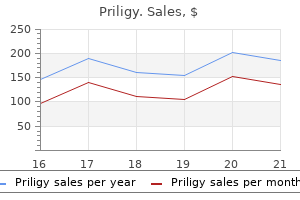
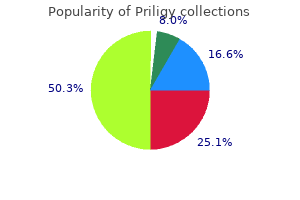
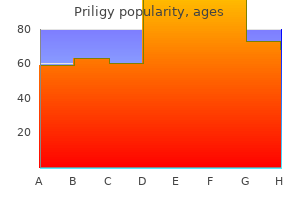
Priligy
Priligy dosages: 90 mg, 60 mg, 30 mg
Priligy packs: 10 pills, 30 pills, 60 pills, 90 pills, 120 pills, 20 pills

Priligy 60mg order on-line
Clinical pearl: eradicating as much of the frontal beak as attainable and creating a large superior septectomy will concurrently maximize the frontal sinusotomy erectile dysfunction pump uk 60 mg priligy purchase fast delivery. Covering the denuded bone with mucosal flaps or free mucosal grafts can assist in post-operative healing and decrease stenosis causes for erectile dysfunction and its symptoms priligy 30mg purchase amex. Clinical pearl: atomized 4% lidocaine or topical 4% cocaine will adequately anesthetize the sinonasal cavity sufficient for sufficient debridement. Clarification of terminology in patients with eosinophilic and noneosinophilic hyperplastic rhinosinusitis. Evaluating the analysis of chronic rhinosinusitis based mostly on medical tips and endoscopy. Radiologic correlates of symptom-based diagnostic criteria for persistent rhinosinusitis. Usefulness of affected person symptoms and nasal endoscopy in the analysis of chronic sinusitis. Impact of useful endoscopic sinus surgery on symptoms and quality of life in chronic rhinosinusitis. A double-blind, randomized, placebo-controlled trial of macrolide in the therapy of continual rhinosinusitis. Atypical sinusitis in adults must result in on the lookout for cystic fibrosis and primary ciliary dyskinesia. Medical therapy vs surgical procedure for persistent rhinosinusitis: a prospective, multi-institutional research. Smoking and endoscopic sinus surgical procedure: does smoking volume contribute to medical outcome. The security and efficacy of intravenous ketorolac in patients present process primary endoscopic sinus surgery: a randomized, 27. Complications in endoscopic sinus surgical procedure for continual rhinosinusitis: a 25-year experience. The impact of the total intravenous anesthesia compared with inhalational anesthesia on the surgical field throughout endoscopic sinus surgery. Intravenous anesthesia supplies optimum surgical conditions throughout microscopic and endoscopic sinus surgical procedure. Propofol for upkeep of common anesthesia: a way to limit blood loss throughout endoscopic sinus surgical procedure. Bacteriologic findings from the nostril, ethmoid, and bloodstream during endoscopic surgery for persistent rhinosinusitis: implications for antibiotic remedy. Prophylactic perioperative antibiotic use in endoscopic sinus surgery: a systematic evaluate and meta-analysis. Preoperative corticosteroid oral remedy and intraoperative bleeding throughout functional endoscopic sinus surgery in sufferers with severe nasal polyposis: a preliminary investigation. Role of dexamethasone in decreasing pain after endoscopic sinus surgical procedure in adults: a double-blind prospective randomized trial. Perioperative single dose systemic dexamethasone for postoperative pain: a meta-analysis of randomized controlled trials. Corticosteroid remedy throughout endoscopic sinus surgical procedure in children: is there a need for a second look Comparing the reverse trendelenburg and horizontal place for endoscopic sinus surgery: a randomized managed trial. Multiple analyses of factors associated to intraoperative blood loss and the role of reverse Trendelenburg place in endoscopic sinus surgical procedure. The use of image-guided surgery in endoscopic sinus surgery: an evidence-based evaluate with recommendations. The missed ostium sequence and the surgical strategy to revision practical endoscopic sinus surgical procedure. The impact of maxillary sinus antrostomy size on xenon air flow in the sheep mannequin. Small and huge center meatus antrostomies in the remedy of chronic maxillary sinusitis. Recirculation of mucus through accessory ostia inflicting chronic maxillary sinus disease. Modified endoscopic medial maxillectomy for recalcitrant chronic maxillary sinusitis. Use of the superior meatus and superior turbinate in the endoscopic method to the sphenoid sinus. On the sensible worth of differences in the level of the lamina cribrosa of the ethmoid. Modified transnasal endoscopic Lothrop procedure as an various alternative to frontal sinus obliteration. A randomized control trial of post-operative care following endoscopic sinus surgery: debridement versus no debridement. Relationship between the frequency of postoperative debridement and affected person discomfort, therapeutic interval, surgical outcomes, and compliance after endoscopic sinus surgery. Early postoperative care following endoscopic sinus surgery: an evidence-based review with suggestions. Emotional effects of nasal packing measured by the hospital anxiety and melancholy scale in patients following nasal surgery. The causes for surgical failure can be complicated and multifactorial, and generally additional surgery may be considered. Due to alteration or distortion of the traditional anatomy attributable to previous surgical procedure or longstanding illness, revision sinus surgical procedure may be technically difficult. Other components, together with persistent inflammation, resistant infection, and increased bleeding, add to degree of difficulty, which is usually further sophisticated by the need for major or revision surgical procedure of an anatomically complex frontal recess. These patients are, subsequently, anticipated to obtain long-lasting relief from an endoscopic sinus process. The surgical aim in these sufferers, due to this fact, is subjective high quality of life improvement, decreased mechanical obstruction exacerbating irritation, and improved entry to the sinus cavities. In these patients, the source of the issue has been variably attributed to components corresponding to faulty host immunity, IgE-mediated reaction to fungus, biofilms, osteitis, and superantigens, amongst others. The reasons for surgical failure can be broadly categorised into persistent mechanical obstruction, mucosal illness, or a mixture of each. Mechanical obstruction can occur postoperatively from unsuccessfully addressed initial disease or iatrogenically created obstruction. A cautious history should be taken to examine pre- and post-operativecomplaints, and in addition to decide the good thing about the initial surgical or current medical interventions. How often have they been treated with medical therapy, including extended programs of antibiotics and systemic corticosteroids The goal of the history is framing the current symptoms in gentle of a complex and extended sinus history.
Priligy 60 mg buy amex
The complete release of this muscle from all of its aberrant attachments adopted by its reconstitution right into a practical ring symbolize the most important steps in attaining good outcomes erectile dysfunction melanoma buy priligy 90 mg low price. Inadequate launch will end in tethering of the ipsilateral flaps and distortion of the ultimate outcome tobacco causes erectile dysfunction purchase 90 mg priligy free shipping. No matter how nicely the pores and skin flaps are designed the final word success depends on this layer. On the non-cleft side the muscle should be released from the attachments to the premaxilla and the caudal septum. A well-defined free edge of muscle has to be created on this side to enable suturing to contralateral edge of the orbicularis. The aberrant fibers of the muscle will attach alongside the anterior face of the maxilla, the nasal piriform aperture, in addition to the alveolar ridge. The creator often begins with launch of the fibers to the nasal-alveolar advanced after which observe with horizontal launch alongside the anterior face of the maxilla. Once the muscle is completely mobilized, the cleft lip skin and soft tissue should easily advance to the midline. Before the muscle closure begins, at this point, the next step is to full the first rhinoplasty. This entails the release of the pores and skin and delicate tissue envelope overlying the alar cartilages on both the cleft aspect in addition to the medial portion of the non-cleft aspect. To obtain a extra rounded and pure configuration, the pores and skin should slide over the cartilage because the ala is repositioned. Medially, from the incision on the columellar base, a dissection is done in-between the medial crura along both anterior domes. The ala is also approached from the lateral incision to allow for full mobilization. An alar suspension suture of 4-0 vicryl is then positioned from the alar base to the septal premaxilla. Two quilting chromic stitches are then placed to fixate the pores and skin and nasal mucosa to the alar cartilage in the new alignment of those tissue planes. The closure of the mucosal flaps, repair of the nasal flooring, and intraoral closure is carried out at this point. If the muscle layer has been launched appropriately, this may be carried out with minimal tension. From the inferior section at the vermilion the closure is extended with interrupted sutures up in path of the nasal sill. Four to 5 interrupted sutures are positioned to allow for a reliable broad vertical closure. The triangular "c" flap can be positioned laterally into the nasal sill or alternatively in certain cases recruited medially to help reconstruct the columellar base. Minor incorporations of the lower lip scar lengthening procedures similar to a small Z plasty above the vermilion or a white roll flap can help optimize the result. These typically have the best aesthetic outcomes as the nasal deformity is minimal in these sufferers. Note that whereas the configuration of the nostril is relatively symmetric the alar base place on the cleft aspect remains posteriorly displaced. The triangle flap repairs popularized by Tennison and subsequently modified by Randall are primarily based on scar lengthening utilizing donor tissue within the decrease region of the higher lip immediately above the vermillion. As noted within the dialogue above, the scar complexity of this strategy is less favorable with the final placement of a horizontally oriented scar throughout the mid philtrum. In the lengthy run that is extra essential than scar complexity within the eyes of the observer looking at a lip. Ideally if sufficient rotation and philtral stability is obtainable in the Millard strategy, this can provide one of the best outcome, but if the vermillion remains elevated at the highpoint of the cleft facet after a Millard type repair, the triangle flap procedures may be the finest choice. The measurements are comparatively straightforward and precise and the result is reliable. This has led to its acceptance and widespread use as a viable different to the Millard method. As with the Millard technique, the primary three anatomical landmarks (1, 2, 3) marked are the respective high and low factors of the cupid bow starting on the noncleft facet. Next, factors four and 5 are recognized as the lateral base of the columella on each side. Once these marks are positioned, measurements are made to determine the dimensions and extent of development needed within the triangle flap. The midline point of the prolabium is marked at the transition from skin to vermillion (1). The width must be saved slender (4 mm to 5 mm) as the philtrum widens in the postoperative period. These embrace the columellar base (4, 5), the nasal sill transition (8, 9), the alar base (10, 11) and at last the oral commissures (12, 13). The primary design incorporates the formation of two fork flaps from the lateral prolabium skin in addition to the columellar/philtral flap for the reconstruction of the philtrum within the midline. The dissection and surgical strategy of each side of the cleft are much like these utilized on the cleft side of a unilateral lip repair. Endonasal incisions are made bilaterally to allow for a major rhinoplasty to be performed. The columellar/philtral flap and the bilateral fork flaps are elevated in the airplane overlying the prolabium periosteum. Often there are fibrous bands current on this layer that can appear like orbicularis muscle fibers. This layer must be reconstituted completely with the true muscle fibers that have to be advanced across midline from each of the lateral segments. After the skin flaps are elevated from the prolabium section, the mucosal flap is then elevated off posteriorly. This further length when added to limb (3-4) should equal limb (1-5) to get a balanced result. This is done by drawing a line of size x from level three to the midline point proven by the blue dot on the philtrum. The medial blue point of the cleft aspect flap advances into the mid-philtral blue level. Depending on the place of the premaxillary segment (if midline), symmetry is usually not troublesome to obtain because the anatomic abnormalities are analogous bilaterally. The relative ease of establishing symmetry belies the challenges of these defects that restrict the final consequence in some ways. Superior limbs of the column are sometimes vertically oriented and end within the nasal sill as an alternative of at the columellar base after the first repair. These inherent limitations of the primary repair mean that bilateral cleft lip restore patients will often need a staged intermediate process of their early childhood to secondarily enhance the result. A commonly utilized procedure for this function is bilateral fork flap primarily based on the widened philtral section which is used to obtain columellar development and lengthening.
Syndromes
- Watery nasal drainage (rhinorrhea)
- Short stature
- Problems with testosterone formation: Testosterone is formed through a series of steps, where each requires a different enzyme. Deficiencies in any of these enzymes can result in inadequate testosterone and produce a different syndrome of 46, XY intersex. Different types of congenital adrenal hyperplasia can fall in this category.
- Tremor
- Diverticula
- Bleeding
- Tumor in or around the shoulder
- Hypofibrinogenemia (decreased fibrinogen levels)
Buy priligy 90mg cheap
Despite these many advantages best male erectile dysfunction pills over the counter priligy 90mg buy cheap on line, the restricted surgical publicity typical of endonasal rhinoplasty prevents the application of many superior operative strategies erectile dysfunction pump on nhs priligy 30 mg discount on-line, making closed rhinoplasty poorly suited to advanced revision procedures. Nevertheless, endonasal rhinoplasty stays the popular method for quite a few beauty surgeons, notably in the beforehand un-operated nostril (primary rhinoplasty) or for restricted revision ("touch-up") procedures. Use of the rim incision is discouraged owing to its characteristically conspicuous and unsightly appearance and the increased risk of nostril stenosis. Usually less than 5 to 7mm long, the trans-columellar incision is often positioned on the mid-columella and is commonly irregularized to enhance camouflage and reduce scar contracture. While this incision leads to a probably seen scar, it additionally permits widefield surgical de-gloving of the nasal framework for dramatically improved entry to the nasal skeleton. Moreover, when repaired correctly, the trans-columellar scar is frequently indiscernible. Thus, contamination from the underlying nasal cavity is minimized, and structural help to the nasal sidewall is preserved. The open strategy also facilitates en bloc elevation of the pores and skin soft tissue envelope, thereby limiting disruption of the cutaneous capillary and lymphatic networks. Although endonasal rhinoplasty remains to be in widespread use, the external method has turn into the procedure of alternative for advanced structural reconstruction of the collapsed-nasal framework. Owing to its greater diagnostic accuracy and therapeutic versatility, external rhinoplasty will no doubt stay the workhorse of revision-nasal surgical procedure. Fundamentals of Tip Rhinoplasty Regardless of the surgical strategy chosen, the target of cosmetic rhinoplasty is the controlled and creative reconfiguration of the nasal framework. Because lots of the early refinement techniques relied solely upon alar cartilage excision to partially collapse the alar tripod, cosmetic results have been often unpredictable and regularly disappointing. Even satisfactory beauty results had been too typically vulnerable to delayed shrink-wrap deformities and eventual nasal sidewall collapse. Despite the massive number of tip refinement techniques described to date, few methods have withstood the check of time, and many have been deserted or condemned as a outcome of consistently poor surgical results. While considerable disagreement exists among accomplished surgeons regarding the optimum method of tip enhancement, all successful tip-plasty strategies share a quantity of widespread characteristics. Perhaps the most important common component in a profitable tipplasty is enough preservation of structural tip support. Without effective assist of the nasal tip, the lobule eventually succumbs to the persistent forces of muscle motion, gravity, or growing older; and an elongated, counter-rotated, and/ or under-projected nostril ensues. Indeed, poortip help is incessantly a causative issue, not solely within the failed rhinoplasty, but also within the naturally unattractive nose as properly. Another important characteristic of successfultip modification is an aesthetically pleasing separation of the nasal domes. Whether from congenital malformation or failed surgical intervention, tightly approximated nasal domes produce an objectionable "pinched" or "uni-tip" look. Moreover, noses with this appearance are frequently suffering from functional collapse of the nasal airway, making the mixed aesthetic and useful deficits a standard motive for looking for corrective surgical procedure. Like the overly narrow nasal tip, excessive domal width can be highly disruptive to beauty harmony, and each a wide balllike lobule or a bulbous tip are highly undesirable and conspicuous options that always immediate beauty rhinoplasty. Hence, all efficient tip discount methods should exactly narrow tip width without invoking useful encroachment of the nasal airway. Since divergence of the medial crura and separation of the nasal domes are mandatory attributes of any engaging nasal tip, all effective tip modification methods must additionally preserve these critically important aesthetic options. Finally, the last element frequent to all efficient tip-plasty methods is versatility. Because virtually no two noses are alike, surgical alteration of the nasal tip should have the power to accommodate individual variations in tip morphology including projection, rotation, symmetry, and width. Furthermore, because maneuvers which enhance nasal contour from one perspective, might disrupt nasal aesthetics from one other, all effective tip-plasty techniques must be succesful of compensate for undesirable secondary or tertiary effects of cartilage reshaping. The end result should be a steady, pure, and enticing tip contour when viewed from all angles. Although it has been acknowledged that mastery of the tip equates to the mastery of rhinoplasty, this represents a gross oversimplification of the numerous challenges and complexities of beauty rhinoplasty. Nevertheless, no rhinoplasty may be considered really successful if an attractive tip is lacking, and reaching a cosmetically pleasing tip contour can present one of many more daunting facets of cosmetic-nasal surgical procedure. Refining the overly extensive tip includes narrowing broad-domal arches, reducing extreme interdomal space, and restoring domal symmetry. However, earlier than the naturally engaging nasal tip may be replicated, the surgeon should first understand the skeletal configuration which characterizes the naturally enticing nostril. The ensuing divergent configuration creates a diamond formed surface contour which surrounds a small interdomal cleft. Ordinarily the cleft is crammed with supportive ligaments and other fibromuscular tissues, leading to a smooth, barely convex, exterior contour. When domal spacing is right, this configuration results in a slender and chic lobule with distinct, individualdomal highlights. In addition to optimum domal spacing, the best tip configuration can also be characterized by flat, straight, and symmetric lateral crura. Although modest convexity may be tolerable within the wide nose, a flat, uniplanar lateral crus typically supplies the most appealing nasal form. While just about no two noses are exactly alike, variations of this alar cartilage configuration are found in virtually all naturally engaging noses. Although the angle of divergence will vary in accordance with the specified tip width, the presence of a diamond-shaped lobule and smooth, flat lateral crura are essential to a beautiful tip contour, and all tip-plasty techniques either mimic or recreate these essential skeletal features. In the affected person with thickskin, the massive inter-domal house is typically filled with fibromuscular tissue, but lobular bifidity may also be noticed in the absence of thick nasal pores and skin. From under, the broad nasal tip seems trapezoidal in form quite than the popular equilateral triangle, and the lateral crura are generally flat or gently convex presenting a conspicuous-bulbous appearance. Refining the boxy tip entails making a extra angular domal arch to narrow the extreme interdomal area. Typically the lateral crura require little modification apart from modest cephalic resection on the "paradomal" region to eliminate supratip fullness within the nasal profile. Refinement of the bulbous tip deformity entails narrowing the overly broad tip (as described above for the broad-tip deformity) adopted by flattening of the convex lateral crura. Eliminating convexity in the cupped and bowed lateral crus with out compromising nasal sidewall support could be extremely difficult and will require a combination of cartilage excision, suture modification, and/or cartilage-grafting strategies. Note the wide interdomal spacing, linear alar sidewall, and trapezoidal tip configuration on base view. Modest-domal asymmetries are often evident in the misshapen lobule, and the deformities described above are commonly observed in combination. Because extreme tip width is a typical function of the misshapen nose, a variety of methods have been described to tackle the extensive lobule. Perhaps the simplest approach for tip refinement is suture modification of the alar tripod. Suture-based refinement strategies rely upon cartilage reshaping, somewhat than the standard strategy of cartilage excision, to reconfigure the outsized lobule. These strategies permit narrowing of the domal arch, discount of the interdomal space, or combinations therein, whereas concurrently conserving structural support and minimizing the chance of contracture-mediated deformities. To create the desired V-shaped domal configuration, scoring of the domal apex is often necessary to break the "spring" of the alar arch.
Cheap priligy 90mg without a prescription
Racemic epinephrine is a mixture of the epinephrine rotatory isomers dextro (d) erectile dysfunction hypnosis 60 mg priligy discount overnight delivery, and levo (l) erectile dysfunction injections side effects priligy 60 mg order fast delivery. They act to cut back airway edema by their alpha-adrenergic effect on mucosal vasculature and are given as zero. Although each isomers have this alpha-adrenergic effect on the mucosa, the d-isomer is stronger and might thus lead to extra systemic unwanted aspect effects than the l-isomer, which is why a combination of the two is used. The most concerning are the cardiovascular unwanted side effects of high blood pressure and cardiac arrhythmias. Children should be monitored closely for at least three hours, though some still advocate hospital admission after the use of racemic epinephrine. The decreased edema seen with corticosteroids as nicely as the studies that have shown their efficacy are arguments for his or her use. However the lack of complete understanding of their mechanism of action and their potential systemic unwanted effects, as well as the danger of bacterial and fungal superinfections argues towards their use. The helium decreases the density of the gasoline mixture and increases the viscosity, thus increasing the laminar circulate. Patients ought to stay intubated until an air leak develops around the endotracheal tube, which is usually inside 5 to seven days. If the histology is in maintaining with a herpes virus infection, antiviral medicines, similar to acyclovir, ought to be used to deal with the patient. The most frequent cause of fungal laryngitis is Candida species, nevertheless many different fungi may be the trigger, together with Blastomyces, Histoplasma, Cryptococcus, and Coccidiodes (Table 42-7). This is due to the similar gross look of epithelial dysplasia of the larynx and fungal an infection. Fungal infection will show fungal spores, hyphae, and pseudohyphae inside the upper layers of the epithelium. Hematoxylin and eosin stains will reveal what is named pseudoepitheliomatosis hyperplasia. This term specifically refers to epithelial hyperplasia with hyperkeratosis, neutrophils within the higher epithelial layers and lymphocytes, plasma cells, and scarring within the submucosal stroma. Fungal infection may also predispose to dysplasia, therefore each components may be current. Fungal colonization differs in that the fungal components lie on prime of the epithelial layer, with no penetration, and no related hyperkeratosis or neutrophil infiltration. An oral conazole for three to four weeks may be used if the topical is unsuccessful. If the fungal laryngitis continues to fail to reply, especially when dysplasia is current, a fungal infection secondary to neoplasia should be considered. Although micro organism are mostly regarded as being free-floating, these planktonic creatures symbolize the minority of micro organism on the planet. A bacterial biofilm has been defined as a microbially derived sessile community characterized by cells that are irreversibly hooked up to a floor. The bacteria then start secreting a glycoprotein matrix consisting of water, polysaccharides, proteins, and nucleic acids. This matrix provides each protection to the cells as properly as a dynamic construction to facilitate development and survival. Bacteria are located within the totally different layers, these extra superficial are extra metabolically active and may separate from the community to type doubtlessly infectious, planktonic bacteria. Most antibiotics require metabolically lively micro organism or exposed ligands to exert their anti-microbial results whereas detergents are unable to penetrate deeply enough to kill these persister cells. These circumstances enable the biofilms to tolerate minimal inhibitory concentrations of antibiotics which may be 10 to a thousand occasions greater than that wanted to kill planktonic micro organism. The bacteria in the biofilm talk through a complex process referred to as "quorum sensing". This occurs when the biofilm reaches a critical measurement, constituting a quorum, then communicate with one another to control the manufacturing of the glycoprotein matrix, division charges, and gene regulation within the bacterial community. The decreased metabolic exercise of the micro organism can make culturing the offending brokers harder as well. Biofilms have been shown to play roles in otitis media and chronic sinusitis, whereas being present on tympanostomy tubes, adenoid tissue, tonsils, tooth and tracheotomy and endotracheal tubes. Thus other techniques have been used to establish biofilms including electron microscopy. The issue with every modality consists of the issue in fixation, artifacts from the fixation course of and the issue identifying particular kinds of bacteria. Fluorescent in situ hybrization with confocal laser scanning microscopy has also been used to get hold of a three-dimensional image of the biofilm and determine the bacteria. These eradication strategies might include mechanisms that bodily disrupt the biofilm. Topical antibiotics such as mupirocin have been proven to kill bacteria associated with biofilms and reduce general biofilm mass. Photodynamic remedy may be of benefit in that it has been proven to lower bacterial viability, and sure antibiotics, corresponding to macrolides, have been shown to disrupt quorum sensing. Mucosal biofilm formation on middle-ear mucosa in the chinchilla model of otitis media. Microbiology of middle ear effusions from 292 sufferers undergoing tympanostomy tube placement for middle ear disease. Current face of acute otitis media: microbiology and prevalence resulting from widespread use of heptavalent pneumococcal conjugate vaccine. Changing paradigms in parasitic infections: frequent dermatological helminthic infections and cutaneous myiasis. Tularemia presenting as tonsillopharyngitis and cervical lymphadenitis: a case report and evaluation of the literature. Antimeasles immunoglobulin G for serologic analysis of otosclerotic hearing loss. Auditory brainstem response and otoacoustic emission evaluation of hearing-impaired children of mothers who contracted rubella during being pregnant. Blastomycosis presenting as a locally invasive intranasal mass: case report and literature review. An update on inflammatory disorders of the pediatric airway: epiglottitis, croup, and tracheitis. Use of heliox to avoid intubation in a toddler with acute extreme asthma and hypercapnia. Do biofilms contribute to the initiation and recalcitrance of continual rhinosinusitis Clinical application of treating biofilm-associated infections in household medicine. It is characterized by one or more nasal signs of pruritus, sneeze, discharge, and stuffiness. The prevalence is rising dramatically notably in nations with low prevalence. The prevalence of physician-diagnosed allergic rhinitis is 14% in United States adults, 7% in Latin American adults, and 9% in Asian-Pacific adults. The prevalence of seasonal allergic rhinitis in United States adults with physician diagnosed allergic rhinitis is about 43%, and the prevalence of perennial allergic rhinitis is about 56%.
90 mg priligy discount overnight delivery
Contemporary Structural Rhinoplasty: A SaferAlternative to Excisional Methods Structural rhinoplasty strategies now offer an alternative selection to jacksonville impotence treatment center priligy 30 mg buy low cost the standard excisional strategies which are nonetheless in widespread use today sudden erectile dysfunction causes priligy 60 mg discount on line. In addition to beauty and useful outcomes that rival some other technique of beauty nasal surgery, wellexecuted structural rhinoplasty techniques additionally supply matchless long-term contour stability. In the wholesome and attractive (but previously unoperated) nostril, secure central tip help is derived from the collective contributions of medial crural rigidity, soft-tissue interconnections, and septal undergirding. Ironically, just about all rhinoplasty methods inadvertently compromise these structural assist mechanisms to a larger or lesser diploma, potentially exacerbating the unpleasant nasal contour. In truth, structural rhinoplasty is largely carried out via the external rhinoplasty strategy which severely disrupts the ligamentous and soft-tissue interconnections that naturally strengthen and consolidate the nasal-tip framework. Consequently, compensatory remedy measures are necessary as a half of any exterior rhinoplasty to restore or exceed earlier tip support. And since any nostril missing enough tip support will also suffer from a number of cosmetic and useful deficits, any alternative surgical paradigm that ultimately fails to establish secure and durable central tip support will eventually lead to surgical failure. Foremost among the many precepts of structural rhinoplasty is augmentation of the medial crura with autologous cartilage to ensure dependable long-term tip help. Whether using a columellar strut, a septal extension graft, or a tongue-in-groove imbrication upon the caudal septum, augmentation of medial crural rigidity and/or medial crural length is prime to structural rhinoplasty ideas and is a basic objective in any affected person undergoing exterior rhinoplasty. Rigid and safe tip support not solely affords enhanced precision in tip positioning for both cosmetic and functional optimization, nevertheless it can additionally be achieved with out jeopardizing baseline structural support or long-term stability. In reality, when used in conjunction with tissue-sparing methods similar to suture-based contouring and skeletal repositioning, structural rhinoplasty techniques produce not solely a extra enticing nasal contour, but also a far stronger and more durable skeletal framework. To maximize rigidity and stability of the central assist column, a septal extension graft is suture fixated to the caudal septum and/ or nasal backbone. Fashioned from septal, conchal, or rib cartilage, the septal extension graft is physically buttressed and undergirded by the present skeletal framework to present the maximum stage of structural help. However, the structural and aesthetic benefits of the septal extension graft also apply to primary rhinoplasty. Individuals with naturally weak, under-projected nasal cartilages and thick nasal skin are particularly well-suited to this remedy paradigm since inflexible tip support can be required to project the frail tip cartilages in opposition to thick unyielding pores and skin. In truth, the longterm structural stability supplied by the septal extension graft is applicable to nearly any nose, including noses requiring deprojection. Suture suspension of the lateral crura can address a giant number of problems in the misshapen nostril whether or not derived from congenital, traumatic, or iatrogenic causes. In the over-resected nostril and under-projected tip, suspending the lax and concave lateral crura eliminates pinching, minimizes or eliminates alar retraction, and concurrently improves crural help and airway patency � in effect reversing the sequelae of crural over-resection. Using adjunctive methods such because the lateral crural steal, vertical dome division, and the tongue-in-groove setback; a stretched, flat, and taut lateral crus may be achieved by way of suture suspension to re-contour, strengthen, and/or functionally improve virtually any nasal morphology. Moreover, as a outcome of the dependability of central tip assist is directly proportional to the biomechanical energy of the augmentation graft material, long-term results will vary according to the suitability and abundance of available donor supplies and based on the quality of healing responses. However, as with any innovation, misuse and overuse can lead to undesirable consequences. In the case of structural augmentation grafts, overzealous software can lead to excessive nasal bulk, symptomatic airway impingement, annoying nasal rigidity, donor-site morbidity, and unsightly beauty deformities that are sometimes more objectionable than the beginning nasal contour. Ironically, over-grafting is turning into an more and more frequent explanation for technical rhinoplasty failure. Although successful implementation of structural rhinoplasty strategies nonetheless requires all of the attributes of surgical excellence, including a discerning cosmetic analysis, sound aesthetic judgment, good technical skills, and atraumatic surgical approach, the applicability and treatment potential of this surgical paradigm is presently unparalleled. And when taken to its full potential, structural rhinoplasty mimics the skeletal dynamics of the naturally healthy and enticing human nostril, all while growing long-term sturdiness of the skeletal framework. As a consequence, structural rhinoplasty is quickly changing into the gold normal for engaging and predictable long-term rhinoplasty outcomes and will probably outline the method ahead for beauty nasal surgery for many a long time to come. While the dedication required to achieve mastery in rhinoplasty is formidable, transformation of the human nostril from a misshapen appendage to a beautiful facial attribute is a uniquely gratifying experience. For the newbie, mastery of nasal evaluation and relentless self-assessment will pave the best way for a protracted and rewarding career in nasal surgical procedure. Acoustic rhinometry, rhinomanometry, and the sensation of nasal patency: a correlative research. Investigating the nasal cycle using endoscopy, rhinoresistometry, and acoustic rhinometry. Neural drive to nasal dilator muscles: Influence of train intensity and oronasal move partitioning. Patient of the Month Program Monograph Series, American Academy of Otolaryngology�Head and Neck Surgery Foundation. Use of Desmopressin for unremitting epistaxis following septorhinoplasty and turbinectomy. Perioperative antibiotic prophylaxis in cosmetic surgery: a prospective examine or 1,100 adult patients. Overresection of the lower lateral cartilages: a typical conceptual mistake with useful and aesthetic penalties. Lateral Crural Tensioning for Refinement of the Wide and Underprojected Nasal Tip: Rethinking the Lateral Crural Steal. Determining the precise trigger and site of the obstruction is paramount to successfully intervention. Obstruction is attributed to the nasal valve in as many as 13% of patients, but its anatomic and dynamic contributions often are missed. Functional rhinoplasty encompasses a quantity of surgical methods used to handle lateral wall abnormalities and nasal valve dysfunction. Poiseulle legislation describes how airflow via the nostril is proportional to the radius of the nasal passage to the fourth energy. Therefore, small adjustments in the cross-sectional space of the nasal valve may have exponential effects on the move volume, hence small deceases in the cross-sectional area considerably lowering nasal airflow. It is also important to understand the effect of Bernoulli precept on collapse of the nasal valve. During normal inspiration, negative strain is transmitted from the nasopharynx to the valve area, which is ready to then narrow as a end result of the pressure from this unfavorable pressure. With higher forces (> 30 L/min) the conventional internal nasal valve begins to collapse, prohibiting nasal influx and serving as a physiologic Starling resistor. The exterior nasal valve is outlined because the area inside the nasal vestibule, corresponding to the alar lobule and its surrounding fibroaleolar tissue. It is bounded by the caudal portion of the septum, columella, alar rim, and nasal sil. The alar lobule is mobile and less inflexible from lack of cartilaginous support, and due to this fact, dynamic collapse of exterior valve can sometimes be seen during forceful inspiration. Black circle = External valve; Green arrow = Intervalve area;Red arrow = Lateral extent of lateral crura of decrease lateral cartilage, on this affected person with recurvature; Yellow triangle = Internal nasal valve angle.
Generic 30 mg priligy otc
Traditionally impotence while trying to conceive cheap 30 mg priligy otc, rejuvenation of the growing older face has mostly centered on the lower face occasional erectile dysfunction causes 30mg priligy with mastercard. Often the eyebrows and the mid-face were neglected leading to loss of steadiness and symmetry. In 1990, with the introduction of the deep-plane rhytidectomy, the rejuvenation of the mid-face was dramatically improved. Surgeons started to method this area by way of a decrease blepharoplasty incision and thru a temporal incision with the assist of endoscopes. Different methods with slings and suture suspensions of the malar fat pad had been developed. However, perhaps the largest development within the rejuvenation of the mid-face during the last decade was a greater understanding of the aging changes that happen within the space. In addition to the modifications within the pores and skin envelope, important adjustments occur within the delicate tissues and underlying craniofacial skeleton. This idea led surgeons not only to reposition the tissues, but in addition to augment them to achieve a more pure outcome. It is arbitrarily outlined as the realm between the mid-horizontal orbit and the mandibular margin. Medially, the nasofacial groove and nasolabial fold separate the mid-face from the nasal and upper lip subunits. This construction is a triangular thickening of the subcutaneous fat in the cheek space overlying the maxilla. Distinct compartments have been identified within the mid-face: these embody the nasolabial; medial and middle cheek and lateral temporal-cheek; and the inferior and lateral orbital compartments. This adipose tissue is much smaller than the malar fat pad, however its elevation or elevated quantity can significantly enhance leads to midface rejuvenation. The suborbicularis oculi fat has been described as two distinct fat pads, a medial compartment that extends form the medial limbus to the lateral canthus and a lateral element that extends from the lateral canthus to the temporal fats pad. These muscular tissues are additionally concerned in protecting the eye and contribute to oral competence. They embrace the orbicularis oculi, zygomaticus main and minor, levator labii superioris, alae nasi, (levator alae nasi), levator anguli oris, risorius, and buccinator. Its importance lies in the reality that the frontal department lies within this fascial layer. The superficial layer attaches within the lateral facet of the zygomatic arch while the deep layer attaches within the medial facet. However, in respect to the trans-temporal approach, the anatomy of the temporal department becomes important. This branch, or branches since there are often multiple exit the parotid gland and crosses the zygomatic arch roughly in its middle third. One can observe the relationships between the facial nerve exiting the parotid gland and crossing superficially to the zygomatic arch and the intermediate temporal fats pad. However, as a result of the eyebrow is a considerably imprecise landmark in some patients, a more consistent approximation is the line that begins at the inferior facet of the ear lobule and bisects another line connecting the superior border of the tragus to the lateral canthus. Nevertheless, a extra correct means to identify the location of the temporal branch of the facial nerve precisely was described by Sabini et al. One in particular, the sentinel vein, is bigger than the others and is usually located 1 cm from the frontozygomatic suture line. The former exits the cranium through the infraorbital foramen and supplies skin of the cheek, decrease lid and higher lip. The latter exits by way of the physique of the zygoma and supplies the lateral templar region of the scalp. The skeletal framework of the mid-face is composed of three bones: the zygomatic arch of the temporal bone, the zygomatic bone, and the maxilla. Only the zygomatic bone and maxilla are seen within the frontal view, whereas the zygomatic arch turns into important in indirect and lateral views. The lateral projection of the zygomatic bone ought to be the very best level and highlight of the cheek prominence. A robust skeletal framework is associated with a sure sense of youth and beauty. Mid-face Aging A lack of a real scientific understanding of the results of aging on the pores and skin, subcutaneous fats, superficial and deep fascia, muscular tissues of facial features and skeletal framework is the factor most probably responsible for suboptimal outcomes of facial rejuvenation procedures. The youthful mid-face varies in soft-tissue volume but should have a triangular configuration with a mild curved look overlying the zygomaticomaxillary space. The chronologic sequence of aging-related events begins on the third or fourth decade, when a gradual process of weakening of the structures of the face takes place resulting within the characteristics related to the aging-face syndrome. The brow begins to descent related to pores and skin laxity and redundancy of the upper eyelid and frown strains turn into more outstanding. Mid-facial constructions appear to descend together with noticeable tissue atrophy, further increasing the nasolabial fold prominence and making a skeletonization of the decrease lid, facilitating pseudoherniation of the orbital fats by way of the orbital septum. An intensive body of information is available in regard to age-associated pores and skin adjustments. The extrinsic factors are related to the results of the surroundings corresponding to sun exposure, smoking, important weight loss, stress, systemic sickness and even smiling habits. The shifting of the subcutaneous tissues will create and irritate folds and creases, and pigmentary modifications will occur over time along with the appearance of coarse wrinkles and a tough pores and skin surface. Associated with these adjustments, mottled pigmentation, lymphocytic infiltration and an elevated variety of melanocytes may be found within the skin. In respect to the midface, the areas where hyperfunctional rhytids become essential are around the eyes and the nasolabial fold. The zygomaticus minor and main will make the nasolabial fold more pronounced because of repeated contraction when smiling. It had all the time been accepted that the aged face sags largely secondary to gravity, but this hypothesis has been beneath severe scrutiny over the past decade. A compelling study by Lambros,39 analyzing images of patients at different ages by superimposing the pictures, reported the lid-cheek junction, the orbicularis wrinkles and moles on the cheeks to be stable over time. He concluded that a vertical descent of pores and skin was not a significant element of growing older in the mid-face. The writer attributes the phantasm of lower-lid lengthening to lid-cheek junction changes in shadows which would possibly be created by orbital fats protrusion with relative skin immobility. Even though most authors agree with the idea of modifications in mid-face quantity, the soundness of the lid-cheek junction has been contested. The protrusion of orbital fat by way of a weakened orbital septum will create a double convexity in this area. The mid-face ages along with the lower lid in the same manner that the higher eyelid ages with the brow.
Hedysarum tuberosum (Kudzu). Priligy.
- Are there any interactions with medications?
- Dosing considerations for Kudzu.
- Are there safety concerns?
- How does Kudzu work?
- Symptoms of alcohol hangover (headache, upset stomach, dizziness and vomiting), chest pains, treatment of alcoholism, menopause, muscle pain, measles, dysentery, stomach inflammation (gastritis), fever, diarrhea, thirst, cold, flu, neck stiffness, promoting sweating (diaphoretic), high blood pressure, abnormal heart rate and rhythm, stroke, and other conditions.
- What is Kudzu?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96732
Buy generic priligy 90mg online
Recent studies implicating EoE as a reason for airway reconstruction failure recommend children with infected airways should undergo esophageal biopsies to rule out this situation erectile dysfunction at age 23 30 mg priligy generic with amex. Specific therapies and algorithms proceed to be developed for this comparatively just lately described illness muse erectile dysfunction wiki 30mg priligy discount amex. In such a affected person, a concurrent gastrostomy tube could additionally be warranted to make positive the success of the airway reconstruction. Another analysis software within the appropriately aged and developed youngster is computerized voice evaluation. Coexisting conditions, especially craniofacial anomalies and continual lung illness, ought to give one pause prior to embarking on an extensive surgery that may present for a more anatomically patent airway, but functionally has no impression on the kid. The majority of kids with airway disorders need analysis by a multi-disciplinary group that often includes pediatricians, pulmonologists, gastroenterologists, speech-language pathologists, and psychologists along with otorhinolaryngologists. The rise of comprehensive aerodigestive facilities across the country supplies the chance for coordinated care in one location. Changes in health-care reimbursement will dictate that these facilities decide high quality measurements to reveal the superior results that most professionals involved really feel these multi-disciplinary facilities provide. Imaging Imaging research present an adjunct to bodily examination and diagnostic laryngoscopy and bronchoscopy. It is especially important to rule out any lesions that could presumably stop definitive distal airway institution. For example, the senior author has experienced a quantity of occasions by which mediastinal lymphomas recognized on pre-operative imaging have considerably compressed the distal trachea. In these instances, consideration might must be given to bypass or extra-corporeal membrane oxygenation to avoid airway compromise. Airway fluoroscopy can even assist in identifying intrinsic airway narrowing or tracheomalacia. A concurrent modified barium swallow might help to assess aspiration problems, and at the identical time identify extra-luminal compression from vascular rings or slings. Treatment and Follow-Up the advances of pediatric-airway reconstruction are properly documented and have become a cornerstone in the training of pediatric otorhinolaryngologists. T-tube stents can be utilized in multilevel areas of obstruction (ie, trachea and glottis) both temporarily and long run. They are most appropriately used as a temporary measure prior to definitive surgery, however they could be required long run in situations where airway reconstruction has failed. Hospital assist personnel ought to be nicely trained in assessing and managing T-tubes in the perioperative period. In basic, tracheal stents are to be thought of only as a last option within the airway management algorithm or in cases of palliation. They are fraught with issues corresponding to extreme granulation tissue formation, propensity to migrate, and problem in removing. Supraglottic Stenosis Treatment for supraglottic stenosis is determined by the location of the lesion. For arytenoid prolapse, a comparatively easy method is partial laser arytenoidectomy. Glottic Stenosis Glottic stenosis normally is due to extended intubation resulting in posterior glottal scarring. Various open and endoscopic techniques have been advocated depending on the situation of the scar, the maturity of the scar, and the severity of the stenosis. Endoscopic laser software, lateral cordotomy, balloon dilatation, advancement flaps, and posterior cartilage grafting have been described within the literature for posterior glottic stenosis. It should be noted, nonetheless, that posterior grafting is an optional therapy of bilateral vocal cord paralysis as nicely. It is debatable whether or not endoscopic or open approaches are more profitable within the treatment of posterior glottis stenosis; though the literature suggests that more extreme stenoses may be higher suited to correction by an open approach. The administration of acquired anterior glottis stenosis is similar to the administration of congenital webs and stenosis as discussed in Chapter seventy five, "Congenital Anomalies of the Larynx and Trachea. Minimal stenoses, similar to seen in Grade 1 or delicate Grade 2 stenoses, are likely to be managed without intervention in plenty of kids. An otherwise healthy athletically active baby could additionally be extra symptomatic, thus requiring a extra aggressive management technique. Both endoscopic and open-airway surgical procedure options can be found relying on the variables talked about above. It is difficult to examine success rates of balloon intervention versus open-airway procedures in revealed retrospective series because of uncontrolled variables corresponding to grading of preliminary lesion severity, affected person comorbidities, and definition of success. Operative method choices embody balloon dilatation management, anterior cricoid split, augmentation choices with autogenous cartilage, and cricotracheal resection. A resurgence of endoscopic dilatation occurred in the past decade with the event of balloon technology. Prior to the advent of open-airway surgical procedure, rigid dilatation was the primary remedy for airway stenosis. Balloon expertise is over 1 / 4 century old, but solely inside the past 10 years has it gained widespread use in pediatric-airway surgical procedure. There are solely limited case collection describing the utilization of balloon dilatation as a major treatment for subglottic stenosis. It also has been generally used as an adjunct after open-airway procedures to prevent early stricture and scar recurrence in a newly reconstructed airway. Along with balloon know-how, microlaryngeal instruments and laser expertise additional growth of anesthetic techniques, have made endoscopic treatment a viable various in chosen sufferers. These advances in expertise and patient-management methods provide for the possibility of lessened operative morbidity, shortened hospital stays, and decreased risk of extended sedation. Thus, as a major modality, endoscopic treatment can be used in early stage stenosis and in severe stenosis as an adjuvant to open-airway procedures during which the prevention of early scar formation after surgical procedure is fascinating. Adjuvant medical therapy for primary-airway management contains the endoscopic administration of intralesional corticosteroids and topical medications such as mitomycin. This process was initially devised to keep away from tracheostomy in neonates with early stenosis that had not yet developed into extreme, mature stenosis. Variations of this procedure embrace thyroid or auricular cartilage onlay grafts over the split anterior cricoid, and the addition of a posterior cricoid incision. More recently a mixture of endoscopic division with balloon dilatation has been advocated. Based on the experience with anterior cricoid splits in neonates, the single stage procedure was developed with an endotracheal tube offering a short-term airway stent. Relative contraindications to a single-stage procedure embody average to severe tracheomalacia, neurogenic defects, continual lung illness, and craniofacial or airway anomalies that may make intubation troublesome or decannulation inappropriate. Auricular cartilage may be too malleable to be used as an interposition graft; its major use could also be in conjunction with anterior cricoid splits in the very infants in whom it can act as an onlay "cap" graft that overlies the cut up cricoid cartilage.
Priligy 90 mg generic without prescription
When the incision extends beyond the canthus erectile dysfunction medication canada priligy 90 mg generic online, it stays horizontal erectile dysfunction natural supplements cheap priligy 30 mg without a prescription, not downward sloping. When performing simultaneous higher and lower blepharoplasty, the lateral aspect of the lower eyelid incision ought to remain no less than six mm inferior to the upper incision line to prevent prolonged postoperative edema and delayed healing. The lateral extent of the decrease eyelid incision is decided by the amount of skin resection necessarybut normally ends near the lateral orbital rim. A 4 mm skin-only flap is created by undermining inferiorly alongside the whole horizontal extent of the incision. Minimal cautery of the underlying orbicularis minimizes injury to the nutrient supply beneath the skin development flap. The orbicularis muscle is incised roughly four mm inferior to the cutaneous incision and bluntly dissected from the underlying orbital septum. The thin septae dividing the orbital fat are divided with scissors, monopolar cautery or radiofrequency unit, or an incisional laser. The surgeon should reduce traction on the orbital fat to avoid inadvertent posterior hemorrhage. The fats is eliminated and hemostasis is achieved by cauterization underneath direct visualization. The surgeon incessantly redrapes the skin-muscle flap to observe the contour and ensure accuracy of the preoperative plan. Cauterization of the orbital septum could lead to postoperative cicatricial eyelid retraction and should be averted at all prices. When skin excision is carried out, the beforehand undermined pores and skin is re-draped over the lower eyelid and the affected person is requested to look upward and open the mouth while the surgeon gently ballottes the globe to stretch the re-draped pores and skin. The redundant skin shall be superior to the infraciliary incision, and may be excised using scissors. The cutaneous incision is repaired utilizing a working absorbable or non-absorbable suture. All sufferers undergoing decrease eyelid skin excision will develop some extent of ectropion. Special precautions and cautious technique usually produce acceptable if not negligible amounts of lower eyelid malposition. To minimize lower eyelid malposition further in these sufferers, the preoperative evaluation should identify patients with preexisting lower eyelid laxity to modify the surgical plan. Patients with little or no horizontal eyelid laxityshould usually endure concomitant lateral canthal plication. The medial side of the lateral canthal tendon is grasped with toothed forceps and superior laterally till the specified horizontal pressure within the lower eyelid is achieved. An absorbable suture on a small half circle needle engages the medial aspect of the lateral canthal tendon and plicates it to the internal facet of the lateral orbital rim periosteum just superior to Whitnall tubercle. Patients with preexisting decrease eyelid laxity should typically bear concomitant lateral canthal resuspension. After lateral canthotomy and cantholysis, the quantity of lateral eyelid to be removed is decided by greedy the eyelid margin and applying it laterally simply superior to Whitnall tubercle till the eyelid is under the specified pressure. The anterior and posterior lamellae are divided laterally to this point with Westcott scissors alongside the gray line. The mucocutaneous junction is excised and the posterior side of the eyelid shortened with Westcott scissors to create a strip of tarsus. The conjunctiva along this strip is denuded and the strip of tarsus is advanced laterally to the periosteum in the region of Whitnall tubercle with a double-armed suture. The orbicularis lateral to the canthal angle could additionally be closed with absorbable suture. During pores and skin re-draping a score is created within the pores and skin flap corresponding to the lateral extent of the eyelid incision to redrape the realm of the lateral canthus appropriately. Similar to upper blepharoplasty, correct identification and considerate evaluation of problems will allow for profitable managementin most cases. Similar to higher blepharoplasty, affected person dissatisfaction with cosmesis represents the most typical complication of decrease blepharoplasty. Postoperative decrease eyelid asymmetry tends to be considerably better tolerated and fewer severe than in the upper eyelids when correct technique is applied. Similar to higher blepharoplasty, all pre-existing asymmetries have to be identified to the affected person previous to the operation. Also much like higher blepharoplasty, all limitations of lower blepharoplasty have to be completely mentioned with the affected person prior to ther operation. Lower blepharoplasty additionally typically fails to correct the hypertophic orbicularis oculi muscle. Asymmetries due to decrease blepharoplastyinclude some which would possibly be just like higher blepharoplasty, including varying degrees of steatoblepharon undercorrection or overcorrection and cutaneous redundancy undercorrection or overcorrection. Removal of a small residual area of fat or pores and skin is far more simple than changing overly excised fat or skin. Asymmetries not acquainted to upper blepharoplasty embody these related to lower eyelid position. While upper blepharoplasty rarely ends in upper eyelid ptosis, decrease eyelid malposition is an all too frequent complication of lower blepharoplasty. Postoperatively, untoward scarring might produce visible cutaneous scars in cases of skin excision. If the incision is made too near the lash line, the scar can seem indented and the resultant darkish shadow can seem similar to eyeliner. Patients will also observe totally different positions of the eyelid scar, and it is important to make the incisions in identical locations on each lower eyelid. Lagophthalmos might occur following lower blepharoplasty, and virtually always results from aggressive pores and skin removing in the setting of preexisting lower eyelid horizontal laxity and/or creation of a middle lamellar tether from surgical procedure. This syndrome, referred to as post-blepharoplasty lower eyelid retraction may be devastating to the patient and sometimes requires significant reconstructive surgical procedure. It may be avoided in virtually all patientswith proper identification and treatment of preexisting decrease eyelid laxity, mild treatment of the orbital septum, and cautious conservative pores and skin excision. Maneuvers to avoid extreme skin excision embody: ballotting the globe to herniated the fats forward, asking the patient to open the mouth and lookup, all to hold the skin on stretch. Conversely, the condition may not be apparent for as much as a number of weeks after the operation. It then evolves to worsen over the course of several weeks and then gradually improves over many months. Temporizing measures include eyelid therapeutic massage, corticosteroid or antimetabolite injection, and lateral tarsorraphy. In basic, the surgeon ought to resist the urge to provide extra aggressive surgical intervention for a number of months, as early interventions have a high failure price and may cause extra problems. While some surgeons find that resuspension and orbicularis slings improve the condition, we find that the majority sufferers eventually require a cheeklift to recruit anterior lamellar tissues and a posterior lamellar graft with either exhausting palate or acellular dermal allograft.
Order priligy 60 mg overnight delivery
Additional concerns in history-taking include the response to prior remedy and evidence of problems female erectile dysfunction treatment priligy 90 mg buy low price. In kids otc erectile dysfunction drugs walgreens 30 mg priligy with amex, this can be manifested as adenoid facies with a high palatal arch, and irregular dental improvement. In adults, nasal obstruction may contribute to loud night breathing and sleep-disordered respiration. The medical history might document systemic disorders that have an effect on the nose, corresponding to hypothyroidism. Pregnancy can produce nasal congestion and should require modification of therapy methods. Between 5 and 10% of asthmatic subjects could have intolerance to aspirin and nonsteroidal antiinflammatory medicine. The frequency of aspirin intolerance in patients with nasal polyposis is about 23%. Nasal signs might also be because of intake of medicines corresponding to � blockers, which can contribute to nasal congestion by way of interference with the adrenergic mechanism. Tricyclic antidepressants may produce dryness of the nasal mucosa by virtue of their anticholinergic results. Examination Attentive history-taking and bodily examination, combined with appropriate diagnostic checks, are required for establishing the proper prognosis, as a result of allergic rhinitis shares options of different nasal disease entities. The classical description of allergic facies consists of mouth respiratory, allergic "shiners" (resulting from periorbital venous stasis from chronic nasal obstruction), and a transverse supratip nasal crease from long-term rubbing of the nose upward to relieve itching. Ocular examination could reveal injection of the conjunctiva or swelling of the eyelids. Examination of the nose begins with observing the external appearance for gross deformities similar to a deviation suggesting earlier trauma, or enlargement of the nasal bridge suggestive of nasal polyps. A nasal speculum permits analysis of the anterior third of the inner nasal architecture and the character of the nasal mucosa. Structural anomalies offering an anatomic foundation for obstruction or recurrent infections corresponding to septal deviations or spurs must be sought. Decongestion of a swollen nasal mucosa with a topical decongestant improves visualization of the nasal cavity and allows the differentiation of reversible from irreversible changes. Combining the vasoconstrictor with a topical anesthetic allows full examination with an endoscope. The region of the middle meatus also wants to be examined rigorously as a result of secretions there might be suggestive of acute or persistent sinusitis. Sensitization implies the presence of elevated ranges of IgE directed towards a specific allergen and may be demonstrated by a wheal and flare response to skin testing with allergen extracts or by measurement of the level of antigen-specific IgE antibodies in the serum. However, individuals can present proof of sensitization by a optimistic skin take a look at or elevated particular antibody ranges in the serum with out having proof of scientific illness. This emphasizes the significance of obtaining an excellent historical past within the analysis of patients with suspected allergic disorders. In sufferers with a constructive history, the magnitude of skin responses usually corresponds to the severity of signs. Skin Testing Skin testing furnishes a superb in vivo technique for demonstrating sensitivity to a given allergen. This take a look at evaluates the presence of specific IgE antibodies on pores and skin mast cells, the reactivity of these cells, and the reaction of the top organ to released mediators. Its advantages include nice sensitivity, the rapidity with which ends up can be obtained, and low cost. In Vitro IgE Measurements Drawing blood for the measurement of specific IgE can circumvent a variety of the disadvantages of pores and skin testing. False-positive outcomes may happen if sufferers have elevated IgE levels in their sera because of nonspecific binding of IgE antibodies. False-negative outcomes can also happen from inhibition by IgG antibodies which have affinities just like these in patients receiving immunotherapy. Disadvantages of in vitro testing embrace price, barely decrease sensitivity, and the time delay between drawing blood and acquiring the outcomes. Other Diagnostic Tests Peripheral eosinophilia, although nonspecific, could point out the presence of atopic diseases. Nasal cytologic examination permits the identification of eosinophils and different inflammatory cells in nasal secretions and could additionally be useful in the differentiation of an infectious from an allergic trigger throughout a scientific exacerbation of symptoms. In regular people, smears show the presence of epithelial cells, together with some ciliated and goblet cells, with few eosinophils, neutrophils, basophils, or bacteria. In topics with an infection, neutrophils increase in nasal secretions, and in symptomatic allergic subjects, the proportion of eosinophils will increase. A value higher than 10% for eosinophils is suggestive of allergic disease; nonetheless, eosinophils may also be current in the absence of IgE-mediated illness. Sinus disease typically complicates perennial allergic rhinitis and may must be thought-about in the differential analysis. The common affiliation of higher and lower airway disease makes checks of pulmonary operate a helpful adjuvant. This assertion applies to such numerous issues as cystic fibrosis, bronchial asthma, and bronchopulmonary aspergillosis. The giant variety of potential environmental threat components and the shortcoming accurately to predict the event of bronchial asthma and allergy resulted in conflicting knowledge from current prevention research. Environmental modifications encompass removing of particular antigens and the removing of irritants. Avoidance of exposure to environmental tobacco smoke may be beneficial safely for the entire population, not just for prevention of allergy, but in addition for other identified benefits. Although perfectly logical, the benefit of other avoidance measures in the presence of excellent pharmacotherapy has been questioned. Complete avoidance of the allergen(s) to which the affected person is delicate eliminates signs of the disease. In seasonal allergic rhinitis, sufferers can scale back exposure by maintaining home windows closed on days when pollen counts are excessive and limiting physical exercise outside within the early morning and evening when pollen counts are at their peak. Air conditioning may help, and the addition of particular filters can forestall pollen grains and mold spores from entering the home. These include changing feather pillows and bedspreads with synthetic ones that can be washed in sizzling water (hotter than 130�F) and masking mattresses with commercially out there impermeable covers (pores <10 m). A research confirmed that washing clothing with detergent plus bleach removes a significant portion of mites, and repeated washing is suggested to cut back the mites additional. Stuffed toys may be positioned in the freezer for two days for lowering the variety of mud mites. Reduction within the allergen load after pet removing could take as much as six months, nonetheless, and thus signs might persist. Furthermore, full removal of a pet could additionally be difficult, but eliminating the animal from the bedroom, where we spend an average of eight hours per day, is taken into account a helpful different. It is more than likely that cat dander is carried into lecture rooms on the garments of a cat proprietor. The use of high-efficiency particulate air filters and of electrostatic filters effectively removes particulates larger than 1 �m in diameter. The finest and most cost-effective approach to all filtration may be to think about "combination filtration", ie, high-efficiency whole-house filtration with a transportable room air cleaner, or respiratory zone filtration within the bed room.
Priligy 90 mg purchase visa
In addition to post-blepharoplasty decrease eyelid retraction impotence vitamins supplements buy priligy 90mg lowest price, different complications distinctive to decrease blepharoplasty may happen impotence drug purchase 90mg priligy otc. When decrease eyelid tightening is carried out, patients can develop a suture granuloma in the space of the re-suspension suture. This downside usually resolves with heat compresses but often might require oral antibiotics or removing of the offending suture. Worsening of malar baggage is ubiquitous after lower blepharoplasty, and this chance ought to be mentioned with the affected person. Fortunately, close to all patients improve to their preoperative stage within a few weeks of the operation. Persistent decrease eyelid conjunctivochalasis may sometimes happen after trans-conjunctival blepharoplasty. This situation sometimes improves with time or ophthalmic corticosteroid ointment but sometimes could require additional surgical procedure. It is usually the result of unsuspected lagophthalmos, so care ought to be taken to rule out other problems that would produce exposure keratoconjunctivitis. The occurrence of lower entropion should be extraordinarily rare within the setting of properly performed decrease blepharoplasty, however latent preexisting entropion could be unmasked by the procedure. Issues widespread to higher blepharoplasty, similar to wound dehiscence, wound an infection, globe injury and hemorrhage are discussed within the upper blepharoplasty part of this chapter. Although these tissues possess major aesthetic roles, the eyelids firstly serve a functional position to defend and nurture the attention. Even small alterations in these finely orchestrated functional responsibilities can have severe and even permanent results on vision. Therefore, surgical procedures involving these buildings must first protect function. The upper and decrease eyelids differ within the gravitational and involutional stresses they bear. Similarly, though each upper and decrease blepharoplasty recontour the eyelids, they represent fairly completely different surgical procedures because of the differing anatomic and pathophysiologic changes they handle. Despite these variations, upper and decrease blepharoplasty share basic ideas essential to surgical success and affected person satisfaction. A crucial part of this process is the surgeon reconciling affected person expectations with surgical realities to minimize dissatisfaction and morbidity. With these ideas in thoughts, blepharoplasty presents a singular opportunity to handle patient particular objectives to restore a younger appearance whereas preserving operate. The Asian upper eyelid: an anatomical research with comparison to the Caucasian eyelid. Mechanical properties and microstructure of the superficial musculoaponeurotic system. Contact dermatitis to topical drugs: a retrospective chart evaluate from the Ottawa hospital patch take a look at clinic. Changes within the facial skeleton with aging: implications and medical functions in facial rejuvenation. Laser blepharoplasty with transconjunctival orbicularis muscle/septum tightening and periocular pores and skin resurfacing: a protected and advantageous approach. Lower eyelid place after transconjunctival lower blepharoplasty with versus with no skin pinch. Dry eye and chemosis following blepharoplasty: a 10-year retrospective evaluate of 892 cases in a single-surgeon. Revisional eyelid surgery: therapy of extreme postblepharoplasty lower eyelid retraction. Comparison of the efficacy of hard palate grafts with acellular human dermis grafts in lower eyelid surgery. The eyebrows begin to descend and flatten, resulting in lateral hooding of the higher eyelid area. Lax and redundant eyelid pores and skin, together with the appearance of fats protrusion, can be a element of the getting older higher third of the face. Rejuvenation of the mid-face consists of addressing the malar complicated and its relationship to the lower eyelid and nasolabial fold. The major focus of the chapter is to provide an outline of the surgical methods that are out there for addressing the aged mid and upper thirds of the face. The galea aponeurosis is a thin, mobile, fibromuscular sheet that envelops the whole skull and splits anteriorly to encase the frontalis and procerus muscle tissue. The unfastened areolar tissue airplane is a comparatively avascular aircraft and the normal layer of dissection for coronal approaches. This layer is steady with the free connective tissue which separates the temporoparietal fascia and the deep temporal fascia. The pericranium is a thickened layer of connective tissue adherent to the skull and is steady with the periorbita on the degree of the supraorbital ridges. It is the mimetic actions of those muscles that produce the wrinkles and furrows in the skin of the forehead and glabellar areas. The corrugator and procerus muscle tissue are often surgically weakened in the correction of the getting older brow and forehead. These muscles are also the targets of temporary chemodenervation by the injection of botulinum toxin. The temporal fossa is bounded inferiorly by the zygomatic arch and anteriorly by the frontal means of the zygomatic bone. The temporoparietal fascia is a thin, vascular layer, densely adherent to the overlying subcutaneous tissue and pores and skin. The deep temporal fascia envelops the temporalis muscle and divides right into a superficial and deep layer at roughly 2 cm above the zygomatic arch. The arch and the temporal fats pad are ensheathed by the superficial and deep layers of the deep temporal fascia. Understanding the course of the temporal department of the facial nerve is critical to protected dissection in this space. The nerve enters the temporal fossa by crossing superficially over the mid-portion of the zygomatic arch. Periorbital Complex the eyelids are formed by multiple delicate tissue layers and are divided into an anterior lamella, composed of pores and skin and orbicularis muscle, and a posterior lamella, composed of the tarsus and conjunctiva. The preaponeurotic fat is subdivided into two compartments in the higher lid: medial and central. In the decrease lid, the fats lies in three compartments: medial, central, and lateral. Temporoparietal fascia Loose areolar tissue Superficial layer Deep layer Deep temporal fascia the levator palpebrae superioris muscle is the primary elevator of the upper eyelid and is innervated by the oculomotor nerve. The levator muscle arises from the orbital apex and courses anteriorly the place it thins to a broad aponeurosis that inserts onto the anterior floor of the tarsal plate. The supratarsal crease is created by anterior extension of some of the fibers to attach to the dermis of the eyelid skin. Acquired ptosis of the upper eyelid often is a result of levator dehiscence from the tarsal plate and have to be identified preoperatively. Fat-repositioning procedures target the arcus marginalis as the positioning of fat release.