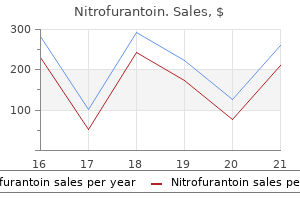
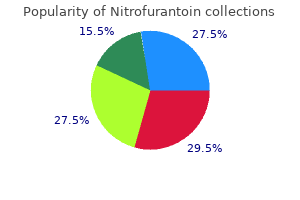
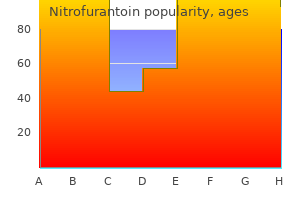
Nitrofurantoin
Nitrofurantoin dosages: 100 mg, 50 mg
Nitrofurantoin packs: 100 pills, 200 pills, 300 pills, 400 pills, 500 pills, 600 pills

Purchase nitrofurantoin 50 mg visa
Similar fibrosis might occur in the retroperitoneum antibiotic resistance news article nitrofurantoin 50 mg buy cheap line, encircling the kidneys and resulting in medicine for uti boots nitrofurantoin 50 mg with visa a progressive obstructive nephropathy. The presence of conduction abnormalities ought to be evaluated by electrocardiography. Lesions contain a dermal infiltrate that features histiocytes, occasional multinucleated large cells which may have the features of Touton cells, and nonspecific inflammatory cells. Systemic illness occurs not often and will contain liver, lung, spleen, lymph nodes, bone, and gastrointestinal tract. Symptomatic visceral involvement may be handled, if needed, with surgical excision, radiation therapy, or chemotherapy. It occurs in adults and will predominantly have an result on ladies, though no rigorous epidemiologic analyses have been performed. Male sufferers are affected extra regularly than female patients, as are people ofAfricanancestry. Associated malignancies include breast and gastric cancers, as properly as hematologic neoplasms. Periorbital areas are the most common website of involvement, however lesions could happen elsewhere on the face, trunk, arms, legs, and genitalia. The most common site of extracutaneous involvement is the eye and might manifest as uveitis or scleritis. Visceral involvement may also occur in quite so much of sites but mostly within the respiratory tract or cardiac buildings. Serum and urine electrophoresis must be carried out to check for the presence of monoclonal gammopathy, and additional hematologic work-up ought to be dictated by the results. Imaging of the chest, abdomen, and pelvis should be performed to assess visceral disease. Symptomatic disease may be treated with corticosteroids, clofarabine, or radiation therapy. Case studies recommend that alkylators corresponding to chlorambucil or melphalan, with or without steroids, may be efficient first-line therapy. Intravenous immunoglobulin has been used a second-line therapy, and lenalidomide has been used in sufferers with monoclonal gammopathy even within the absence of clinically documented a quantity of myeloma. It is a disease of adults, with a median age of analysis for the histiocytic sarcoma subtype within the mid-40s to mid-50s, and no intercourse imbalance. Recent recommendations suggest that the term malignant histiocytosis should be utilized to the complete household of ailments and that the mobile phenotypes should be considered subtypes. Patients might current with symptomatic mass lesions that might be accompanied by fever and weight loss. Onrecognitionofantigen,these effector cells launch perforin-containing cytolytic granules that contribute to lysis of the antigen-expressing goal cell. Under normal situations, goal cell elimination limits antigen publicity, leading to downregulation of the immune response, termed activation-induced cell death. Patients regularly present with a fulminant image offever,cytopenias,andmultiorganfailure,andtheyareoftensuspectedof having septic shock. Bone marrow aspiration frequently, although not at all times, demonstrates hemophagocytosis. As discussed within the subsequent part, the prognosis, particularly in adults, may be challenging. Depending on the websites of disease, efficient approaches might embrace surgical procedure, radiation remedy, or systemic chemotherapy, notably regimens developed for aggressive lymphomas. A spectrum of outcomes may be seen in these sufferers, from spontaneous remission to recurrent and refractory illness. Many acute viral infections are related to hemophagocytosis, and hemolytic anemias are associated with the same finding. In contemplating the diagnosis, a radical history should include details regarding current infections, history of autoimmune disease, underlying malignancy, and underlying immune issues. Patients ought to bear marrow examination, and along with routine research, marrow samples must be sentforflowcytometryandT-cellgenerearrangementstudies. Children with neurologic symptoms obtain intrathecal methotrexate, however that is hardly ever essential in adults. Following completion of the 8-week course, sufferers may be placed on upkeep therapy with the addition of calcineurin inhibitors to intermittent dexamethasone and etoposide, normally as a bridge to stem cell transplantation. Patients with important liver dysfunction can have initial dose reduction of etoposide with dose increases as function improves. However, adult sufferers with refractory or relapsed disease, and individuals who have had life-threatening illness at presentation, ought to be evaluated for transplantation. Therapy prolongation improves end result in multisystem Langerhans cell histiocytosis. Langerhans cell histiocytosis in adults: advances in pathophysiology and remedy. Multicentric reticulohistiocytosis: a multicenter case collection and evaluation of literature. A 58-year-old girl presents with pain in a number of joints and a new rash consisting of nonpruritic yellow-to-brown papules and nodules on her face, ears, and forearms. She tells you that she has misplaced about 10 kilos, unintentionally, over the past four months. In addition to histologic and immunohistologic evaluation of a skin biopsy, probably the most useful diagnostic technique might be: A. Approximately 25% of sufferers with this illness, the majority of whom are women, have an underlying malignancy. A 43-year-old man with no previous medical history presents to the hospital with a 2-month historical past of fevers and evening sweats. Physical examination reveals a cachecticappearing young man with a palpable liver and spleen. A 45-year-old man with a 25 pack-year smoking history presents to the emergency room with chest pain and mild dyspnea. His chest radiograph shows a small pneumothorax together with reticulonodular opacities within the middle to upper lung zones. His common bodily examination is unremarkable except for yellowish plaques in his periorbitalskin. Weekly vinblastine 6mg/m2 plus day by day prednisone 40mg/m2 for six weeks, adopted by the same doses of vinblastine on day 1 and prednisone on days 1 via 5 every 21 days for forty six weeks E. The prevalence of eosinophilic esophagitis seems to be increasing, consistent with an total enhance in the incidence of atopic illness, and has been estimated at 2. Eosinophils are terminally differentiated cells of the myeloid lineage that circulate in low numbers within the peripheral blood. This definition encompasses numerous clinical subtypes that differ in etiology and/or medical manifestations and have prognostic and therapeutic implications (Table 161-1).
100 mg nitrofurantoin buy visa
Fewer than one third of circumstances of anemia in hypothyroidism are macrocytic; otherwise anemia in endocrine deficiency is normocytic treatment for recurrent uti in dogs nitrofurantoin 100 mg on line. Treatment of the underlying deficiency corrects the anemia of endocrine deficiency virus 2014 usa cheap nitrofurantoin 100 mg on line. Beginning across the seventh week of pregnancy, the pink cell mass begins to expand up to 15 to 25% above prepregnancy baseline. At roughly the identical time, the plasma volume begins to increase disproportionately, finally reaching 40 to 50% above baseline throughout weeks sixteen to 24. Lower hemoglobin concentrations or microcytic or macrocytic anemia does require evaluation. The largely probably contributors to anemia in being pregnant are iron deficiency or folate deficiency, demand for both of which is elevated during pregnancy. In the absence of a preexisting deficiency or an increased demand induced by hemolysis, the zero. The prevalence of anemia is three- to four-fold elevated in African Americans over 65 in comparison with individuals of white European ancestry but only slightly elevated in Latino populations. However, gender-specific imply hemoglobin/hematocrit values for older sufferers are practically similar to the overall inhabitants mean values. The elevated frequency of anemia with getting older partly displays age-related declines in renal perform, gastric acidity, and testosterone in males, in addition to an increased frequency of other pathology. In aged people with persistent unexplained anemia and abnormalities in different lineages Normocytic anemias additionally characterize a mixed group of issues. In most other circumstances, they symbolize anemia associated with some other systemic dysfunction. Pure purple cell aplasia presents as an isolated normochromic normocytic anemia with hanging reticulocytopenia. The anemia of inflammation, which is likely the most typical normocytic anemia syndrome after acute blood loss or early iron deficiency, is mentioned in Chapter one hundred fifty. Anemia is a much less frequent complication of polycystic kidney illness due to secretion of erythropoietin by the cysts. The major pathogenetic issue within the anemia of renal insufficiency is erythropoietin deficiency. The use of recombinant erythropoietin (erythropoiesis stimulating agents) has considerably mitigated this drawback, though even in the erythropoietin period 48% of predialysis patients and 28% of hemodialysis patients have hematocrit values <30%. Other mechanisms contributing to the anemia of renal failure are suppression of the erythroid progenitor response to anemia and shortened pink cell survival. Shortened purple cell survival has numerous proposed mechanisms, including decreased ability to regulate mobile oxidative stress, results of toxic metabolites accumulated in uremia, and membrane lipid peroxidation. Erythropoietin concentrations are usually not useful in making a prognosis as a outcome of the similar old suggestions relationship between hemoglobin concentration/hematocrit and erythropoietin secretion is lost. The anemia of renal insufficiency is treated with recombinant erythropoietin or an erythropoietin analog. Iron supplementation ought to be thought of when the transferrin saturation is lower than 30% or serum ferritin concentration is less than 500 ng/mL. Hepcidin results impair iron absorption in renal failure,7 and intravenous iron could additionally be more effective for supplementation than oral iron. Total blood quantity in cirrhosis and other persistent liver ailments is usually elevated 10 to 15%, however could also be expanded as much as 30%. Dilution of the purple cell mass by expanded plasma volume is a major component in the anemia of liver illness. Target cells in liver illness have increased diameter that distinguishes them from the microcytic target cells of hemoglobinopathies or thalassemia. The effectiveness of day by day supplementation with four hundred or 800 microg/day folate in reaching protective red blood folate concentrations in non-pregnant women: a randomized trial. Clonal hematopoiesis of indeterminate potential and its distinction from myelodysplastic syndromes. Optimal dose, timing and ratio of blood products in massive transfusion: results from a scientific evaluate. Causes of macrocytic anemia amongst 628 sufferers: imply corpuscular volumes of 114 and a hundred thirty f L as crucial markers for categorization. The majority of affected people are kids and younger and/or pregnant girls. In the absence of an excretion mechanism, most iron is recycled by macrophages that destroy senescent pink cells. The liver peptide hepcidin regulates iron homeostasis at a systemic degree (Chapter 201). Duodenal enterocytes easily take up dietary heme by way of a receptor; inside the enterocytes, iron is recovered through heme oxygenase. Enterocytes take in nonheme iron much less effectively through a well-studied complex mechanism. Iron stored in duodenal ferritin is lost from the body, with the shedding of mucosal cells into the lumen. Because hepcidin is downregulated in hypoxia, iron absorption is strongly increased by the mixed effects of elevated intestinal iron absorption and iron launch from storage websites in macrophages and hepatocytes. Except for elevated requirements in children and younger or pregnant women, the principle causes of iron deficiency/iron deficiency anemia are inadequate dietary iron consumption, insufficient iron absorption, and persistent blood losses. However, refractoriness to oral iron is extra generally because of defective absorption in gastrointestinal issues. They cause irondeficient erythropoiesis however are "atypical" as a result of iron and ferritin are often discrepant in contrast with traditional iron deficiency. In addition, iron-restricted erythropoiesis happens when iron supply for erythropoiesis is reduced no matter iron stores, as within the presence of high hepcidin levels. Iron could turn out to be limiting in the recovery from acute blood loss, as after main surgery, probably due to the increased wants and the concomitant irritation. For instance, animal studies and clinical knowledge indicate that the guts is very iron dependent and that cardiomyocyte iron deficiency might develop even within the absence of anemia, especially in failing hearts. Because iron deficiency anemia normally progresses slowly, sufferers, particularly if young, might tolerate well even extreme anemia. In aged sufferers, cardiovascular signs corresponding to dyspnea, angina, or coronary heart failure could reveal anemia. The most common hypochromic microcytic anemias are iron deficiency anemia and the thalassemia syndromes (Chapter 153), while more rare are the congenital sideroblastic anemias. The anemia of chronic irritation (Chapter 149) is normally normochromic and normocytic; nevertheless, when long-standing or associated with absolute iron deficiency, it may turn into hypochromic and microcytic. Iron deficiency anemia signifies a extra extreme discount of complete body iron that results in anemia. It is estimated that amongst individuals with anemia (>2 billion worldwide), greater than half have iron deficiency anemia. These anemias are principally brought on by both iron deficiency or hemoglobinopathies, significantly the thalassemia syndromes. In many instances, iron deficiency should be differentiated from the anemia of continual illness or inflammation for which a blood take a look at for the soluble transferrin receptor could be helpful. Treatment for iron deficiency initially requires identification of its cause.
Syndromes
- Bloody or dark urine
- Those with weakened immune systems due to AIDS, diabetes, or medications that suppress the immune system
- Exercise the neck and shoulders frequently when typing, working on computers, or doing other close work.
- Holes (necrosis) in the skin or tissues underneath
- Decongestants, including pseudoephedrine
- Liver disease
- Infertility
- Time it was swallowed
- Fibrinolysis
- Pressure, pain, or spasms in your back or the lower part of your belly
50 mg nitrofurantoin buy with visa
Tests for chronic viral hepatitis and customary genetic causes of persistent liver illness are all unfavorable antibiotics for sinus infection and drinking 100 mg nitrofurantoin buy otc. Liver ultrasonography reveals increased echogenicity of the liver and cholelithiasis with out thickening of the gallbladder wall infection 9gag nitrofurantoin 50 mg buy on line. In addition to cholecystectomy, which of the next choices ought to be really helpful A 51-year-old man presents with three months of painless jaundice, pale stools, and darkish urine, in addition to spiking fevers. Abdominal ultrasound reveals proximal dilation of the intrahepatic bile ducts, and magnetic resonance cholangiopancreatography reveals a constricting mass in the frequent bile duct a quantity of centimeters distal to the junction of the right and left hepatic ducts. After being began on intravenous broad-spectrum antibiotics, the patient is taken to surgery, the place the mass is resected. Two weeks later his whole bilirubin is 14 mg/dL, direct-reacting bilirubin 10 mg/dL, alkaline phosphatase 225, and urine urobilinogen still undetectable. Because of the persistent direct-reacting hyperbilirubinemia and elevated alkaline phosphatase, the surgeon is contemplating taking the affected person again to the working room and re-exploring his biliary tract. Urine bilirubin Answer: E After profitable reduction of continual bile duct obstruction, each the entire bilirubin and the alkaline phosphatase could take a number of weeks to normalize. Although the absence of urobilinogen from the urine on the time of admission reflected full bile duct obstruction, its persistence after 2 weeks of broad-spectrum antibiotic therapy not reflects biliary obstruction, but rather elimination by the antibiotics of the bacteria necessary to convert bilirubin in the gut to urobilinogen. In this case, use of a dipstick that detects bilirubinuria may save the affected person from an pointless second surgical process. A 24-year-old nurse presented to the worker well being department of her hospital complaining of arthralgias, weak point, and fatigue for 2 weeks. Her family history included relatives with rheumatoid arthritis and lupus erythematosus. On physical examination, she was pale, with faintly icteric sclerae and a palpable spleen tip. A lupus erythematosus preparation was negative, but because a direct Coombs test was strongly optimistic, the diagnosis of autoimmune hemolytic anemia was made. Based on her persistent anemia and reticulocytosis, a rheumatologist argued that the present therapy was ineffective and urged rising her prednisone dose to eighty mg/day. The hematologist said that she was primarily cured and urged continuation of the current treatment with follow-up in 2 weeks. Which of the next take a look at results led the hematologist to that correct conclusion Other viruses may cause acute inflammatory liver disease, including members of the Herpesviridae household corresponding to human cytomegalovirus, Epstein-Barr virus, or herpes simplex virus. It is unclear to what extent other viruses, corresponding to parvovirus B19 or human herpesvirus 6, can also trigger acute hepatitis. Patients who present with an acute viral hepatitis syndrome however unfavorable virologic tests are referred to as having non-A-to-E hepatitis, maybe attributable to hepatotropic viruses which have but to be recognized. Antiviral treatment is indicated just for the treatment of acute hepatitis C, because of the excessive risk (50 to 80%) of chronicity. The different causes of acute viral hepatitis are self-resolving in the vast majority of circumstances. Because none of the hepatotropic viruses is cytopathic, liver damage is mediated by a robust cytotoxic T cell�mediated response in opposition to infected hepatocytes that specific viral antigens at their floor. Proinflammatory cytokines, natural killer cells, and antibody-dependent cellular cytotoxicity also seem to play a role in liver necroinflammation. Successful immune elimination may result in viral clearance, which may or may not be associated with lifelong immunity, depending on the infecting agent. The immune response is sometimes so potent that the patient develops subfulminant or even fulminant hepatitis that requires liver transplantation (Chapter 145). In some patients-the proportion varies, based on the virus liable for acute hepatitis-the immune response fails and continual an infection is established (Chapter 140). This incubation period is usually characterized by nonspecific symptoms, including fatigue, nausea, loss of appetite, flulike signs, and/or right higher quadrant ache (Table 139-2). The incubation period is often characterised by leukopenia and relative lymphocytosis. Immune-mediated symptoms, together with rash, hives, arthralgias, angioneurotic edema, and fever, are noticed in 10 to 20% of patients during the preicteric section. During the acute stage of the disease, symptoms could vary extensively, from asymptomatic to subicteric, icteric or severe, and fulminant. On laboratory testing, acute viral hepatitis is characterized by elevated complete and direct serum bilirubin levels and aminotransferase ranges which are often higher than 10 times the higher limit of regular. Cholestatic acute hepatitis is related incessantly with prolonged and fluctuating jaundice and pruritus. After 1 to 3 weeks, on average, both medical and laboratory signs progressively enhance and return to normal. Signs of hepatic failure (Chapter 145), including changes in personality, aggressive conduct, sleeping disorders, and hepatic encephalopathy, characterize fulminant types of acute viral hepatitis. The analysis of acute hepatitis is suspected primarily based on elevated serum aminotransferase levels, which are typically more than 10 times the upper restrict of regular (Table 139-3). Total and direct bilirubin ranges are elevated if the acute hepatitis is subicteric or icteric. Liver biopsy or a noninvasive evaluation of liver inflammation and fibrosis are usually not required. All circumstances of acute hepatitis should be reported to the native, state, or nationwide well being department as soon as possible after diagnosis. Patients with subfulminant or fulminant hepatitis ought to be supported in an intensive care unit setting and evaluated for attainable liver transplantation (Chapter 145). Prognosis is dependent upon the diploma of prolongation of the prothrombin time, in addition to the degree of elevation of the bilirubin and lactate levels. A issue V stage less than 40% or any signs of encephalopathy are indications for hospitalization. Other signs of poor prognosis are persistently worsening jaundice, ascites, and an acute lower within the dimension of the liver. Acute hepatitis A in adults may require hospitalization in as a lot as 13% of cases2; extended courses of 6 to 9 months have been reported in 10% of adult patients with a prognosis of acute hepatitis A. It is presently unclear to what extent totally different genotypes are associated with distinct scientific programs of infection. In developing international locations, an infection usually happens at a young age and a lot of the population has been uncovered and is protected after age 10 years. In developed countries, nonetheless, an infection can happen at any age, and the prevalence of exposed, immune topics slowly will increase with age. In the United States, in accordance with the Centers for Disease Control and Prevention, the incidence of acute hepatitis A declined from 12. Transmission by blood transfusion has been reported, and isolated instances of obvious perinatal transmission have been described.
Nitrofurantoin 100 mg generic with amex
The depth of the evaluation relies on numerous elements virus yahoo email buy nitrofurantoin 50 mg fast delivery, including the age when the primary stone is diagnosed and the frequency of recurrent stones antibiotics for acne wiki nitrofurantoin 50 mg discount mastercard. Treatment for recurrent calcium stones rests on the four pillars of elevated hydration (goal urine volume >2 liters per day), moderation of sodium intake (goal <2000 mg/day), moderation of protein intake (~1 g/kg/day), and an age- and gender-appropriate calcium consumption derived mainly from dairy merchandise and never from dietary supplements. The recurrence price of calcium oxalate nephrolithiasis is about 25% at 5 to 10 years. A number of single-nucleotide polymorphisms, in genes coding for the calcium-sensing receptor, the vitamin D receptor, and osteopontin, and others, have been associated with calcium nephrolithiasis. Overall, 14 monogenic mutations account for 15% of nephrolithiasis/nephrocalcinosis, and genetic components appear to clarify about 20 to 35% of the interindividual variation in excretion of ions critical to stone formation. Urinary oxalate is derived from endogenous metabolism of glyoxylate and ascorbic acid or from dietary sources, such as cocoa, nuts, tea, and sure leafy green greens such as spinach. Additionally, ethylene glycol, a common vehicle antifreeze, is metabolized to oxalate and might trigger excessive urinary oxalate excretion in conjunction with severe metabolic acidosis and renal failure (Chapter 102). Primary hyperoxaluria (Chapter 194) outcomes from defects in hepatic enzymes within the liver glyoxylate pathway; the outcomes are substantial endogenous oxalate production and a marked elevation of urinary oxalate (80 to 300 mg/day). Type 3 main hyperoxaluria, which accounts for about 5% of cases, is a result of mutations within the gene that catalyzes the cleavage of 4-hydroxy-2-oxoglutarate to pyruvate and glyoxylate. Nephrolithiasis and nephrocalcinosis can even result from a selection of monogenic issues, corresponding to Dent disease (X-linked recessive nephrolithiasis; Chapter 119), McCune-Albright syndrome (Chapters 218 and 234), osteogenesis imperfecta kind 1 (Chapter 244), and congenital lactase deficiency (Chapter 131). Citrate inhibits stone formation by combining with calcium to form a soluble advanced that reduces the availability of calcium to bind with oxalate or phosphate. Distal renal tubular acidosis (Chapter 110) promotes the formation of calcium phosphate stones owing to bone demineralization and an alkaline tubular pH. Calcium oxalate kidney stones type on calcium phosphate deposits, termed Randall plaques, which are located in the renal papillae. These calcium phosphate crystals, in the form of apatite, originate across the thin loop of Henle after which extend into the interstitium with out eroding into the tubular lumen or damaging the tubular cells. The stone can break off from the Randall plaque and then migrate to , irritate, and probably obstruct the ureter. Most sufferers with uric acid stones have a decreased urine pH, and some have low urine volumes or elevated urinary uric acid levels. Uric acid stone formers have higher body weight and a higher incidence of insulin resistance and type 2 diabetes mellitus. Insulin resistance also leads to impaired urinary ammonium excretion, thereby ensuing within the excretion of extra hydrogen ions as titratable acids and decrease urine pH, which reduces the solubility of ammonium. Hyperuricosuria may be seen in sufferers who ingest large portions of dietary purine, corresponding to organ meats, shellfish, sure fish. Hyperuricemic issues, together with gout (Chapter 257), myeloproliferative problems, tumor lysis syndrome, and sure inborn errors of metabolism, can also contribute to an increased urinary uric acid. Struvite stones, typically referred to as triple phosphate stones, magnesium ammonium phosphate stones, and infection stones, comprise only about 10 to 25% of all stones however represent the majority of staghorn calculi, which are massive stones that extend past a single renal calyx. Similarly, any patient with urinary stasis, similar to sufferers with neurogenic bladders, indwelling urinary catheters, or spinal twine lesions, is vulnerable to struvite stones. Struvite stones type solely within the presence of each ammonium ions and an alkaline urine (pH 7), which solely occur with urease-producing micro organism. Proteus (Chapter 289) is a typical urease-producing bacterium, but other gram-negative and gram-positive bacteria, corresponding to Klebsiella spp. Although regular folks excrete about 30 to 50 mg of cystine per day, heterozygotes for cystinuria excrete about 400 mg/day, and homozygotes usually excrete about 600 mg/day. Thus, homozygotes must frequently excrete greater than 2 L of urine each day to avoid stone formation. Cystinuria is unrelated to the much more severe disorder cystinosis (Chapter 119), which results in extensive intracellular cystine accumulation. The ache is of abrupt onset and may intensify into extreme, excruciating flank ache. The ache may migrate anteriorly along the stomach and inferiorly to the groin, testicles, or labia majora because the stone moves down the ureter toward the ureterovesical junction. Conversely, even massive calculi may be asymptomatic and be discovered during the investigation of unrelated symptoms. Obstruction brought on by calculi may also be painless, and nephrolithiasis ought to at all times be considered within the differential analysis of unexplained acute or chronic kidney disease (Chapters 112 and 121). Some sufferers have demonstrable flank tenderness, and a uncommon patient with hyperuricemia could have tophi (Chapter 257). However, the bodily examination is most helpful for not exhibiting other potential causes of pain. Ultrasonography is a simple and fast way to detect possible urinary obstruction without exposing the affected person to ionizing radiation. Ultrasound can detect clinically vital renal calculi, with about an 85% sensitivity for detecting the ureteral stones that cause acute symptoms. Based on the density of the stone, it also can often differentiate a calcium-containing stone from a cystine or uric acid stone. Approximately 90% of kidney stones are radiopaque and could additionally be detected on a easy belly radiograph. Unfortunately, nonetheless, the stone is often obscured by stool, vertebrae, or belly fuel, so the sensitivity of a plain belly radiograph is about 55%, and its specificity is just about 75%. Intravenous pyelography has a sensitivity of about 75% and a specificity of more than 90% for detecting renal calculi. Intravenous pyelography can be useful for figuring out structural abnormalities of the urinary tract, such a medullary sponge kidney (Chapter 118), that predisposes to stone formation. It also carries the danger of radiographic distinction materials, which is larger in individuals with underlying renal compromise. If nausea and vomiting forestall the use of oral medication, parenteral medication is typically required. A3 An intravenous option is ketorolac (30 to 60 mg), and an oral possibility is ibuprofen (200 to four hundred mg/dose each 4 to 6 hours with a most every day dose of 1. Oral oxycodone (5 to 15 mg each four to 6 hours as needed) could also be added to ibuprofen for outpatient pain management. Medical Expulsive Therapy Kidney stones 5 mm or smaller have about a 70% probability of passing spontaneously, whereas stones between 5 and 7 mm have a 60% likelihood, stones 7 to 9 mm have a 48% probability, and stones 9 mm or bigger have a 25% probability of passing spontaneously. The patient should be adopted carefully, usually with repeat ultrasound examinations every week or 2 weeks. Expulsive remedy can reduce ureteral spasm and improve spontaneous passage charges by about 50%. Although neither tamsulosin daily nor nifedipine have been effective at reducing the necessity for further therapy to obtain stone clearance in four weeks for sufferers with expectantly managed ureteric colic in some randomized trials, A4 A5 meta-analysis of all trials nonetheless reveals an overall profit for -blockers such as tamsulosin (0.
Nitrofurantoin 50 mg generic without prescription
Ten-year survival charges are extremely age dependent: 85% infection during labor 100 mg nitrofurantoin best, 77% treatment for uti guidelines discount nitrofurantoin 50 mg without prescription, and 66% for recipients in the first, second, and third a long time of life, respectively. Transplantation of syngeneic (twin) stem cells represents the only exception to this rule. In such cases, stem cell transplantation is the best first choice, even in older sufferers. Fludarabine-based conditioning regimens have improved outcomes of matched unrelated donor transplants substantially. Indeed, the enhancements have been encouraging sufficient to recommend strongly that unrelated donor searches be initiated at the time of analysis for any patient younger than 30 years. Adults older than 30 years ought to be thought-about candidates for different donor stem cell transplantation if two makes an attempt at immunosuppressive remedy have failed. Complete responses are defined as the resolution of pancytopenia and the development of regular blood counts. Forty to 60% of these sufferers will relapse in 5 years, however most will reply to a repeated course of immunosuppressive remedy. Some would require persistent immunosuppressive therapy with cyclosporine to stay transfusion unbiased. Because remissions can happen late, 6 months of therapy is required before declaring ist a therapeutic failure. For these in that group whose responses are suboptimal, alternatives are: (a) repeated ist with modifications. For secondcourse ist, response rates are 35% for initially refractory sufferers and 60% for sufferers whose illness initially responded but then relapsed. Bmt = bone marrow transplant; ist = immunosuppressive therapy; ucB = umbilical wire blood. Slowing the infusion after premedication with glucocorticosteroids and antihistamines often solves this downside. Third, it seems clear that an extended interval between analysis of aplastic anemia and the initiation of immunosuppressive therapy is a unfavorable predictor of response. Treatment ought to start as quickly as attainable, actually inside three weeks of preliminary prognosis. A key think about successful management of children and adults with inherited bone marrow failure syndromes is their need for remedy in centers with experience and experience. Pre- and post-transplant management of such patients is advanced and should be tailored to the unique options of each disease. Late morbidity and mortality complicates the management of transplanted telomeropathy sufferers,15 and Diamond-Blackfan anemia sufferers can be managed for long periods of time with steroids alone. Consequently, the exact timing of transplants in patients with telomeropathies and with Diamond-Blackfan anemia has not been established. Glucocorticosteroids in Diamond-Blackfan Anemia Although the mechanism by which glucocorticosteroids induce remissions in patients with Diamond-Blackfan anemia is unknown, practically 80% of patients initially reply. Prednisone therapy is started at 2 mg/kg/day and is tapered after the hemoglobin will increase to 10 g/dL. Most sufferers require a low everyother-day dose, however 15% remain in remission off steroids altogether. Only half of the patients with steroid-resistant extreme anemia survive to the age of forty years. Supportive Care platelet transfusions In the absence of bleeding or infection, platelet transfusions are commonly administered only when the platelet depend declines to 10,000/�L or much less (Chapters 163 and 167), but in the presence of energetic an infection or bleeding, transfusion thresholds are often set at 20,000/�L or larger. As a common rule, nevertheless, the quantity is higher in elderly sufferers than in young sufferers. Adults with underlying cardiopulmonary disease could have symptomatic anemia at 8 g/dL. If persistent transfusion therapy is required, the event of iron overload might require chelation therapy. Matched sibling donor transplants are associated with larger response charges, lower relapse charges, long-term survival charges approximating 80%, and lower incidence of clonal evolution. Immunosuppressive therapy is related to long-term (10-year) survival rates of 70 to 75% in responders. Infection represents the most typical explanation for dying in sufferers of any age handled with either immunosuppression alone or stem cell transplantation. About 35% of sufferers with acquired aplastic anemia have clonal hematopoiesis generally ascertained either cytogenetically or by targeted gene sequencing. Some cytogenetic and genetic alterations are associated with higher responses to immunosuppressive remedy. For that purpose, antibacterial, antiviral, and antifungal prophylaxis is routinely utilized in transplant recipients. Importantly, the onset of fever requires immediate clinical evaluation and empirical antibiotic remedy as described in Chapter 265. Inherited Bone Marrow Failure Syndromes Apart from public health measures controlling exposures to benzene, fragrant hydrocarbons, and radiation, little may be accomplished to forestall acquired aplastic anemia. Once the proband is identified, different affected relations, carriers, and siblings with no mutant allele can be identified, and genetic outcomes may be utilized not only in deciding on preemptive (stem cell transplantation) remedy but in household planning as well (for preimplantation genetic prognosis adopted by in vitro fertilization). Because all somatic cells of youngsters and adults with Fanconi anemia are hypersensitive to alkylating agents and oxidative stress, they want to not obtain commonplace doses of radiation or alkylating brokers both for transplant conditioning or for remedy of malignancies. Fortunately, the potential donor pool has expanded now that alternative donor transplants are achievable in Fanconi anemia patients,16 and radiation-free conditioning with reduced levels of alkylating brokers has additionally been successful. In sufferers with acquired aplastic anemia, this complication doubtless evolves by way of a process of clonal choice and adaptation and for that purpose is seen less generally in patients fully responsive to therapy than in these with less than full responses (who subsequently have ongoing suppression of hematopoiesis). This means that more practical methods of immunosuppressive therapy may higher control ongoing marrow injury and reduce the incidence of clonal evolution. Stem cell transplantation with nonmyeloablative approaches has the potential of curing the marrow failure component of those ailments and prolonging life. However, it does nothing to scale back the opposite common life-threatening complication of squamous cell carcinoma. There are good theoretical causes for anticipating that successful transplantation will cut back the chance of clonal evolution to myelodysplasia and acute leukemia. The choice to transplant is influenced by other key elements, as described earlier. Taking these troublesome points into consideration, all sufferers must be evaluated early in an experienced transplantation middle, and members of the family must be screened by hematologists, geneticists, and genetic counselors with use of specialty laboratories. In kids with Fanconi anemia, with proper conditioning regimens, matched sibling donor transplant recipients have expected 5-year survival rates of 90% or more, and with trendy conditioning regimens various donor transplants, in youngsters 10 years of age or younger, are equally successful. In patients with Diamond-Blackfan anemia, sibling donor transplant recipients have 3-year survival rates of about 80%, however the role of matched unrelated donor transplants has not been established. For sufferers with acquired aplastic anemia, small molecules that selectively target the T-cell clones liable for hematopoietic suppression and improve the activity of regulatory T-cells19 could present more effective and fewer poisonous methods for immunosuppressive remedy. For all patients with aplastic anemia, additional enhancements in different donor transplantation have made this modality extra widely out there for sufferers who had not been beforehand thought of to be optimal candidates. For kids with non-severe aplastic anemia, the 10-year progression-free survival price is only about 25%, suggesting that potential trials of early intervention. For patients with inherited bone marrow failure syndromes, the Future Treatments genes for which have been largely identified, the potential of stem cell gene remedy holds huge theoretical promise and has been validated in murine models of the disease and by experiments of nature.
Purchase nitrofurantoin 50 mg fast delivery
Hepatic fibrosis antibiotics for sinus infection cephalexin nitrofurantoin 50 mg discount with mastercard, secondary to dilation of the intrahepatic and extrahepatic bile ducts antibiotics for acne causing depression nitrofurantoin 50 mg buy without prescription, manifests as recurrent ascending cholangitis (Chapter 146) and portal hypertension with splenomegaly and esophageal varices. Aside from an occasional affected sibling, a household historical past is usually not elicited. A6 Bosutinib, an oval dual Src/Bcr-Abl tyrosine kinase inhibitor, can cut back the speed of kidney enlargement however has not been proven to sluggish the decline in glomerular filtration. Fibrocystin/polyductin is predominantly expressed in the cortical and medullary amassing ducts and the thick ascending limbs of Henle. It carries a 30% mortality price owing to extreme pulmonary hypoplasia; oligohydramnios, presumably linked to in utero renal disease, likely accounts for the pulmonary hypoplasia. Hypertension is nearly common, typically develops earlier than renal impairment is clear, and probably accelerates the decline in renal operate. Findings related to renal tubular dysfunction may be current and embody polyuria, enuresis, hyponatremia, and hyperchloremic metabolic acidosis. Treatment of portal hypertension could require liver transplantation or portosystemic shunting (Chapter 145). With enhancing sensitivity of gene-based diagnostics, genetic counseling will play a extra energetic position in prevention. Approximately 50 to 80% of sufferers who survive this era stay previous 15 years of age. Nephronophthisis is characterised pathologically by renal interstitial fibrosis, tubular atrophy with basement membrane thickening and disruption, and renal cysts and diverticula that are largely restricted to the loops of Henle and distal tubules on the corticomedullary junctions. Polyuria occurs early, owing to decreased urinary concentrating ability and to salt losing. A presumptive diagnosis relies on a robust household history and a bland urinary sediment with minimal proteinuria. Medullary sponge kidney, which is a rare dysfunction of unknown pathogenesis, is characterized by congenitally acquired internal medullary and papillary amassing duct dilations, hypercalciuria, and a gentle defect in urinary focus and acidification owing to tubular dysfunction. Patients present with microscopic or gross hematuria and recurrent kidney stones, normally by the second or third decade of life. Medullary sponge kidney can also be an incidental discovering on an intravenous pyelogram that shows the characteristic pooling of distinction material inside the cystic collecting ducts. Calyceal cysts and calyceal clubbing predominate the renal lesion and are best diagnosed by intravenous urography quite than ultrasonography. Oral-facial-digital syndrome is a rare neurodevelopmental ciliopathy characterised by malformations of the mind, face, oral cavity, and digits. Renal (primarily glomerular) cysts are found in as many as 50% of sufferers, all females; males carrying the mutation die in utero. Cysts arise from proximal and distal tubule dilations in small end-stage kidneys no matter cause, mode of dialysis, or presence of a functioning kidney transplant. Acquired cystic kidney illness is often asymptomatic, however it often results in enlarged kidneys with related stomach discomfort and pain. Cyst hemorrhage, which is more widespread than cyst an infection, presents with flank ache, anemia, or hematuria. Mutations in uromodulin impair trafficking of furosemide-sensitive Na-K-2Cl transporter to the apical membrane of the thick ascending limb, thereby causing mild sodium losing and volume contraction, with a secondary enhance in proximal tubule urate reabsorption and hyperuricemia. Anemia, attributable to decreased ranges of angiotensin, precedes the development of persistent kidney disease. Hyperuricemia develops early, likely owing to relative hypotension and increased proximal absorption of uric acid. Accumulation of the abnormal renin leads to tubular cell demise and continual kidney disease. Carcinomas generally current as hematuria and are two to 200 occasions more widespread in patients with acquired cystic kidney disease than within the basic dialysis inhabitants. Any proof of septa formation, solid materials, or distinction enhancement within a cyst is suspicious for carcinoma and warrants consideration of nephrectomy. The incidence of renal cell carcinoma in patients with acquired cystic kidney illness is roughly zero. Tolvaptan and kidney pain in patients with autosomal dominant polycystic kidney disease: secondary evaluation from a randomized managed trial. Treatments to slow development of autosomal dominant polycystic kidney illness: systematic evaluate and meta-analysis of randomized trials. Impact of liver quantity on polycystic liver diseaserelated signs and high quality of life. A kidney-disease gene panel permits a comprehensive genetic analysis of cystic and glomerular inherited kidney diseases. Dietary salt restriction is beneficial to the management of autosomal dominant polycystic kidney illness. Outcome of polycystic kidney disease sufferers on peritoneal dialysis: systematic evaluation of literature and meta-analysis. Is regular screening for intracranial aneurysm needed in sufferers with autosomal dominant polycystic kidney disease Total kidney volume: the most priceless predictor of autosomal dominant polycystic kidney illness progression. Genetics of autosomal recessive polycystic kidney disease and its differential diagnoses. Biopsy proven medullary sponge kidney: scientific findings, histopathology, and role of osteogenesis in stone and plaque formation. Risk components for illness progression in autosomal dominant polycystic kidney illness embody: A. Answer: E Male gender, early onset of hypertension, whole kidney quantity larger than 600 cc/m, and proteinuria are risk elements for the progression of illness. In confirming a prognosis of autosomal dominant polycystic kidney disease in an adult affected person with a optimistic family historical past, which of the following is needed Gene mutational analysis of the affected person and a minimum of two relations (one of whom has the disease) D. All of the above Answer: A A optimistic ultrasonography lead to a patient with a optimistic household historical past of autosomal dominant polycystic kidney disease is sufficient to confirm the prognosis. In the terminal collecting duct, antidiuretic hormone regulates water reabsorption and urinary concentration. Inherited renal tubular disorders are a bunch of conditions in which the conventional renal tubular reabsorption of ions, organic solutes, and water (Chapter 108) is disrupted due to defects in single genes. Disorders of Proximal Tubule Function Cystinuria is characterized by faulty proximal tubular reabsorption of cystine and dibasic amino acids, resulting in increased excretion of cystine and the danger of forming cystine-containing urinary stones (Chapter 117). Although the severity of the illness is similar in all kinds of cystinurias, the scientific presentation could be quite variable, and the onset of disease could occur from infancy to the seventh decade of life. Cystine stones are radiopaque and infrequently form the nidus for secondary calcium oxalate stones. Symptoms embody renal colic, which may be associated with urinary tract obstruction and/or an infection. Affected children can be identified by elevated urinary cystine ranges, however testing must be carried out after tubular transport has totally matured (at age 2 years). Conservative remedy with high urine quantity and urinary alkalinization is sufficient for many sufferers with cystinuria.
Side-Saddle Plant (Pitcher Plant). Nitrofurantoin.
- Digestive disorders, constipation, urinary tract diseases, fluid retention, preventing scar formation, pain, and other conditions.
- Are there safety concerns?
- Dosing considerations for Pitcher Plant.
- How does Pitcher Plant work?
- What is Pitcher Plant?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96145
Buy nitrofurantoin 100 mg with visa
After an outline of the essential physiology regulating red cell manufacturing antimicrobial pens order nitrofurantoin 100 mg without prescription, an strategy to anemia is printed virus wear 100 mg nitrofurantoin cheap with mastercard, based on classification by the reticulocyte response to anemia and further refined by division into normocytic, microcytic, and macrocytic anemia syndromes. In addition, particular anemia syndromes are mentioned including methemoglobinemia, anemia of renal insufficiency, anemia of liver disease, anemia of endocrine deficiencies, physiologic anemia of being pregnant, and unexplained anemia of growing older. The remedy for acute methemoglobinemia is methylene blue 1 to 2 mg/kg, though greater doses as a lot as 6 to 7 mg/kg can be required. The primary regulator of purple cell manufacturing is the effectiveness of oxygen delivery. This crucial want might clarify why hemoglobin concentration or hematocrit are controlled in a relatively slim normal range as compared to the white blood count or platelet rely, the place the higher restrict of regular could additionally be two or 3 times the lower limit of regular. The mediator that interprets peripheral oxygen need to pink cell production is the hormone erythropoietin. After start, the predominant physiologic website of erythropoietin manufacturing is the kidney, although the liver retains some limited capability for erythropoietin production, and neoplasms arising from other tissues and organs could secrete erythropoietin in an unregulated manner. Erythropoietin binds to particular receptors on erythroid progenitors in the marrow leading to increased purple cell production. When correction of anemia normalizes the oxygen pressure within the renal cortex, erythropoietin production falls again to basal ranges. Ambient hypoxia or underoxygenation of the blood by a rightto-left cardiopulmonary shunt additionally results in erythropoietin production. This causes the erythrocytosis seen in dwellers at high altitudes and in people with uncorrected cyanotic heart illness. Red cell production has some feedback regulation of iron availability by way of the erythroferrone/hepcidin/ferroportin axis (Chapter 150). ApproAch to the AnemiAs 1029 failure of the palmar creases to become more prominent when the prolonged fingers are pushed down, extending the palm, usually indicates a hemoglobin no greater than 7 to eight g/dL. Tachycardia and a systolic ejection murmur could develop because of anemia and cardiovascular lodging to it. Peripheral edema could also be occasionally seen with moderately severe anemia: this will replicate a mixture of excessive output heart failure and loss of oncotic pressure associated with fewer blood cells. On uncommon events, retinal hemorrhages may be seen on fundoscopic examination in extreme anemia. All of those vascular and cardiac manifestations of anemia will resolve with correction of anemia. Anemia of fast onset, as may be seen with huge acute hemolysis or with acute blood loss, is extra prone to be symptomatic than anemia from purple cell underproduction or from slow gastrointestinal blood loss. Preservation of blood quantity and cardiovascular accommodation are doubtless the explanations that sufferers, even the aged, with sluggish onset anemias such as B12 deficiency are historically reported to become symptomatic at a lot lower hemoglobin concentrations or hematocrits than patients with iron deficiency anemia from blood loss. A person with coronary artery disease or persistent obstructive lung illness is extra prone to turn out to be symptomatic than an anemic particular person with out these disorders who has the identical hemoglobin focus. Palpitations or a sense of the guts racing or pounding might happen, representing a more rapid heart rate and elevated ejection fraction in order to keep oxygen delivery. Symptomatology in anemia syndromes that develop as a consequence of another disease (such because the anemia of irritation in association with rheumatoid arthritis) will more than likely be dominated by the symptoms of the associated illness. Pica, the need to eat nonnutritive substances similar to ice, is very particular to iron deficiency. Pallor can even occur in other situations associated with shunting of blood away from the periphery to the critical organs. In the evaluation of anemia, pallor of the conjunctival mucosa or the creases within the palm are extra particular than pallor in other sites. Pallor of the conjunctival mucosa generally signifies a hemoglobin focus lower than 9 g/dL; and Hematocrit, purple blood cell depend, and hemoglobin focus require adjustment to frequent items for red cell indices calculations. Certain physical findings may assist guide the analysis of anemia focus by offering clues to particular syndromes, underlying disorders, or bleeding (Table 149-5). Petechiae, purpura, or thrush counsel abnormalities of the platelets or white cells and raise the possibility of a generalized marrow dysfunction not restricted to the erythroid lineage. Frontal bossing (prominence of the brow because of expansion of pink marrow in the skull) is seen in congenital hemolytic anemias but can be a normal variant; in general, adults with hemolytic anemia and this physical discovering have had their diagnosis defined earlier in life. The neurologic findings of B12 deficiency generally require a more thorough examination than is part of the routine physical examination (Chapter 155). Duration of anemia assists in distinguishing congenital from chronic or acute causes. Because iron deficiency is the most typical etiology of anemia in scientific drugs, dietary history (vegetarian or vegan) and a historical past of blood loss ought to all the time be pursued. In women, this must also embrace asking about number of previous pregnancies and whether iron supplementation was used through the pregnancy. Every youngster delivered at time period represents an investment of 800 mg of maternal iron (Chapter 150). A history of cholelithiasis in early maturity is suggestive of congenital hemolytic problems. A historical past of rheumatic or persistent inflammatory disorders raises the potential of the anemia of inflammation (Chapter 150). A historical past of petechiae or straightforward bruising or a historical past of recurrent an infection raises the chance of a hematopoietic dysfunction not limited to the erythroid lineage. A historical past of a specific prognosis, such as sickle cell anemia or thalassemia, is clearly useful. Similarly, a history of family members with episodes of jaundice following minor illnesses suggests a congenital hemolytic the standard complete blood count supplied by automated cell counters contains quite lots of instantly measured and calculated parameters, which at a minimum embrace the white blood cell depend, the red blood cell depend, the hemoglobin concentration and hematocrit, the platelet count, and the red cell indices described beneath. Many automated counters additionally provide a differential white blood rely and a semiquantitative description of red cell abnormalities. Decreased counts of white blood cells and platelets are mentioned in Chapters 158 and 163, respectively. Clinicians should become familiar with the traditional values specific to the laboratories they use. The hematocrit and red cell counts are concentrations as is the hemoglobin concentration, which implies that a change in the plasma quantity can elevate them or decrease them relative to the actual whole body pink cell quantity. An example of an anemia (significant discount within the hemoglobin focus or hematocrit) related to a normal or barely increased pink cell quantity happens within the second trimester of regular being pregnant. In distinction, an elevated hemoglobin concentration or hematocrit with a traditional or decreased pink cell quantity could be seen in dehydration or the capillary leak syndrome Red cells may additionally be described by parameters known as red cell indices, that are routinely calculated by most electronic cell counters. Red blood cell parameter determinations will range between laboratories depending upon tools used and on the inhabitants serving as the basis for the traditional range. For instance, the traditional purple cell values amongst patients residing at high altitude are greater than those in regular topics at sea stage because of decrease ambient oxygen tension driving greater erythropoietin production. Normal values are different between newborns, children, and adults and between women and men after puberty. The distinction in normal hemoglobin concentration, hematocrit, and pink cell depend between grownup men and women is attributed to the motion of testosterone in sensitizing erythroid progenitors to erythropoietin. Reticulocyte Count Red cells newly launched from the bone marrow which have shed their nuclei however still contain some nuclear material within the cytoplasm are called reticulocytes. Reticulocytes have been traditionally measured through supravital staining on recent smears, but now are most frequently measured by circulate cytometry technology included into electronic blood counters. On the routine Wright-Giemsa� stained peripheral blood smear, reticulocytes are slightly larger than purple cells, have little or no central pallor, and have a more grayish (polychromatic) tinge to the cytoplasm.
Nitrofurantoin 100 mg buy online
For the inherited bone marrow failure syndromes (Fanconi anemia antimicrobial use guidelines nitrofurantoin 50 mg generic mastercard, dyskeratosis congenita [telomeropathies] oral antibiotics for mild acne buy generic nitrofurantoin 50 mg on-line, and Diamond-Blackfan anemia) transplantation supplies the only hope for remedy of bone marrow failure however transplantation conditioning regimens and specific post-transplant follow-up research for late effects11 are unique for every specific disease (E-Table 156-3 and E-Table 1564). In truth, for extreme acquired aplastic anemia, immunosuppressive therapy either alone or related to stem cell transplantation is required. Recombinant hematopoietic growth components alone are disappointingly ineffective, except for eltrombopag, a small-molecule agonist of the thrombopoietin receptor (Chapter 163). A large randomized study of eltrombopag together with immunosuppressive remedy is underway (ClinicalTrials. In sufferers with shortened telomeres, artificial androgen remedy with danazol (800 mg daily) can lengthen telomeres and lead to substantial hematologic improvement. Fanconi Anemia Fanconi anemia must be thought of in adults of any age with a family history of aplastic anemia, acute myelogenous leukemia or myelodysplasia, or squamous cell carcinoma at an unusually young age. This illness also needs to be thought of in any patient with any bodily finding listed in Table 156-3 or in sufferers with a family member who has any of those findings. Unfortunately, some sufferers with Fanconi anemia meet none of these criteria, so some hematologists advocate testing for Fanconi anemia in all patients with aplastic anemia younger than 40 years. This disease could be ruled out by acquiring a chromosomal breakage take a look at (see Table 156-3). Here, either lymphocytes or pores and skin fibroblasts are exposed to cross-linking agents. If the clinical context is suggestive (see Table 156-3) but results of the lymphocyte chromosomal breakage test are adverse or equivocal, testing of skin fibroblasts is absolutely required to rule out the prognosis. Once the analysis is made, historical past, bodily examination, blood counts, and chromosomal breakage tests should be carried out on all instant members of the family. Hematopoietic Stem Cell Transplantation: Matched Sibling Donor Dyskeratosis Congenita Dyskeratosis congenita should be considered in any aplastic adult of any age with a member of the family who has had aplastic anemia. It should likewise be considered if both the affected person or a member of the family has had acute myelogenous leukemia, myelodysplasia, nail dystrophy, lacy pores and skin pigmentation, pulmonary fibrosis, oral leukoplakia, squamous cell carcinoma at an unusually younger age, or some other bodily discovering listed in Table 156-3. This disease, a telomeropathy, could be ruled out regularly in patients whose circulating white cells have normal or minimally shortened telomeres as assessed by move cytometric methods. However, in sufferers with extremely quick telomeres (below the first percentile of regular telomere length) or in these with a suggestive household history or physical findings, genetic testing is warranted (see Table 156-3). This is supported by giant retrospective research suggesting that stem cell transplantation is superior to immunosuppressive remedy alone for the therapy of extreme aplastic anemia, especially in patients youthful than forty years. Patients contemplating immunosuppressive remedy with out transplant ought to concentrate on the risks of recurrence and late life-threatening clonal evolution to myelodysplasia or acute leukemia. Unless the donor is a twin, stem cells derived from the bone marrow, not the peripheral blood, ought to be the source of donor stem cells. Knowing the particular gene concerned is essential if preimplantation genetic analysis and in vitro fertilization is planned, an strategy that has successfully resulted in unaffected offspring and ideal twine blood stem cell donors for transplantation of an affected sibling. Transplant linked immunosuppressive therapy begins 2 to 4 days earlier than infusion of stem cells. Posttransplantation immunosuppression regimens are absolutely required and differ from middle to center. Horse versus rabbit antithymocyte globulin in immunosuppressive remedy of treatment-naive aplastic anemia: a systematic review and meta-analysis. A landscape of germ line mutations in a cohort of inherited bone marrow failure sufferers. Current data and priorities for future research in late effects after hematopoietic cell transplantation for inherited bone marrow failure syndromes: consensus assertion from the Second Pediatric Blood and Marrow Transplant Consortium International Conference on Late Effects after Pediatric Hematopoietic Cell Transplantation. Late results screening pointers after hematopoietic cell transplantation for inherited bone marrow failure syndromes: consensus statement from the Second sixteen. In a affected person with pancytopenia, which of the following abnormalities in the peripheral blood smear would supply a useful indicator that the cause for the pancytopenia is aplastic anemia None of the above Answer: E the peripheral blood smear in aplastic anemia is mostly regular, even in severe circumstances. For instance, hypersegmented polymorphonuclear leukocytes (A) counsel megaloblastic anemia (which in more superior levels may cause pancytopenia, not simply anemia). Nucleated (B) and teardrop-shaped (C) red cells suggest a "myelophthisic" course of that includes invasion of the bone marrow by "overseas" parts (like metastatic cancer, fibrosis, or granulomas). The pathogenesis of most circumstances of acquired aplastic anemia can be attributed to: A. Radiation publicity Answer: D Environmental publicity to myelosuppressive chemicals and radiation are now unusual causes of aplastic anemia. The majority of patients with acquired aplastic anemia have an autoimmune illness characterised by oligoclonal T-cell populations that operate to repress stem cell operate. This accounts for the favorable responses to immunosuppressive therapy in such sufferers. A 19-year-old man with extreme aplastic anemia is identified by chromosomal breakage testing to have Fanconi anemia. Bone marrow transplant from a matched associated donor after fludarabinebased conditioning C. Cord blood hematopoietic stem cell transplant after conditioning that features irradiation D. Allogeneic hematopoietic stem cell transplantation in Fanconi anemia: the European Group for Blood and Marrow Transplantation experience. Most of the identified genes inactivated in Fanconi anemia encode proteins that shield the genome from extreme injury induced by chemical cross-linking brokers. Most of the identified genes inactivated in dyskeratosis congenita encode proteins that take part within the upkeep of telomeres. Most of the recognized genes inactivated in Diamond-Blackfan anemia encode ribosomal proteins. The best screening take a look at for Diamond-Blackfan anemia is the chromosomal breakage take a look at. Answer: D Gene mutations for these three syndromes principally involve inactivations of particular genes that encode the key proteins concerned of their molecular pathogenesis, respectively, as correctly indicated in decisions A to C. These mutations in exon 10 (including the rare S505N variant) happen in the juxtamembrane, intracytosolic portion and stabilize the receptor in an energetic dimeric configuration. Although these neoplasms exist alongside a continuous disease spectrum, they every exhibit heterogeneous molecular, biologic, and clinical features that translate into distinctive natural histories. These are all neoplasms arising in a pluripotent hematopoietic stem cell with variations in phenotypic expression being pushed, at least in part, by now well-established somatic mutations. In other instances, therapy is directed at palliation of signs and/or management of the excessive blood counts to forestall thrombotic, vascular, and bleeding problems. No association has been found for skilled, administrative, or clerical occupations.
Purchase nitrofurantoin 100 mg fast delivery
When the direct-reacting fraction is bigger than 15% infection 6 weeks after wisdom tooth removal 50 mg nitrofurantoin generic mastercard, a simple dipstick check for bilirubinuria could make clear the scenario antibiotic resistance animal agriculture purchase nitrofurantoin 50 mg on-line. The canalicular transport mechanism for excretion of bilirubin conjugates is very sensitive to injury. Accordingly, in parenchymal liver illness or mechanical bile duct obstruction, bilirubin conjugates throughout the hepatocyte or biliary tract may reflux into the blood stream, resulting in a blended or, much less typically, a purely conjugated hyperbilirubinemia. Conjugated bilirubin, which is normally loosely sure to albumin, is instantly filtered on the glomerulus; even modest levels of conjugated hyperbilirubinemia result in bilirubinuria, which is always a pathologic finding. Transcutaneous bilirubinometry is an alternate method for measuring bilirubin in infants with neonatal jaundice. The technique is predicated on the measurement of the light mirrored from the percutaneous transmission of visible mild and is conceptually analogous to pulse oximetry. Conjugation of unconjugated bilirubin to bilirubin monoglucuronides and diglucuronides is a important process that greatly increases the aqueous solubility of bilirubin, thereby enhancing its elimination from the body whereas simultaneously decreasing its capability to diffuse across biologic membranes, including the blood-brain barrier. In newborn infants, a decreased capability to conjugate bilirubin leads to unconjugated hyperbilirubinemia (physiologic jaundice of the newborn). If extreme, this hyperbilirubinemia could then result in irreversible central nervous system toxicity. Phototherapy by exposure to gentle within the blue spectrum (390-470 nm) converts bilirubin to water-soluble photoisomers that are readily excreted in bile, thereby defending the central nervous system from bilirubin toxicity. Enterohepatic Circulation and Excretion of Bilirubin Normal human bile contains an average of lower than 5% unconjugated bilirubin, 7% bilirubin monoconjugates, and 90% bilirubin diconjugates. Following canalicular secretion, conjugated bilirubin passes down the gastrointestinal tract with out reabsorption by both the gallbladder or intestinal mucosa. Although some bilirubin reaches the feces, most is converted to urobilinogen and to associated compounds by bacteria inside the ileum and colon, where the urobilinogen is reabsorbed, returns to the liver through the portal circulation, and is re-excreted into bile in a means of enterohepatic recirculation. Hemolysis will increase the load of bilirubin coming into the gut and subsequently the quantity of urobilinogen shaped and reabsorbed. Liver illness decreases hepatic extraction of bilirubin; consequently, plasma urobilinogen ranges rise and extra urobilinogen is excreted in the urine. Severe cholestasis, bile duct obstruction, or antibiotics that scale back or get rid of the bacterial conversion of bilirubin to urobilinogen markedly lower the formation and urinary excretion of urobilinogen. In these circumstances, unconjugated bilirubin is reabsorbed from the intestine, thereby amplifying the hyperbilirubinemia. Increased Bilirubin Production Measurement of Bilirubin in Plasma the total plasma bilirubin focus in regular adults is less than 1 to 1. Modern analytic strategies present that normal plasma contains principally unconjugated bilirubin, with only a trace of conjugated bilirubin. Clinical laboratories usually quantify plasma bilirubin by a reaction by which bilirubin is cleaved by a diazo reagent, such as diazotized sulfanilic acid, to azodipyrroles which may be readily quantitated spectrophotometrically. Unconjugated bilirubin reacts slowly because the positioning of assault by the diazo reagent is protected by inside hydrogen bonding. Accordingly, accurate measurement of the whole plasma bilirubin focus requires addition of an accelerator, such as ethanol or urea, to disrupt this inside hydrogen bonding and to ensure complete reaction of any unconjugated bilirubin. An elevated production of bilirubin and a ensuing unconjugated hyperbilirubinemia could be attributable to hemolysis, an accelerated destruction of transfused erythrocytes, resorption of hematomas, or ineffective erythropoiesis owing to lead poisoning, megaloblastic anemias related to deficiency of either folic acid or vitamin B12, sideroblastic anemia, congenital erythropoietic porphyria, or myeloproliferative or myelodysplastic ailments. In these settings, other liver exams are typically normal and the hyperbilirubinemia is modest, rarely exceeding four mg/dL; larger values indicate concomitant hepatic dysfunction. However, after brisk blood transfusion or resorption of large hematomas caused by trauma, the increased bilirubin load may be transiently enough to lead to frank jaundice. Besides particular blood issues, mild hemolysis accompanies many acquired ailments. In the setting of systemic illness, which may embody a level of hepatic dysfunction, hemolysis may produce a part of conjugated hyperbilirubinemia along with an elevated unconjugated bilirubin focus. Prolonged hemolysis could result in the formation of pigmented gallstones that comprise calcium salts of bilirubin (Chapter 146). Decreased hepatic bilirubin uptake also contributes to the unconjugated hyperbilirubinemia of Gilbert syndrome, although the principal molecular basis for that syndrome is a discount in bilirubin conjugation. The most frequent reason for decreased bilirubin clearance is a lower in bilirubin conjugating exercise. The hereditary hyperbilirubinemias (Table 138-2) are a group of 5 syndromes by which hyperbilirubinemia happens as an isolated biochemical abnormality, with out proof of either hepatocellular necrosis or cholestasis. In CriglerNajjar sort 1, essentially no functional enzyme activity is present, whereas patients with Crigler-Najjar sort 2 have up to 10% of regular and sufferers with Gilbert syndrome have 10 to 33% of regular activity, leading to bilirubin concentrations of 18 to 45, 6 to 25, and 1. Most instances of Crigler-Najjar sorts 1 and a pair of also come up from homozygous or double heterozygous structural mutations throughout the coding region. Jaundice represents the most visible sign of hepatobiliary illness of many causes (Table 138-1). Bilirubin in regular bile: <5% unconjugated bilirubin, with an average of 7% bilirubin monoconjugates and 90% bilirubin diconjugates. Crigler-Najjar kind 1 is characterised by putting unconjugated hyperbilirubinemia that appears in the neonatal interval, persists for life, and is unresponsive to phenobarbital. In Crigler-Najjar Syndrome Type 1 a smaller subset (type 1B), a mutation within the bilirubin-specific exon A1 limits the defect to bilirubin conjugation. Before the availability of phototherapy, most patients with Crigler-Najjar kind 1 died of bilirubin encephalopathy (kernicterus) in infancy or early childhood. Optimal remedy for a neurologically intact affected person contains (1) roughly 12 hours/day of phototherapy from delivery throughout childhood, maybe supplemented by trade transfusion in the neonatal interval; (2) use of tin-protoporphyrin to blunt transient episodes of increased hyperbilirubinemia; and (3) early liver transplantation, earlier than the onset of mind harm. Bilirubin concentrations are usually lower in Crigler-Najjar sort 2, and plasma bilirubin ranges could be decreased to three to 5 mg/dL by phenobarbital. Although a lot much less frequent in CriglerNajjar type 2, kernicterus has occurred in any respect ages, sometimes associated with elements that temporarily raise the plasma bilirubin focus above baseline. For this purpose, phenobarbital remedy is usually recommended; a single bedtime dose normally maintains clinically secure plasma bilirubin concentrations. Gilbert syndrome is the most common form of the hereditary hyperbilirubinemias, with a genotypic prevalence of roughly 12% and a phenotypic prevalence of approximately 7% in whites. Its excessive prevalence may clarify the frequency of gentle unconjugated hyperbilirubinemia in liver transplant recipients and why population-wide studies of bilirubin ranges are inclined to skew toward higher levels. Plasma bilirubin concentrations are most often less than 3 mg/dL, though each greater and lower values are frequent, with will increase of two-fold to three-fold commonly occurring with fasting and intercurrent illness. The phenotypic distinction between delicate Gilbert syndrome and a traditional state is often blurred. Oxidative drug metabolism and the disposition of many, but not all, xenobiotics that are metabolized by glucuronidation seem to be normal in Gilbert syndrome. Peak bilirubin levels are sometimes less than 5 to 10 mg/dL, and ranges return to normal within 2 weeks as mechanisms fostering bilirubin disposition mature. Prematurity, with or with out hemolysis, is associated with higher bilirubin levels which will require phototherapy. [newline]The progestational steroid 3,20pregnanediol and sure fatty acids which are present in breast milk (but not serum) of some mothers inhibit bilirubin conjugation and might trigger extreme neonatal hyperbilirubinemia (breast milk jaundice). Two phenotypically comparable however mechanistically distinct inherited issues, Dubin-Johnson syndrome and Rotor syndrome, are characterised by conjugated or combined hyperbilirubinemia with normal values for different standard liver tests (see Table 138-2). The process of secretion followed by reuptake can also be involved in the disposition of drug metabolites and is believed to prevent the local saturation of upstream hepatocytes with bilirubin and drug conjugates. Another distinguishing attribute is the gray to black pigment that accumulates in cytosolic lysosomal granules in Dubin-Johnson syndrome and offers the liver a attribute black look.
Cheap nitrofurantoin 100 mg without prescription
Acute bacterial prostatitis (type I) is characterised by acute infection of the prostate gland antibiotic induced diarrhea treatment nitrofurantoin 50 mg generic without a prescription. Presenting signs embrace pelvic bacteria horizontal gene transfer cheap 100 mg nitrofurantoin, perineal, penile, or ejaculatory pain in addition to irritative or obstructive voiding symptoms and sexual dysfunction. Patients with extreme infections can current with fever and chills and can turn into septic (Chapter 100). These patients tend to be much less sick during every episode and usually present with voiding symptoms and pain. Leukocytes or inflammatory cells are found in prostate tissue, semen, or expressed prostatic secretions. The prognosis of prostatitis requires a careful history, physical examination, and examination of the urine. The physician should ask pertinent questions on voiding historical past, sexual historical past, signs, pain, neurologic issues, and prior pelvic surgery. The physical examination should embody an stomach, exterior genital, perineal, and digital rectal examination. Urodynamic strategies provide useful insight for sufferers experiencing predominantly voiding signs. Other circumstances, similar to prostatic obstruction, primary bladder neck obstruction, dysfunctional voiding, urethral obstruction, and detrusor-sphincter dyssynergia, may be outlined with the assistance of postvoid residual, pressure-flow urodynamics, or videourodynamics. These conditions, in comparability to prostatitis, have many effective remedy choices. Measurement of a postvoid residual urine quantity by ultrasound can be used to assess incomplete emptying as a end result of urinary retention is often a risk issue for recurrent infections. Low most urine move rates suggest bladder outlet obstruction, decreased detrusor contractility, or both as an alternative explanation for decrease urinary tract symptoms and poor move. Cultures of urethral swabs could additionally be used to evaluate sufferers with probably undiagnosed sexually transmitted diseases (Chapter 269). Other diagnostic exams include semen analysis and culture, that are useful for patients with complaints of abnormal-smelling semen or infertility. Cystoscopy is an adjunct to urodynamics in the analysis of persistent prostatitis/chronic pelvic pain syndrome, especially earlier than any surgical intervention. Cystoscopy is also carried out for analysis of hematuria or irregular cytology findings as a outcome of prostate cancer (Chapter 191) or bladder most cancers (Chapter 187) could cause signs just like persistent pelvic pain syndrome. Anywhere from one third to two thirds of males present process prostate biopsy have continual irritation, however the correlation with symptoms of prostatitis is unclear. The potential utility of pelvic computed xerographic scanning and transrectal magnetic resonance imaging is unclear. Laboratory Evaluation Urinalysis and urine culture should be carried out for every affected person. Historically, the four-specimen take a look at was beneficial, with specimens obtained from the initial voided bladder urine, midstream voided bladder urine, expressed prostatic secretions obtained during prostate massage, and voided bladder urine collected after prostate therapeutic massage. Leukocytes with out bacteria counsel inflammation consistent with nonbacterial prostatitis. In the final week, have you ever experienced any ache or discomfort within the following areas How often have you ever had to urinate once more lower than two hours after you finished urinating, over the last week How often have you ever had ache or discomfort in any of those areas over the last week How much have your symptoms stored you from doing the sorts of stuff you would normally do, over the past week How typically have you ever had a sensation of not emptying your bladder fully after you completed urinating, over the past week Antibiotics with good lipid solubility, good enteric bacterial protection, and a high pKa have the most effective prostatic penetration. These antibiotics embrace quinolones, sulfa-based preparations, macrolides, tetracyclines, and aminoglycosides. A13 In cases in which atypical micro organism, similar to chlamydia, are suspected to be the reason for continual bacterial prostatitis, better outcomes could also be achieved by macrolide antibiotics, such as azithromycin (500 mg twice daily). Most studies show effective remedy with 30 days of remedy, however some clinicians prescribe 6 weeks of therapy as for acute prostatitis as a result of the recurrence fee is as high as 40% inside a 12 months. Current empirical therapy makes use of a mix of -blockers, adrenergic antagonists, phosphodiesterase 5 inhibitors, A15 and anti inflammatory agents. Neuroleptics, corresponding to gabapentin, have been tried however seem to be no better than placebo and have unwanted effects. Conservative supportive therapies embrace warm sitz baths and special diets that keep away from spicy foods, caffeine, alcohol, and other urinary irritants. Therapies that goal to improve rest and to reeducate pelvic floor muscle function can enhance signs in extremely stressed individuals with dysfunctional voiding. Unproven treatments embrace trigger point massage mixed with relaxation and electromagnetic pelvic flooring therapy, acupuncture, and percutaneous tibial nerve stimulation. A16 Prostate massage may be mixed with other therapies, however its efficacy has been variable. Silodosin for the remedy of lower urinary tract symptoms in males with benign prostatic hyperplasia. Efficacy and security of tadalafil 5 mg as soon as every day within the remedy of decrease urinary tract signs associated with benign prostatic hyperplasia in males aged 75 years: integrated analyses of pooled information from multinational, randomized, placebo-controlled clinical studies. Systematic evaluate and meta-analysis on the efficacy and tolerability of mirabegron for the treatment of storage decrease urinary tract symptoms/overactive bladder: comparability with placebo and tolterodine. Combination of alpha-blocker and 5-reductase inhibitor for treatment of benign prostatic hyperplasia. Safety and efficacy of the mixture of once-daily tadalafil and alpha-1 blocker in Japanese men with decrease urinary tract signs suggestive of benign prostatic hyperplasia: a randomized, placebo-controlled, cross-over study. Alpha-blockers with or without phosphodiesterase type 5 inhibitor for treatment of lower urinary tract signs secondary to benign prostatic hyperplasia: a scientific review and meta-analysis. Three-year outcomes of the possible, randomized managed rezum system examine: convective radiofrequency thermal therapy for therapy of lower urinary tract signs as a result of benign prostatic hyperplasia. Long-term effects of doxazosin, finasteride and combination therapy on high quality of life in males with benign prostatic hyperplasia. Efficacy of newer drugs for decrease urinary tract symptoms attributed to benign prostatic hyperplasia: a scientific evaluate. Network meta-analysis of the efficacy of acupuncture, alpha-blockers and antibiotics on chronic prostatitis/chronic pelvic pain syndrome. Current evidence for the involvement of intercourse steroid receptors and sex hormones in benign prostatic hyperplasia. Lower urinary tract symptoms, benign prostatic hyperplasia, and urinary retention. Prostate dimension, nocturia and the digital rectal examination: a cohort study of 30 500 males. Aquablation versus transurethral resection of the prostate: 1 year United States-cohort outcomes.