt/V has turn into ingrained in the follow of dialysis quantification.
Discount lopressor 50 mg otc
Vital signs are obtained frequently in the first hour after which each 2 to four hours blood pressure cuff amazon 12.5 mg lopressor order with visa. Asif A blood pressure medication making me cough buy lopressor 12.5 mg with visa, Cherla G, Merrill D, et al: Venous mapping using venography and the risk of radio-contrast-induced nephropathy. Lee T, Ullah A, Allon M, et al: Decreased cumulative access survival in arteriovenous fistulas requiring interventions to promote maturation. Turmel-Rodrigues L, Pengloan J, et al: Treatment of stenosis and thrombosis in haemodialysis fistulas and grafts by interventional radiology. Vascular Access 2006 Work Group: Clinical practice tips for vascular access. Wystrychowski G, Kitzler T, Thijssen S, et al: Impact of swap of vascular entry sort on key clinical and laboratory parameters in persistent hemodialysis sufferers. Allon M, Bailey R, Ballard R, et al: A multidisciplinary approach to hemodialysis entry: potential analysis. Roy-Chaudhury P, Arend L, Zhang J, et al: Neointimal hyperplasia in early arteriovenous fistula failure. Roy-Chaudhury P, Wang Y, Krishnamoorthy M, et al: Cellular phenotypes in human stenotic lesions from haemodialysis vascular entry. Lee T: Novel paradigms for dialysis vascular access: downstream vascular biology-is there a ultimate frequent pathway Tonelli M, James M, Wiebe N, et al: Ultrasound monitoring to detect entry stenosis in hemodialysis patients: a systematic evaluate. Katsanos K, Karnabatidis D, Kitrou P, et al: Paclitaxel-coated balloon angioplasty vs. McDougal G, Agarwal R: Clinical efficiency traits of hemodialysis graft monitoring. Ascher E, Gade P, Hingorani A, et al: Changes within the practice of angioaccess surgery: impression of dialysis outcomes high quality initiative recommendations. Asif A, Cherla G, Merrill D, et al: Conversion of tunneled hemodialysis catheter-consigned sufferers to arteriovenous fistula. Wong V, Ward R, Taylor J, et al: Factors associated with early failure of arteriovenous fistulae for hemodialysis access. Turmel-Rodrigues L, Mouton A, Birmele B, et al: Salvage of immature forearm fistulas for haemodialysis by interventional radiology. Faiyaz R, Abreo K, Zaman F, et al: Salvage of poorly developed arteriovenous fistulae with percutaneous ligation of accent veins. Turmel-Rodrigues L, Pengloan J, Rodrigue H, et al: Treatment of failed native arteriovenous fistulae for hemodialysis by interventional radiology. Lee T, Barker J, Allon M: Needle infiltration of arteriovenous fistulas in hemodialysis: risk elements and penalties. Lee T, Barker J, Allon M: Tunneled catheters in hemodialysis sufferers: reasons and subsequent outcomes. Pourchez T, Moriniere P, Fournier A, et al: Use of Permcath (Quinton) catheter in uremic patients in whom the creation of conventional vascular access for hemodialysis is troublesome. Shaffer D: Catheter-related sepsis complicating long-term, tunnelled central venous dialysis catheters: administration by guidewire exchange. Tanriover B, Carlton D, Saddekni S, et al: Bacteremia related to tunneled dialysis catheters: comparability of two remedy strategies. Buriankova E, Kocher M, Bachleda P, et al: Endovascular therapy of central vein stenoses in patients with dialysis shunts. Maskova J, Komarkova J, Kivanek J, et al: Endovascular treatment of central vein stenoses and/or occlusions in hemodialysis sufferers. Leon C, Asif A: Arteriovenous entry and hand ache: the distal hypoperfusion ischemic syndrome. Krishnasami Z, Carlton D, Bimbo L, et al: Management of hemodialysis catheter-related bacteremia with an adjunctive antibiotic lock resolution. Vardhan A, Davies J, Daryanani I, et al: Treatment of haemodialysis catheter-related infections. Fernandez-Hidalgo N, Almirante B, Calleja R, et al: Antibioticlock remedy for long-term intravascular catheter-related bacteremia: outcomes of an open, non-comparative study. Appelgren P, Ransjo U, Bindslev L, et al: Surface heparinization of central venous catheters reduces microbial colonization in vitro and in vivo: results from a prospective, randomized trial. Jain G, Allon M, Saddekni S, et al: Does heparin coating improve patency or scale back infection of tunneled dialysis catheters Comert M, Borazan A, Kulah E, et al: A new laparoscopic method for placement of a everlasting peritoneal dialysis catheter: the preperitoneal tunneling method. Soontrapornchai P, Simapatanapong T: Comparison of open and laparoscopic secure placement of peritoneal dialysis catheters. Nebel M, Marczewski K, Finke K: Three years of experience with the swan-neck Tenckhoff catheter. Hergessel O, Felten H, Andrassy K, et al: Safety of ultrasoundguided percutaneous renal biopsy-retrospective evaluation of 1090 consecutive cases. Sedlacek M, Teodorescu V, Falk A, et al: Hemodialysis access placement with preoperative noninvasive vascular mapping: comparability between sufferers with and with out diabetes. It seems also to play a protecting position in surveillance for altered normal cells, similar to ones which have undergone malignant transformation or those who turn into reactive to self-tissue corresponding to in autoimmune illnesses. Many necessary components of immunity that are ancient in evolutionary time are described as parts of natural or innate immunity. In distinction, immune reactants that specifically acknowledge overseas molecules or antigens from the microbial world are generated on account of an adaptive immune response. The main components of such antigenspecific adaptive immunity are immunoglobulins, which are made by B cells, and (thymus-dependent) T cells. The innate immune response, initially triggered by ischemiareperfusion harm related to transplantation, is capable of driving immune cells to the goal harm web site and augmenting the antigen-specific immune response, thus contributing finally to graft destruction. The first successful kidney transplantation was performed in 1954 on the Peter Bent Brigham Hospital in Boston, Massachusetts, between equivalent twins. In the Nineteen Sixties, recognition of the immunosuppressive properties of azathioprine together with corticosteroids made it attainable to efficiently perform transplant surgical procedures between nonidentical donors and recipients. First, the immune system should not respond to any self-antigens, which it does principally via the mechanisms of self-tolerance. Second, nonself (foreign) antigens derived from quite a few sources, together with pathogens and tumor cells, have to be successfully acknowledged to forestall infection and malignancy. In this paradigm, the immune system simply acknowledges transplanted tissues as nonself, inflicting allograft rejection. The final aim of clinical transplantation is to develop protocols to induce particular tolerance to the graft, in order that the immune system is regulated to settle for the allograft as self without maintenance immunosuppression. Whereas the T cell response to a conventional antigen may be experimentally detected only after previous immunization, an allogeneic response, as assayed in a combined lymphocyte culture in vitro, could be readily detected in previously unimmunized (naive) lymphocytes. At least a half of the basis for the higher magnitude of the allogeneic response is the increased frequency of responding cells. For example, the frequency of particular T cells to typical antigens is roughly 1 in 104 to 105, whereas the frequency responding throughout allogeneic stimulation could be as excessive as 1%.
Order lopressor 25 mg with mastercard
Elastic recoil refills the pump tubing after the roller has passed hypertension first aid lopressor 100 mg order without a prescription, readying it for the following roller pulse pressure below 20 lopressor 12.5 mg buy lowest price. Because of the elastic recoil and because most pumps have solely two or three rollers, blood move through the dialyzer is pulsatile. Increasing the variety of rollers makes the circulate much less pulsatile however increases the chance of hemolysis and injury to the pump segment. An different configuration of the dialysate supply system allows using a single needle within the vascular access or a single-lumen catheter for dialysis. The benefit is much less trauma to the vascular entry, particularly during preliminary cannulation of a model new fistula, and potentially reduced dialysis catheter use after surgical revision of a vascular entry. Accepted ranges for arterial inflow pressures are -20 to -80 mm Hg, but may be as little as -200 mm Hg when blood circulate rate (Qb) is excessive. The distal or venous strain monitor gauges the resistance to blood return within the vascular access, and acceptable values vary from +50 to +200 mm Hg. When the higher or lower limits of arterial or venous pressures are exceeded, an alarm sounds, and the blood pump turns off. Blood clotting within the dialyzer, kinking or clotting in the venous blood strains, improperly positioned venous needles, infiltration of a venous needle, or venous outflow stenosis could cause excessive venous pressures. Excessively excessive pressures anyplace within the blood compartment might rupture the dialyzer membrane or disconnect the blood circuit, resulting in an abrupt lower in pressure in the blood circuit. The automated shutoff of the blood pump in this circumstance is doubtlessly lifesaving. Two additional security devices, the venous air entice and the air detector, are situated within the blood line distal to the dialyzer. Air may enter the blood circuit by way of loose connections, improper arterial needle place, or the saline infusion line. The venous air lure prevents any air that will have entered the blood circuit from returning to the affected person. If air remains to be detected within the venous line after the air entice, the machine alarms, and a relay swap turns off the blood pump. These safety features prevent air embolism, which carries a high mortality rate, especially if not instantly recognized. However, microbubbles fashioned during dialysis could escape detection and lodge in organs such as the mind and lungs, possibly contributing to the upper incidence of pulmonary hypertension and cognitive decline noticed in dialysis recipients. Hemodialyzers affect the effectivity and the quality of dialysis via their membranes, which decide their K0A value, and through the blood and dialysate flow rates, which decide the clearance values (see additionally Factors that Affect Clearance in a Flowing System) (Table sixty five. Virtually all of the commercial dialyzers out there in the United States are hollow-fiber dialyzers. Such hemodialyzers are constructed with a cylindrical plastic casing (usually polycarbonate) that encloses a number of thousand hollow-fiber semipermeable membranes stretched from one finish to the opposite and anchored at every finish by a plastic potting compound, usually polyurethane. Along with the semipermeable membrane, the potting compound separates the blood compartment from the dialysate compartment, where dialysate flows between and around each fiber. Blood flows to or from the open end of each fiber via a removable header hooked up to the blood tubing. Apart from decreasing blood priming quantity, the hollow-fiber design additionally improves the efficiency of solute trade by increasing the contact area between blood and dialysate. In addition to the capability of the membrane to activate blood components, its absorptive capability can affect its biocompatibility. Some synthetic membranes, similar to polyacrylonitrile, are extra hydrophobic, bind proteins to a greater extent, and will ameliorate bioincompatible inflammatory reactions via their capacity to bind anaphylatoxins such as C3a and C5a and cytokines. Studies evaluating the relative biocompatibility of substituted cellulose versus synthetic membranes reported no distinction. In basic, the thinner and extra porous the membrane, the extra environment friendly is the transport of solutes and fluid throughout it. The urea K0A (or clearance) of the dialyzer describes its capability to remove low-molecular-weight substances; the vitamin B12 and 2-microglobulin (2M) K0A (or clearance), its capacity to remove higher-molecular-weight substances; Propertiesofthe solute Bloodside Dialysateside, Increases;, decreases. The potting compound absorbs chemical compounds used to disinfect newly manufactured dialyzers. Two major classes of membrane material can be found commercially: (1) cotton fiber, or cellulose-based membranes, and (2) synthetic membranes. Although these membranes are thicker, they are often rendered more permeable than the cellulose membranes, yielding larger fluid and solute removing. The fascinating increase in solute transport associated with larger membranes may be achieved by growing the length, increasing the number, or lowering the diameter of the hollow fiber,176 however every maneuver has undesirable effects when carried too far. Smallerdiameter fibers can offset this disadvantage, however because the fiber diameter decreases, resistance to blood flow will increase, enhancing not only filtration but in addition backfiltration and clotting. Because of those antagonistic effects, the minimal acceptable inner fiber diameter is a hundred and eighty �m. In the late Eighties, with the advent of extra permeable dialyzer membranes, improved strategies to cut back bacteriologic contamination of bicarbonate dialysate (see later), more precise ultrafiltration control, and extra reliable vascular access to obtain enough blood move, therapy times decreased to 2 to three hours three times weekly within the United States. These substituted cellulose and artificial membranes ushered in the era of the high-efficiency and high-flux dialysis. In essence, both forms of dialyzers have improved solute and fluid clearance over that with standard hemodialyzers and reap the benefits of higher blood and dialysate flow charges to scale back dialysis time whereas maintaining an enough dose. High-efficiency dialyzers have a better K0A and a better clearance of small molecules, corresponding to urea, than normal dialyzers (see Table sixty five. High-flux dialyzers have a highly permeable membrane for bigger molecules, similar to vitamin B12 and 2M, and have the next Kf than highefficiency dialyzers, but not essentially high urea clearances (see Table 65. As evident from the foregoing dialogue, the 2 dialyzer designs incessantly overlap, hence the imprecision (see Table 65. High-efficiency and high-flux dialyzers contain both substituted cellulose or an artificial membrane. Both highefficiency and high-flux types of dialysis require the utilization of bicarbonate dialysate and volume-controlled filtration. When acetate was used as a base, its price of diffusion into blood exceeded the metabolic capacity of the physique, leading to acidosis, vasodilation, and intradialytic hypotension (see "Dialysate Composition" section). The latest meta analyses conclude that convective therapies may scale back intradialytic hypotension201,212,213 and cardiovascular mortality,201,213 but additional high-quality randomized and controlled research addressing the effect of convective quantity on outcomes are needed. Most dialysis clinics use a single-pass delivery system, which discards the dialysate after a single passage via the dialyzer, and a single-patient supply system, which prepares dialysate individually and continuously at every affected person station by mixing liquid concentrates with a proportionate volume of purified water. In this design, either the dialysate is combined in an area separate from patient care after which piped to each affected person station or the concentrate is piped to each station before mixing. These centralized systems decrease affected person care costs and reduce staff back injuries from carrying the person concentrate jugs. However, a significant drawback is the shortcoming to modify the dialysate concentration of electrolytes similar to calcium and potassium for individual patients. If the dialysate is too sizzling, protein denaturation (>42� C) and hemolysis (>45� C) happen.
Purchase 25 mg lopressor free shipping
The diploma of proteinuria in preeclampsia can range broadly prehypertension young discount 12.5 mg lopressor with mastercard, from minimal to nephrotic range blood pressure medication kinds 50 mg lopressor generic free shipping. New-onset proteinuria is especially helpful among women with persistent hypertension to diagnose superimposed preeclampsia (see Table 49. However, amongst ladies with underlying proteinuria, different signs of preeclampsia, corresponding to elevated transaminases, thrombocytopenia, and cerebral indicators and symptoms, are extra helpful to diagnose superimposed preeclampsia. Still, the sudden onset of extreme edema, particularly in the palms and face, could be an essential presenting symptom in this in any other case insidious disease and will immediate analysis. It has been instructed that hyperuricemia might contribute to the pathogenesis of preeclampsia by inducing endothelial dysfunction60 or by impairing trophoblast invasiveness, a key element in placental vascular remodeling. Pulmonary edema complicates 2% to 3% of extreme preeclampsia34 and may lead to respiratory failure. Up to a 3rd of eclampsia cases occur postpartum, generally days to weeks after delivery. Most preventable errors in preeclampsia administration resulting in maternal dying contain inattention to blood stress control and signs of pulmonary edema. Worldwide, preeclampsia is associated with a perinatal and neonatal mortality price of 10%74; as with maternal mortality, the chance of neonatal mortality will increase considerably for preeclampsia presenting earlier in gestation. Neonatal demise is most commonly because of iatrogenic untimely supply undertaken to preserve the well being of the mom. However, normalization of blood stress and proteinuria typically takes days to weeks. The American Heart Association guidelines include a historical past of preeclampsia as a risk factor for heart problems in women. Kaplan-Meier plot of the cumulative chance of survival without admission to the hospital for ischemic coronary heart disease or demise from ischemic heart disease in ladies with and withoutahistoryofpreeclampsia. Preeclampsia and heart problems share many threat components, similar to continual hypertension, diabetes, weight problems, renal illness, and the metabolic syndrome. Still, the rise in long-term cardiovascular mortality holds even for girls in whom preeclampsia develops in the absence of any overt vascular threat elements. Whether these observations result from vascular injury or persistent endothelial dysfunction caused by preeclampsia, or just reflect the widespread risk components for preeclampsia and cardiovascular disease, stays speculative. Regardless of etiology, it is recommended that girls who expertise preeclampsia, especially with preterm birth or intrauterine progress restriction, receive screening for potentially modifiable cardiovascular and kidney illness danger elements (hypertension, diabetes mellitus, hyperlipidemia, obesity) on the postpartum obstetrician go to and yearly thereafter. Abnormal uterine artery Doppler ultrasound findings, consistent with decreased uteroplacental perfusion, are noticed earlier than the scientific onset of preeclampsia. However, proof for a causative position for placental ischemia alone stays circumstantial, and several observations call the speculation into question. For example, the animal models based on uterine hypoperfusion fail to induce a quantity of of the multiorgan options of preeclampsia, together with seizures, elevated liver enzyme values, and thrombocytopenia. It could additionally be that the placental ischemic injury that accompanies late-stage preeclampsia is a secondary event. These invasive fetal cells replace the endothelial layer of the uterine vessels, remodeling them from small-caliber resistance vessels to flaccid, high-caliber capacitance vessels. The medical manifestations of preeclampsia replicate widespread endothelial dysfunction resulting in vasoconstriction and end-organ ischemia. Dozens of serum markers of endothelial activation are deranged in girls with preeclampsia, together with von Willebrand antigen, mobile fibronectin, soluble tissue factor, soluble E-selectin, platelet-derived growth issue, and endothelin. Systemic vascular resistance is higher and cardiac output is lower than in regular pregnancies. Women with preeclampsia have impaired endothelium-dependent vasorelaxation, which has been noted prospectively prior to the onset of hypertension and proteinuria114 and persists for years after the preeclampsia episode. The presence of cerebral edema in eclampsia correlates with markers of endothelial harm but not the severity of hypertension,124 suggesting that the edema is secondary to endothelial dysfunction rather than a direct result of blood pressure elevation. The risk of preeclampsia is inversely proportional to the size of cohabitation,132 and oral tolerance to paternal antigens through oral intercourse and swallowing is associated with decreased threat. Several novel isoforms of sFlt1 have been described, but the precise position of the various varieties in human illness continues to be being investigated. This response may result in failure of fetal cells to successfully invade the maternal vessels during placental vascular growth. Observational studies suggest that preeclampsia danger will increase in circumstances of exposure to novel paternal antigens, not solely in first pregnancies but additionally in pregnancies with new partners129 and with lengthy interpregnancy interval. Although the glomerular capillary endothelial cell appears to be the primary glomerular target in preeclampsia, the podocyte is clearly affected in extreme illness, as evidenced by podocyturia throughout clinical illness and even before overt proteinuria. Renal autopsy examination in women who died of preeclampsia demonstrates markedly reduced podocyte expression of nephrin,one hundred seventy and serum from preeclamptic ladies reduces nephrin expression by cultured podocytes. Higher sFlt1 levels have been noted in first than in second pregnancies,173 in twin than in singleton pregnancies,174,one hundred seventy five in ladies with prior preeclampsia,176 and in girls carrying fetuses affected by trisomy 5000 Mean sFlt1 focus (pg/mL) 4000 3000 2000 1000 zero Gestational age (wk) Women with scientific pre-eclampsia P zero. In the case of twin pregnancies, the elevated sFlt1 production seems to be as a result of higher placental mass somewhat than placental ischemia. This pattern might mirror a physiologic anti-angiogenic shift in the placental milieu towards the end of being pregnant, similar to completion of the vasculogenic phase of placental development. It is intuitive to hypothesize that placental vascular growth may be regulated by a neighborhood stability between proangiogenic and anti-angiogenic components and that excess antiangiogenic sFlt1 in early gestation might contribute to inadequate cytotrophoblast invasion in preeclampsia. In this case, placental ischemia, quite than causative, might reflect that the placenta is the earliest organ affected by this derangement of angiogenic stability. Animal fashions of preeclampsia based mostly on induction of uteroplacental ischemia are characterized by increased endogenous sFlt196,183 and sEng. Heme oxygenase 1 and its downstream metabolite, carbon monoxide, act as a vascular protective factor by inhibiting the manufacturing of sFlt1. In addition to angiogenic alterations, women in whom preeclampsia develops also have evidence of insulin resistance. For example, lack of adequate antenatal care is strongly related to poor outcomes, including eclampsia and fetal dying. Higher blood pressure in the first or second trimester, even within the absence of overt hypertension, is related to elevated threat for preeclampsia in wholesome nulliparous girls. Presumably on account of failed placental vascular reworking, preeclampsia is associated with elevated placental vascular resistance and uterine artery waveform abnormalities in the second trimester, as measured by uterine artery Doppler ultrasonography. Test performance varies widely amongst research due to variations in populations studied, gestational age at the time of measurement, definition of an abnormal result, and severity and timing of preeclampsia detected: Sensitivities and specificities vary from 65% to 85%. Some knowledge recommend that there may be promise in combining uterine artery Doppler ultrasonography with measurement of serum biomarkers in screening for preeclampsia. Alterations in circulating ranges of the angiogenic components sFlt1 and sEng happen weeks previous to the onset of preeclampsia and may be useful for screening and/or diagnosis. Later research have suggested that circulating angiogenic elements in plasma or serum can be utilized to differentiate preeclampsia from different diseases that mimic preeclampsia, corresponding to chronic hypertension, gestational hypertension, lupus nephritis, and chronic kidney disease. Aspirin and different antiplatelet brokers have been evaluated in dozens of trials for the prevention of preeclampsia, each in high-risk teams and in wholesome nulliparous women.
Guelder Rose (Cramp Bark). Lopressor.
- Are there safety concerns?
- Cramps, muscle spasms, menstrual cramps, cramps during pregnancy, use as a kidney stimulant in urinary conditions which involve pain or spasms, cancer, hysteria, nervous disorders, and many other conditions.
- Dosing considerations for Cramp Bark.
- How does Cramp Bark work?
- What is Cramp Bark?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96728
Lopressor 12.5 mg generic amex
The amino acid sequence variable areas are on the first (1) and second (2) domains prehypertension caffeine lopressor 25 mg overnight delivery. Class I molecules are expressed on almost all nucleated body cells blood pressure omron discount 25 mg lopressor with mastercard, including the endothelium of blood vessels. Some organ-specific anatomic variations happen in endothelial expression, and in states of active inflammation the density of class I may be domestically increased. Each locus product in a given individual bears a unique-so-called private-antigenic epitope plus further public epitopes which may be shared more widely among the many population. This accomplishment afforded visualization of how the amino acid sequence pertains to the folding of the chains into a three-dimensional structure. The two distal membrane domains, 1 and 2, kind a groove along the top surface of the molecule facing away from the cell membrane. In the crystallographic research, the groove, roughly 25 � lengthy and 10 � wide, contained an unidentified molecule that in subsequent research was shown to symbolize the sure peptide fragment, eight to nine amino acids lengthy. These peptides have an extended linear core construction, and binding is to a large measure determined by side-chain interactions. The websites that determine whether or not a given peptide binds may confer a conformational change on the fragment. Peptides present in eluates from class I crystals or purified molecules are usually eight or nine residues in size. Their origin is in the intracellular pool of polypeptides derived from metabolic turnover of housekeeping proteins or intracellular infections such as viruses. There is selective proteolysis and transmembrane transport from lysosomal compartments into the Golgi, where octamer or nonamer peptides are positioned at school I binding sites before transport to the cell floor. Generally, a optimistic response is marked by cell lysis within the presence of rabbit complement. In addition, more broadly reactive antisera, originally thought to comprise a quantity of antibodies in mixture, might have reactivity to the general public determinants. Although there are a quantity of examples of monoclonal antibodies that will substitute for human antisera, a giant quantity of monoclonal antibodies react in a "public" style, but not necessarily in the identical patterns that human antisera do. The latter are generally directed to class I incompatibilities and injure applicable target cells after direct cell-to-cell contact is initiated by T cell�antigen receptors. When cytotoxic T cells are examined in opposition to a large number of individuals typed by classical serologic strategies, an excellent, but not perfect, correlation is noticed overall. Some antigenic websites, or epitopes, recognized by T cells are literally totally different from these on the same class I molecule which may be acknowledged by antibodies. Loglinear plots of allograft survival all the time present a straight-line decline after the primary year, which makes it possible to calculate a half-life and to project survival rates over time. Avoiding ischemic and storage injury of organs from living donors definitely enhances outcomes as in contrast with those from deceased donors. There is appreciable opportunity both for matching extra circumstances and for avoiding fully mismatched allografts. Because of the size of the national pool available, approximately 15% to 20% of deceased donor kidneys are actually shared on this foundation. In subsequent years, however, the affect on allograft survival of the three loci was discovered to be roughly equal and additive. The more effective immunosuppressive remedy in widespread use right now produces 1-year deceased donor allograft survival charges as high as those related to one-haplotype matched residing, associated donors. These outcomes are in line with the steady improve in early allograft survival and late allograft survival with newer and more powerful immunosuppressive brokers. Although 1-year allograft survival rate has steadily improved to more than 95% over the past few decades with better immunosuppressant strategies, this has not been efficiently translated to improved long-term kidney allograft survival. Five-year overall adjusted allograft survival of extended standards donor, non�extended criteria donor, and residing donor kidney recipients is simply 57%, 72%, and 81%, respectively. Patients experiencing an acute rejection episode have shorter long-term allograft survival. It must be famous that the diploma of mismatch was not in itself directly predictive of early rejection, however it did predict the prognosis as quickly as a rejection episode had occurred. Acute vascular rejection has poorer long-term consequence than less severe tubulointerstitial rejection. Multiple acute rejection episodes are associated with a higher risk for persistent allograft harm. A poor long-term consequence is significantly more common in patients who had multiple acute rejection episode in comparison with these with just one episode (34. Likewise, a single, late acute rejection episode (occurring >3 months after transplantation) carries a much greater danger for allograft failure than early (<3 months) acute rejections. Studies have shown that patients with acute rejection episodes who recovered their baseline kidney operate to greater than 95% at 1 year submit transplantation had significantly larger 6-year allograft survival in contrast with their counterparts who had less than 75% baseline restoration. Alternatively, the rejection tempo may be intrinsically more highly effective with more mismatched antigens. Therefore it seems that evidently a break in self-tolerance could additionally be elicited after transplantation, resulting in the generation of these autoantibodies. They are expressed on the cell surface of a restricted variety of cell types, including endothelial cells, epithelial cells, fibroblasts, dendritic cells, and activated T and B lymphocytes. The A and B groups are glycosylated differentially, whereas group O lacks the enzymes essential for glycosylation. Thus they may cause hyperacute rejection of vascular allografts because of preformed pure antibodies. Specifically, people with group A or B sorts produce natural antibodies to the opposite type, and those with group O produce antibodies to each A and B. Allograft rejection because of red blood cell type mismatching can be readily prevented by routine blood typing earlier than transplantation. Both pathways have been shown in experimental animals to contribute independently to allograft rejection. Other important but poorly understood mechanisms that will contribute to allograft destruction embody nonspecific tissue injury and restore and allograft cell apoptosis. With the introduction of erythropoietin-stimulating brokers, the necessity for blood transfusions before transplantation has dramatically diminished, and this has helped in the reduction of sensitization in potential transplant recipients. Immune cells, as part of the immune surveillance process, move from the circulatory system via the endothelium and into tissues before returning by way of the lymphatic system into the circulation. The inevitable tissue harm that occurs during transplantation ends in a non�antigen-specific inflammatory response, which tremendously will increase leukocyte recruitment (including T cells). This in turn is mediated through interactions between surface molecules (known as adhesion molecules) and their receptors on endothelial cells and leukocytes, and likewise by way of the secretion and binding of small soluble proteins known as chemokines. The website of alloantigen recognition had been believed to be to the allograft itself, but data appear to indicate that antigen recognition might happen in lymphoid tissues. The context of antigen presentation, most strongly outlined by the sort of cell that presents antigen, is also more and more recognized as important in whether or not the T cell mounts an aggressive or passive response to the antigen. Provision of signal 1 alone leads as an alternative to a state of T cell unresponsiveness or "anergy. These transcription components are answerable for the elevated and, in some cases, decreased expression of quite so much of gene products related to T cell activation. First, they roll alongside the vessel wall through interactions between selectins on the endothelium and receptors on immune cells.
Lopressor 100 mg cheap line
The cysts are emphasised arrhythmia heart attack generic 25 mg lopressor visa, illustrating that cysts smaller than 3 mm could be detected blood pressure bottom number is high order lopressor 100 mg fast delivery. Genetic testing can be utilized when the imaging outcomes are equivocal and when a definite diagnosis is required in a youthful individual, similar to a potential residing related kidney donor. Moreover, the take a look at results are oblique and can be confounded by de novo mutations, mosaicism, and bilineal illness. Mild to reasonable persistent proteinuria (150-1500 mg/day) could additionally be present in a major variety of sufferers in the middle to late stages of the disease. The rates of change of whole kidney and complete cyst volumes and of right and left kidney volumes have been strongly correlated. It has not been decided whether or not the defect is attributable to disruption of the medullary structure by the cysts or to a mobile defect instantly linked to the disruption of the polycystin perform. Newer studies counsel that the urinary concentrating defect and elevated vasopressin values could contribute to cystogenesis. Defective medullary trapping of ammonia and transfer to the urine brought on by the concentrating defect could contribute to the low urine pH values, hypocitric aciduria, and predisposition to stone formation. The linearity of the 4 measurements for every affected person within the 3 years of follow-up is according to an exponential development process. Twenty-four-hour ambulatory blood pressure monitoring of children or younger adults without hypertension could reveal blood strain elevations, attenuated nocturnal blood strain dipping, and exaggerated blood pressure response throughout exercise, which can be accompanied by left ventricular hypertrophy and diastolic dysfunction. The presence of hypertension additionally increases the risk of fetal and maternal problems during pregnancy. Some patients have continual flank ache with out an identifiable etiology aside from the cysts. If signs last more than 1 week or if the initial episode occurs after the age of 50 years, investigation to exclude neoplasm should be undertaken. Nuclear imaging (67Ga or 111In-labeled leukocyte scans) may be helpful, but false-negative and false-positive results are possible. Symptoms usually brought on by massive enlargement of the liver or by mass effect from a single or a limited variety of dominant cysts include dyspnea, early satiety, gastroesophageal reflux, and mechanical lower again ache. It is unsure whether or not the reported association of carcinoma of the pancreas represents greater than probability. Arachnoid membrane cysts are asymptomatic however may enhance the chance for subdural hematomas. Focal findings such as cranial nerve palsy and seizure result from compression of native constructions. Subtle alterations in polycystin function could improve the smooth muscle dysfunction from getting older, which is believed to underlie the development of diverticula. A small prospective research from the University of Colorado showed that rigorous blood strain control caused a larger lower in left ventricular mass without a detectable impact on renal perform. Laparoscopic renal denervation or thoracoscopic sympathosplanchnicectomy can be thought-about, notably in polycystic kidneys with out giant cysts. Arterial embolization is an alternative when the surgical danger is high, however its role has not been fully defined. Cyst Hemorrhage Cyst hemorrhages are often self-limiting and reply to conservative administration with mattress rest, analgesics, and hydration. The antfibrinolytic agent tranexamic acid has been successfully utilized in some cases, but no controlled research of its use have been performed282 and the dose needs to be decreased within the presence of renal insufficiency. Reassurance, life-style modification, avoidance of aggravating activities, tricyclic antidepressants, and pain clinic interventions corresponding to splanchnic nerve blockade with local anesthesia or steroids may be helpful. When a number of cysts contribute to ache, laparoscopic or surgical cyst fenestration via lumbotomy or flank incisions could also be Cyst infections are sometimes difficult to treat. If fever persists after 1 to 2 weeks of appropriate antimicrobial therapy, percutaneous or surgical drainage of infected cysts or, in the case of end-stage polycystic kidneys, nephrectomy ought to be undertaken. Pretransplantation nephrectomy, commonly used up to now, has fallen out of favor. When nephrectomy is indicated, hand-assisted laparoscopic nephrectomy is associated with much less intraoperative blood loss, much less postoperative ache, and faster recovery than open nephrectomy and is increasingly getting used. When a hepatic cyst infection is suspected, any cyst with unusual look on an imaging study ought to be aspirated for diagnostic purposes. Long-term oral antibiotic suppression or prophylaxis should be reserved for relapsing or recurrent instances. Antibiotics of alternative are trimethoprim-sulfamethoxazole and the fluoroquinolones, that are effective against the typical infecting organisms and concentrate in the biliary tree and cysts. Estrogens are likely to contribute to cyst development, but the use of oral contraceptive brokers and postmenopausal estrogen substitute therapy are contraindicated provided that the liver is significantly enlarged and the risk for additional hepatic cyst growth outweighs the advantages of estrogen therapy. Options embody percutaneous cyst aspiration and sclerosis, laparoscopic fenestration, open surgical hepatic resection/cyst fenestration, selective hepatic artery embolization, and liver transplantation. Laparoscopic fenestration could be thought-about for giant cysts which would possibly be more prone to recur after ethanol sclerosis or if a quantity of cysts are current that might require a number of percutaneous passes to be treated adequately. When an asymptomatic aneurysm is found, a advice on whether to intervene is dependent upon its size, site, and morphology; prior history of subarachnoid hemorrhage from one other aneurysm; patient age and general health; and whether the aneurysm is coilable or clippable. Among unruptured noncavernous phase aneurysms less than 7 mm in diameter, the rupture dangers were larger among patients who had a previous subarachnoid hemorrhage from one other aneurysm. Morning and afternoon cut up 45/15-mg doses had been titrated at weekly intervals to 60/30 and 90/30 mg. Twenty-three p.c of tolvaptan-treated subjects withdrew from the trial, 15% because of adverse events, together with aquaresis-related signs in 8%, as compared with 14%, 5%, and zero. Of the subjects assigned to tolvaptan therapy and completing three years of treatment, 24%, 21%, and 55% had been tolerating doses of 45/15, 60/30, and 90/30 mg, respectively, at the finish of the examine. Seventeen percent of subjects receiving placebo had been unable to tolerate the 90/30 mg dose. The therapy effect was best from baseline to year 1, but also vital from yr 1 to yr 2, and from 12 months 2 to 12 months 3. The analysis of time to development or progression of multiple scientific events (worsening kidney function, severe kidney ache, hypertension, and albuminuria) confirmed fewer clinical events for tolvaptan than for placebo, with a hazard ratio of 0. This outcome was driven by a 61% lower danger of 25% reductions in reciprocal serum creatinine value and a 36% decrease danger of kidney pain events. Tolvaptan additionally decreased the rate of decline of reciprocal serum creatinine worth, from -3. Increases in serum sodium and uric acid were more frequently seen in tolvaptantreated topics. Tolvaptan-treated topics also had more frequent, clinically vital elevations of liver enzymes, leading to discontinuation of tolvaptan in 1. Because somatostatin has a half-life of approximately 3 minutes, extra secure artificial peptides (octreotide, lanreotide, and pasireotide) have been developed for scientific use. Halflives in the circulation are 2 hours for octreotide and lanreotide and 12 hours for pasireotide.
Lopressor 100 mg discount visa
A number of different antihypertensive therapeutic drug classes are effective in the therapy of hypertensive emergencies blood pressure jumps around discount 100 mg lopressor fast delivery. In the urine blood pressure zoladex lopressor 25 mg order visa, 20% is eradicated unchanged, and the rest undergoes hepatic metabolism to inactive metabolites. In renal illness, the plasma half-life is prolonged, and dosage discount is required. Concurrent administration of a -adrenergic antagonist controls these reflex vasodilatory responses. Salt and water retention also occur, and concurrent diuretic administration is usually required. Diazoxide and its metabolites are removed by hemodialysis and peritoneal dialysis, however clearance is comparatively low due to extensive protein binding. Hydralazine is a direct-acting vasodilator and may be given intramuscularly or as a rapid intravenous bolus injection (Table 50. Thiocyanate is essentially excreted in the urine; it has a plasma half-life of 1 week in regular people and accumulates in those with renal insufficiency. The look of drug unresponsiveness could mirror a rise in the focus of free cyanide. In such circumstances, the drug ought to be promptly discontinued and the levels of cyanide measured. Nitroglycerin may dilate epicardial coronary vessels and their collaterals, rising the blood supply to ischemic areas. Nitroglycerin has an instantaneous onset of action but is rapidly metabolized to dinitrates and mononitrates (see Table 50. Because nitroglycerin is absorbed by many plastics, dilution must be carried out solely in glass parenteral answer bottles. Patients with regular or low left ventricular filling stress or pulmonary wedge stress may be hypersensitive to the results of nitroglycerin. Esmolol hydrochloride focus for injection should be diluted to a ultimate focus of 10 mg/ mL. Esmolol shares all of the poisonous potential of the 1-adrenergic antagonists, as previously discussed. After intravenous injection of a loading dose of 250 to 500 mg/kg and then infusion of a upkeep dose ranging from 50 to one hundred mg/kg/min, steady-state blood concentrations are achieved inside 5 minutes (see Table 50. Esmolol has pharmacologic actions similar to these of different 1-selective adrenergic antagonists; it produces adverse chronotropic and inotropic activity. Because the kidneys remove the de-esterified metabolite of esmolol, the drug ought to be used cautiously in sufferers with renal insufficiency. The drug should be administered to sufferers within the supine position to avoid symptomatic postural hypotension. It blocks transmission of impulses at sympathetic and parasympathetic ganglia by occupying receptor websites and by stabilizing the postsynaptic membranes towards the action of acetylcholine liberated from presynaptic nerve endings. Peripheral vascular resistance is decreased, the heart price is usually increased, and cardiac output is decreased due to venous dilation and peripheral pooling of blood. It has a direct onset of motion when administered as a steady infusion (see Table 50. The major disadvantage is that the drug should be administered with the patient supine to avoid profound postural hypotension. Other disadvantages embrace the following: (1) potential for tachyphylaxis after sustained infusion (48 hours); (2) appearance of antagonistic effects associated with parasympathetic and sympathetic blockade; and (3) histamine release. Adverse results include these related to nonselective -adrenergic blockade, as beforehand discussed. The relationship between the intravenous infusion dose and steady-state blood concentrations is linear in patients with gentle to average hypertension and in wholesome volunteers. The initial section is rapid (half-life of 1 minute) and accounts for 85% to 90% of elimination. The commonest opposed events are sinus tachycardia, headache, nausea, and chest discomfort. Fenoldopam is a racemic mixture during which the R isomers are liable for its biologic exercise. It has vasodilatory results on coronary, renal, mesenteric, and peripheral arteries in experimental studies; nonetheless, not all vascular beds reply uniformly. In humans, the drug will increase renal blood move in hypertensive and normotensive topics. Fenoldopam comes in 1-mL ampules that include 10 mg of fenoldopam and is diluted for administration as a constant infusion at a rate of zero. Adverse effects embody reflex enhance in heart price, enhance in intraocular strain, headache, flushing, nausea, and hypotension. The dosages and pharmacodynamic results of rapid-acting oral medicine which may be commonly used within the remedy of hypertensive emergencies are given in Table 50. Investigators O, et al: Telmisartan, ramipril, or each in sufferers at excessive threat for vascular events. Rossing K, et al: Dual blockade of the renin-angiotensin system in diabetic nephropathy: a randomized double-blind crossover study. Bangalore S, et al: Antihypertensive medication and danger of most cancers: network meta-analyses and trial sequential analyses of 324,168 individuals from randomised trials. Poirier L, Lacourci�re Y: the evolving role of -adrenergic receptor blockers in managing hypertension. Kaoukis A, et al: the function of endothelin system in cardiovascular disease and the potential therapeutic views of its inhibition. Rakusan D, et al: Persistent antihypertensive effect of aliskiren is accompanied by lowered proteinuria and normalization of glomerular space in Ren-2 transgenic rats. In addition, potent cerebral vasodilators can conceivably cause an increase in intracranial stress, creating the potential for cerebral edema and attainable herniation. For most hypertensive emergencies, a parenteral drug, corresponding to sodium nitroprusside, is good. Intravenous nicardipine can be used as a outcome of it facilitates coronary vasodilation. Patients with acute aortic dissection are finest handled with a -adrenergic antagonist plus nitroprusside or a ganglionic blocker, corresponding to trimethaphan. Fenoldopam could additionally be useful for patients with kidney disease as a result of it maintains renal blood flow. Kunz R, et al: Meta-analysis: impact of monotherapy and mixture therapy with inhibitors of the renin angiotensin system on proteinuria in renal illness. Mercier K, Smith H, Biederman J: Renin-angiotensin-aldosterone system inhibition: overview of the therapeutic use of angiotensinconverting enzyme inhibitors, angiotensin receptor blockers, mineralocorticoid receptor antagonists, and direct renin inhibitors. Bao G, Gohlke P, Qadri F, et al: Chronic kinin receptor blockade attenuates the antihypertensive effect of ramipril. Hirooka Y, Imaizumi T, Masaki H, et al: Captopril improves impaired endothelium-dependent vasodilation in hypertensive sufferers. Nakamura M, Funakoshi T, Yoshida H, et al: Endotheliumdependent vasodilation is augmented by angiotensin changing enzyme inhibitors in healthy volunteers.