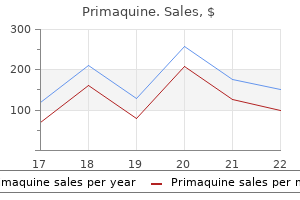
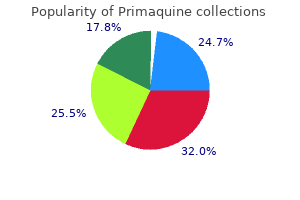
Primaquine
Primaquine dosages: 15 mg
Primaquine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 240 pills, 300 pills

7.5 mg primaquine cheap fast delivery
The pre-calculated table is then used to present an overall rating treatment joint pain cheap primaquine 15 mg with mastercard, which in this instance is 21 treatment rosacea primaquine 15 mg order on-line. In this study, all affected person targets have been achieved inside the timeframe and the agreement between raters was excessive. Significantly, it was found to be strikingly extra responsive than the other measures. They studied the similarities and variations in patient-set versus physiotherapist-set targets. Therapists regularly select impairment-level objectives and patients extra regularly set activity stage targets. Findings showed that objectives set by therapists were extra often achieved than those set by sufferers. In conjunction with this, the therapist sets an impairment-level objective which helps the achievement of the exercise the affected person has recognized. Therapists must have the power to define the construct they wish to consider and have the knowledge base which allows them to select measurements appropriately. At the core of the Bobath Concept is the popularity that each patient must be treated as an individual. A further problem with standardised measures is that they often lack the ability to show change within the efficiency of qualitative useful motion which treatment strives to promote (Paci 2003). Therapists need to develop the skills that can allow them to choose measurement tools primarily based on knowledge of their psychometric and scientific properties. International Bobath Instructors Training Association (2004) Theoretical assumptions and clinical apply (Internet). World Health Organization (2001) International Classification of Functioning Disability and Health. Inability to rise from a sitting place is recognised by the World Health Organization as a disabling situation and is considered a predictor of future incapacity. Its qualitative efficiency has implications for so much of other actions and has also been linked with prediction of effectivity in gait (Chou et al. In every day life, moving between sitting and standing is carried out many occasions a day in many various contexts. This complicated and biomechanically difficult task may be performed in isolation however is more generally accomplished as a half of different practical duties such as toileting, dressing and getting out of a automobile. These elements of postural management have been discovered, developed and modified primarily based on prior movement experiences. However, with ageing, harm or impaired movement management, the conventional components and sequencing may be lost resulting in the usage of different compensatory methods to regain function. This basic exercise with its implications for independence and high quality of life requires considerable therapy time, with as a lot as 25% reported to be devoted to this area (Jette et al. Based on scientific reasoning, the Bobath therapist can focus therapy on the acquisition of particular parts of the movement sequence in several postures, environments and contexts. Emphasis is positioned on: alignment, range and sample of movement, timing, pace, power, postural management. Integration of those parts into the efficiency of the duty in a selection of settings is important for carry over into perform. Common constraints within the literature include beginning place, seat peak, foot place and higher limb position. Seat top A variety of researchers have considered this aspect not solely by method of setting the extent as a normal relative to the length of levers within the particular person, but also comparing the effectivity and energy stage at totally different heights (Mazza et al. This ought to be progressively adapted to enable the affected person to achieve optimal motor performance. Within the Bobath Concept, these compensatory methods are also minimised by therapeutically enhancing motor performance. Carr and Gentile (1994) demonstrated that when the upper limbs have been restricted, regular topics transferred their physique mass forward less at thigh-off, and there was a greater challenge to steadiness. Clinically, if upper limb involvement is impeded, for example by low postural activity, malalignment, hypertonia or biomechanical adjustments, the qualitative efficiency will be lowered. The upper limbs are often unable to contribute actively to the switch and will even intervene with it as illustrated in the medical example at the finish of this chapter. A robust temporal coupling of activity between upper and lower limb was identified. Normally, upper limb use is dependent upon numerous elements together with how far again the individual is in the seat, slope of the seat or peak of the seat relative to leg length. The upper limbs could also be used to help the trunk transferring ahead, to present momentum or to help in elevating the body at seat off. Although these stages are often described separately, they type a continuum with the entire sequence often carried out in lower than 2 seconds (Chou et al. Therefore, the task requires the person to overcome inertia, gain momentum, and control acceleration and deceleration. Stage 1: Flexion momentum begins with initiation of the movement and ends just earlier than the buttocks raise from the chair (seat off) this description is predicated upon the subject ranging from an unsupported sitting place. In relaxed sitting, the pelvis is often in a level of posterior tilt and the pelvis moves towards anterior tilt during this part of forward flexion of the trunk. This 86 Moving Between Sitting and Standing ensures that the physique weight is raised by segmental, synergistic trunk and pelvic activity. Trunk extensor muscles and belly muscle co-activation are required to produce linear extension on a stable base created by way of the alignment and activation of the decrease limbs. Clinical experience means that gaining this efficiency in recruitment of trunk exercise to transfer the body weight upwards and forwards requires a selection of elements to be thought-about. These embody: starting posture, degree of support, postural alignment and exercise, relative seat top and floor. Patients with poor postural management of the trunk and associated difficulty creating an optimal alignment may have preparation of activity at this stage. This underpins the medical position of facilitation of antigravity activity exerted from the pelvis and hips in a lateral or antero-posterior direction necessary earlier than forward flexion of the trunk. This improves timing and feed-forward control and should minimise undesirable compensatory methods. Since the model new base of assist is relatively small, alignment, exercise and stability within the ankles and toes are essential. Dynamic stability and flexibility inside the foot is required all through all phases of the transitions. Interference components corresponding to restricted vary of movement or altered tone must be considered along with the selection and use of orthoses which may impact on foot mobility. Appropriate alignment of the decrease limbs can have a significant impact on the timing and sample of muscle activation at this stage and into the extension part. For example, a patient with a quantity of sclerosis, with increased muscle tone within the hip adductors, could use a strategy of increased hip flexion and anterior tilt in the course of the ahead momentum part, rising the problem of the rise into extension.
Primaquine 7.5 mg generic on-line
This is in distinction to express studying involving higher-level cognitive functioning associated to specific areas of the mind administering medications 7th edition ebook 7.5 mg primaquine discount free shipping. Neural mechanisms that combine posture and movement are widespread throughout the nervous system and are recruited in patterns which might be both task and context particular (Stuart 2005) treatment buy cheap primaquine 7.5 mg. The studying of expert motor actions, producing smooth, coordinated patterns of movement, requires precise temporal coordination of muscular tissues and joints that are practised many occasions over (Nudo 2007). Internal fashions, involving sensorimotor maps, are utilized by the nervous system for anticipatory adjustments within the development of expert movement (Takahashi & Reinkensmeyer 2003). Therefore specificity of apply allows the affected person to entry extra appropriate patterns of exercise, which is important in therapy to promote the restoration of skilled useful actions. This is supported by a latest study by which motor improvements were seen when the patient was attentive to the patterns of exercise rather than the motor end result (Cirstea & Levin 2007). However, too much express instruction relating to efficiency may intrude with implicit motor sequence learning after stroke (Boyd & Winstein 2003). Auditory info is processed cognitively and therefore can intervene with the automated processing of other senses concerned in implicit learning. Concurrent augmented verbal suggestions is recognized as boosting performance, but degrading studying (Jensen et al. Information could additionally be given explicitly to the patient, carer or interdisciplinary group members and should contain elements of: organising the environmental constraints similar to the peak of mattress or work high; constraint of 1 physique part to enable one other to move; alteration of the entire task when it comes to initiation, sequencing, pace and timing of the task; strengthening of specific parts of the duty in functionally relevant situations; acceptable postural orientation for the task; advice to carers or interdisciplinary staff members on handling. There is preliminary evidence that neurofacilitation strategies improve motor perform in stroke sufferers by normalising exercise within the sensorimotor network (Miyai et al. Significant short-term results on gait parameters have additionally been demonstrated using neurofacilitation methods (Hesse et al. The significance of afferent info in the management of motion the hyperlink between cognition, perception and motion has already been recognized in this chapter as being crucial to the achievement of independent and adaptable functional behaviour. Perception is based on info obtained by the nervous system through specific modalities of afferent data together with cutaneous and joint receptors, muscle spindle, golgi tendon organs, vestibular data, vision, auditory information, olfactory data and taste. Through this information we perceive the exterior world, remain alert, kind a physique picture and regulate our actions (Kandel et al. The management of efficient motion requires the person to be tuned into visual, vestibular and somatosensory data (cutaneous, joint and muscle receptors). All of those contribute to the development of an inside representation of physique posture which is referred to because the postural body schema. This supplies a basis for all interactions involving notion and action towards the external world and is more likely to be partly genetically decided and partly acquired through ongoing experiential studying. It is due to this fact adaptable and vulnerable, and depends on the continued info that it receives. The inner representations of physique posture could be considered as a general neural mechanism for resolving sensory problems. They bring together info from many sensory sources, combining incoming and outgoing data (Massion 1994; Perennou et al. It is believed that a central nervous system mannequin of physique dynamics is crucial to anticipatory management of posture during movement (Frank & Earl 1990). The postural body schema consists of: alignment of physique segments to each other and in relation to the setting; motion of the body segments in relation to the base of support; orientation of the physique in relation to gravity (verticality). The integration of visible, vestibular and somatosensory information is advanced and dependent on intact sensory motor networks. This permits for a bias in path of essentially the most acceptable senses dependent on the duty and the environment. The neurological affected person will use obtainable senses which is ready to immediately have an effect on their postural body schema. A common downside which will develop is acquired sensory loss as a result of lack of appropriate use of somatosensory data. Patients with neurological dysfunction usually proceed to rely closely on visible info, limiting the integration of somatosensory information. Systems management of posture and movement the complex picture which is exhibited in sufferers with neurological circumstances almost at all times entails harm to the methods which control posture and voluntary movement. When the descending drive to the spinal twine is disrupted, this results in issues organising acceptable goal-orientated patterns of activity on a background of postural control. The human physique is essentially unstable due to the evolvement of bipedal stance to free the higher limbs for operate. Maintaining stability requires a finely tuned advanced processing of information to find a way to keep appropriate postural stability within the many various postures that are essential for us to operate every day. Postural responses happen in anticipation of and alongside movement, and during sudden perturbations, and are commonly generally known as feed-forward and suggestions management, respectively. Intended actions contain motor planning at a higher stage, including the cerebellum, basal ganglia and cerebral cortex, and form feed-forward mechanisms to adapt motor and sensory systems on the idea of earlier expertise. Automatic responses to sudden perturbations happen on the basis of ongoing visual, vestibular and somatosensory data. Recruitment of applicable musculature to produce rapid postural management methods entails medial descending techniques, including the vestibulospinal and pontine reticulospinal techniques. They act on axial and proximal muscular tissues, and are concerned in sustaining an upright posture and integrating actions of the limbs with the trunk. Lateral descending methods, including corticospinal and rubrospinal methods, are liable for the recruitment of distal muscle tissue and therefore assist postural control through the manufacturing of selective motion (Ruhland & Le van Kan 2003; Schepens & Drew 2004; Lalonde & Strazielle 2007). A major drawback in many sufferers is the weak spot of neural drive to postural muscles which leads to issue producing acceptable antigravity exercise for easy coordinated motion. Muscle weak point and reintegrating afferent information contribute to postural instability in stroke (Marigold et al. This leads to fixation strategies that forestall the affected person from growing adaptable motion and limits their motion choices. Requirements of environment friendly movement Identifying the necessities of environment friendly motion with respect to operate is key to medical reasoning within the Bobath Concept. Postural control is an essential basis for movement with the following being key necessities incorporated into postural management for practical movement: Balance strategies Patterns of movement Speed and accuracy Strength and endurance Understanding how these interlink and influence each other is particularly necessary in understanding the complexity of the management of movement for scientific reasoning. There is little argument in the literature relating to the significance of postural management for environment friendly motion (Pollock et al. It involves the ability to orientate and stabilise the physique inside the pressure of gravity utilizing appropriate stability mechanisms. The recovery of stability is a critical part for reaching independence in the activities of day by day living (Lundy-Ekman 2002). Analysis of postural alignment is an important feature of the evaluation process (Lennon & Ashburn 2000). Bobath therapists analyse posture and movement via the alignment of key factors in relation to one another and in relation to a given base of assist. Key factors are described as areas of the body from which motion might most effectively be managed (Edwards 1996). The distal refers to the palms and ft; the proximal to the shoulder girdles, head and pelvis; and the central to the mid-thoracic area.
Primaquine 15mg generic with amex
Lymphatic drainage of the anterior thoracic wall goes first to the internal thoracic lymph nodes alongside the inner thoracic arteries and veins symptoms of 15mg primaquine cheap visa. The extra frequent scheme of venous drainage on the posterior thoracic wall differs slightly from the one in your text however the sample offered right here on this slide is the one you should be taught medicine during the civil war primaquine 15mg discount. On the best aspect, the first vein drains immediately into the best brachiocephalic vein. The veins from the 2nd to the 4th drain to the right superior intercostal vein which empty within the azygos vein. Note that the azygos vein arches over the basis of the best lung to drain into the superior vena cava. The lymphatic drainage of the posterior wall goes to posterior intercostal and para-aortic lymph nodes. On the left aspect, the first vein drains directly into the left brachiocephalic vein. Then, the veins in spaces 2 to 4 drain into the left superior intercostal vein which then empty into the left brachiocephalic vein. The veins from areas 5 to eight drain into the accent hemiazygos vein with the veins from area 9 to 12 draining into the hemiazygos vein. The thoracic cavity has three compartments: the 2 pulmonary (pleural cavities), which contain the lungs and their surrounding pleural sacs and the mediastinum in between, which incorporates all the opposite thoracic buildings. The mediastinum is a movable compartment, partitioning between the 2 pleural cavities. The mediastinum extends from the thoracic outlet and the foundation of the neck, superiorly, down to the diaphragm. The mediastinum extends anteriorly from the sternum to the 12 thoracic vertebrae of the vertebral column posteriorly. The superior extent is a line drawn between the suprasternal notch of the manubrium to the higher border of the T1 vertebral body. A line between the sternal angle and the T4/T5 intervertebral disc divides the mediastinum in the superior and inferior mediastina. The inferior mediastinum is further divided by the pericardial sac and cavity into anterior, center, and posterior mediastina. The thymus (and/or its remnants) is probably the most anterior structure in the superior mediastinum. It normally extends down into the anterior mediastinum, just anterior to the upper a part of the pericardium. In this figure, the thymus and the anterior wall of the pericardium have been cut away. This lateral view from Netter permits us to visualize the 3 subdivisions of the inferior mediastinum: the anterior, middle and posterior mediastinum. The esophagus is a muscular tube that conveys meals from the pharynx to the abdomen. In the posterior mediastinum, it passes posterior to the left bronchus and the left atrium. It passes posterior to part of the diaphragm, and then through the esophageal hiatus of the diaphragm to the abdomen. It begins in the stomach (cistern chili) on the best side of the aorta (at the level of about L1). As it ascends, it passes with the aorta through the aortic hiatus of the diaphragm, then ascends on the posterior facet (right side) of the esophagus to cross over to the left (at about the stage of T4) earlier than getting into the superior mediastinum to empty usually into the left brachiocephalic vein. The phrenic nerves descend between the pericardium and pleura on each side, anterior to the roots of the lungs. They distribute to the mediastinal pleura after which to the muscle of the dome of the diaphragm (see the thoracic contents lecture). It continues alongside the esophagus because the posterior vagal trunk through the esophageal hiatus into the abdomen. The left vagus nerve passes between left common carotid and subclavian arteries and descends anterior to the aortic arch. The left recurrent laryngeal nerve branch loops beneath the arch, lateral and posterior to the ligamentum arteriosum (an embryological remnant). The left vagus nerve continues posterior to the basis of the left lung and alongside the esophagus as the anterior vagal trunk via the esophageal hiatus. Observe also the proper and left (paravertebral) sympathetic chains and associated structures (ganglia, white and gray rami communicantes) as nicely as the thoracic splanchnic nerves. Recall that preganglionic sympathetic fibers travel in higher splanchnic nerve (T5-9), lesser splanchnic nerve (T10-11), and least splanchnic nerve (T12). D Center for Anatomical Studies and Education Department of Regenerative Medicine and Cell Biology College of Medicine Medical University of South Carolina Slide 1. In this slide, please visualize the constructions that might be discussed in the course of the course of this lecture. The trachea is an roughly 5 inches long, 1 inch extensive, cellular cartilaginous and membranous tube beginning at the lower border of the cricoid cartilage and ending by bifurcating (branching) into the right and the left major (primary) bronchi on the degree of the sternal angle. Recall that the cricoid cartilage (upper finish of the trachea) is on the degree of the C6 vertebra and the sternal angle (lower finish of the trachea) is on the decrease stage of the 4th thoracic vertebra. Note that during a bronchoscopy, a keelshaped anatomical construction, the carina could be noticed on the stage of the bifurcation. In this cross-section of the trachea, we will observe that the trachea: - Has a fibroelastic wall with an embedded collection of U-shaped bars of hyaline cartilage maintaining the lumen patent (open) - Has a mucosa lining the within lumen - Has a band of clean muscle, the trachealis muscle, closing the posterior free end of the U-shaped cartilage. In terms of relationship, the trachea is surrounded by: - Anteriorly: the brachiocephalic trunk and the arch of the aorta (the sternum, the thymus, the left widespread carotid artery, and left brachiocephalic vein) - Posteriorly: the esophagus and the left recurrent laryngeal nerve. In phrases of relationship, the trachea is surrounded by: - On the right side: the azygos vein, the best vagus nerve and the pleura - On the left side: the arch of the aorta, the left common carotid and left subclavian arteries, the left vagus, left phrenic nerve and pleura. The trachea receives its innervation by way of branches of: - the vagus and the recurrent laryngeal nerves - the sympathetic trunks these branches are distributed to the: - the trachealis muscle - the mucous membrane lining the trachea. Understand that the best lung divides into 3 lobes, the superior, the middle and the inferior lobe whereas the left lobe divides in 2 lobes, the superior and the inferior lobe with an extra structure not present in the proper lung the lingual. Note how the right bronchus is wider, shorter and extra vertical than the left bronchus. This is clinically essential as small swallowed foreign objects (like peanuts, cash, and so forth. Observe that: the first bronchi divide into secondary bronchi On the proper aspect, the first bronchus divides right into a superior bronchus and an intermediate bronchus before entering the hilum of the right lung On the left facet, the primary bronchus first enters the hilum of the left lung and then divides into a superior and an inferior bronchus the terms "secondary" and "lobar" bronchi are synonymous terms because the secondary bronchi ventilate the lobes of the right and left lungs. The secondary bronchi additional divide into tertiary bronchi, additionally known as segmental bronchi because they ventilate the bronchopulmonary segments of the lungs (see next). Note that the bronchi continue to endure division till the extent of the terminal bronchiole (up to a total of 27 divisions). They are separated by the heart, the nice vessels and the opposite buildings discovered in the mediastinum. Note that every lung: - Is conical in shape, lined with a visceral pleura and suspended by its root - Has an apex, a concave base that sits on the diaphragm, a convex costal surface and a concave mediastinal surface.
Primaquine 7.5mg safe
Patients should be supplied with recommendation and steering on movement and function medicine park oklahoma primaquine 15mg with mastercard, for the periods between therapy periods medicine knowledge discount 7.5mg primaquine, so as to obtain carry-over. Preventative and promotive features of therapy have to be addressed on a continual basis, and may think about problems with physical and cardiovascular health. Treatment is aimed toward preventing the institution of spasticity and maximising residual operate (Cornall 1991). Therapists can achieve tone discount in numerous methods such as mobilisation of muscular tissues and stiff joints, muscle stretch, apply of more regular motion patterns, and through more environment friendly, much less effortful performance of functional tasks (Mayston 2002). Weight bearing can help influence irregular tone only if the affected person is in a position to adapt and change muscular alignment actively (Raine 2007). Therapists work on tone to enhance movement, to not normalise tone for its personal sake (Lennon et al. Bobath therapists search to find the causal impact of associated reactions somewhat than merely changing the sample produced by the related response. The goal is to management somewhat than inhibit related reactions (Lynch-Ellerington 2000). A primary concern of the Bobath Concept is the activation of the patient to overcome postural hypotonia. There could additionally be many reasons different than just motor problems which can influence posture and balance, corresponding to sensory and perceptual issues. Selective actions of the trunk and limbs, each concentric and eccentric, are interdependent and interactive with a postural control mechanism. Therefore, the recovery of selective movement is a prerequisite for environment friendly postural control, alignment and function (Raine 2007). Balance in an individual is achieved by way of bettering their orientation and stability in relation to postural management (Mayston 2002). There could also be an element of conscious management over muscle tone; however, the purpose is for the affected person to develop management of their steadiness and movement on an computerized basis in order to initiate and management useful movements. It is recognised that some movements might have to be cognitive, similar to some manipulative actions of the hand or throughout studying of goal-directed actions. However, a person who has to take into consideration their stability will be unable to carry out some other activity concurrently (Leonard 1998). Sensory techniques Sensory methods provide important details about both the inner and external environments upon which skilled motion is predicated and refined. At some stages of skill acquisition, somatosensory referencing could additionally be emphasised over verbal or visible suggestions. This change of sensory precedence is essential to cut back compensation methods, such as visual fixation, and challenges the patient to use extra appropriate sensory strategies for the task (postural control, steadiness, stereognosis). Voluntary movement is amongst the most powerful types of sensory stimulation on which more refined movement may be constructed (Leonard 1998). As a half of treatment it is very important create the suitable size and compliance of both muscle and soft tissues to have adequate joint vary to obtain the required practical motion parts. It is also essential to achieve appropriate size for efficient muscle activation (Mayston 2001). Optimising muscle length should incorporate the complex relationship of stability and mobility parts for the task (Mayston 2001). To achieve the appropriate muscle stability for operate, remedy may require selective and particular strength training (Raine 2007). Body weight and gravity can be utilized to strengthen muscle tissue as well as acceptable resisted workout routines (Raine 2007). However, actions should be owned by the affected person and be experienced both with and finally without the handling of the therapist (Raine 2007). Adjuncts to remedy the Bobath Concept can be complemented with other modalities and adjuncts corresponding to structured apply, use of orthotics and muscle strengthening (Mayston 2007). Splinting and orthoses may be indicated to acquire alignment or a good weightbearing base for improved proximal and truncal exercise (Mayston 2001). Restraint of the much less affected body elements manually throughout a therapy session could also be used to assist activation of the affected parts (Raine 2007). The therapist utilises selective constraint via posturing a limb or through an environmental support. To improve postural management or assist reciprocal activity of the decrease limbs as part of the strolling sample, the therapist could select to use a treadmill with or without body-weight support and this could embody facilitation to enable the most environment friendly pattern. The therapist by way of a wide selection of techniques of handling and activating the affected person could make motion needed and attainable, and incorporate these extra environment friendly ways of moving into on a regular basis life (Mayston 2001). Using other techniques in parallel, corresponding to Maitland mobilisations, is suitable with the Bobath Concept (Lennon & Ashburn 2000). A role of the therapist is to facilitate balance and selective movement as a basis for useful activity and 15 Bobath Concept: Theory and Clinical Practice in Neurological Rehabilitation successful aim acquisition. Successful aim acquisition in a given task should then be practised to enhance efficiency and promote generalisation (Raine 2007). Preparation is of no value in itself, however should be included into useful activity, which is meaningful to the affected person in order to promote carry-over (Raine 2007). These developments have been in response to , and supported by, advances in the fields of neuroscience, biomechanics and motor studying. As described by Mayston (2007), there have been many changes within the Bobath Concept and a lot of elements that stay the same. An understanding of tone, patterns of motion and postural management that underlie the performance of useful tasks. Aspects which have modified: Changes in the understanding of tone to embody each neural and non-neural parts. It is important to continually apply and evaluate new information and evidence as it becomes obtainable as a part of the continuing growth of the Bobath Concept. Key Learning Points the systems method to motor management supplies the foundation of the current principle underpinning of the Bobath Concept. Preparation is of no value in itself, however have to be included into useful exercise which is meaningful to the patient, so as to promote carry-over. Plasticity underlies all talent learning and is an element of the nervous systems function. Therapists need to concentrate on the principles of motor studying: energetic participation, opportunities for practice and significant goals. The Bobath Concept may be complemented with different modalities and adjuncts similar to structured practice, use of orthotics and muscle strengthening. In: Upper Motor Neurone Syndrome and Spasticity: Clinical Management and Neurophysiology (eds M. An Understanding of Functional Movement as a Basis for Clinical Reasoning Linzi Meadows and Jenny Williams Introduction the up to date Bobath Concept relies on a methods model of motor control, the idea of plasticity, principles of motor learning, and an understanding and application of functional human movement. An in-depth understanding of human movement is crucial to the scientific reasoning process.

Diseases
- Spinal-bulbar muscular atrophy
- Transient global amnesia
- Chromosome 18 ring
- Johanson Blizzard syndrome
- Allergic encephalomyelitis
- Multiple pterygium syndrome
- Fetal phenothiazine syndrome
- Micromelic dysplasia dislocation of radius
- Hypercalcemia
- Crow Fukase syndrome
Buy primaquine 7.5 mg without prescription
This is the portion of the ankle joint that carries the physique weight between the leg and foot symptoms lung cancer primaquine 15 mg cheap on line. The sides of the talus are firmly held in place by the articulations with the medial malleolus of the tibia and the lateral malleolus of the fibula treatment quadriceps strain best primaquine 7.5mg, which prevent any side-to-side movement of the talus. The ankle is thus a uniaxial hinge joint that permits only for dorsiflexion and plantar flexion of the foot. Additional joints between the tarsal bones of the posterior foot permit for the actions of foot inversion and eversion. Most necessary for these movements is the subtalar joint, positioned between the talus and calcaneus bones. The joints between the talus and navicular bones and the calcaneus and cuboid bones are also important contributors to these movements. Together, the small motions that take place at these joints all contribute to the manufacturing of inversion and eversion foot motions. Like the hinge joints of the elbow and knee, the talocrural joint of the ankle is supported by a number of strong ligaments positioned on the sides of the joint. These ligaments extend from the medial malleolus of the tibia or lateral malleolus of the fibula and anchor to the talus and calcaneus bones. They also stop abnormal sideto-side and twisting actions of the talus and calcaneus bones during eversion and inversion of the foot. The deltoid ligament supports the ankle joint and also resists extreme eversion of the foot. These embody the anterior talofibular ligament and the posterior talofibular ligament, each of which span between the talus bone and the lateral malleolus of the fibula, and the calcaneofibular ligament, located between the calcaneus bone and fibula. The talocrural (ankle) joint is a uniaxial hinge joint that only permits for dorsiflexion or plantar flexion of the foot. Movements on the subtalar joint, between the talus and calcaneus bones, mixed with motions at different intertarsal joints, enables eversion/inversion movements of the foot. Ligaments that unite the medial or lateral malleolus with the talus and calcaneus bones serve to assist the talocrural joint and to resist extra eversion or inversion of the foot. Lesson eleven: the Lower Limb � Nerves Created by Gabriella Sandberg Introduction Motor nerves arise from the spinal wire to provide innervation to all muscles. All of the spinal nerves embody axons of neurons carrying each sensory info towards the central nervous system and motor info away from the central nervous system. The anatomy and organization of spinal nerves is discussed in detail in Lesson 22. Spinal nerves can continue to instantly form peripheral nerves or axons from completely different spinal nerves could be reorganized to comply with different courses in the periphery. Axon reorganization happens at 4 locations alongside the length of the vertebral column, every identified as a nerve plexus. The lumbar plexus arises from the entire lumbar spinal nerves and offers rise to nerves innervating the pelvic region and the anterior leg. The femoral nerve is doubtless certainly one of the major nerves from this plexus, which provides rise to the saphenous nerve as a department that extends through the anterior decrease leg. The most vital systemic nerve to come from this plexus is the sciatic nerve, which is a combination of the tibial nerve and the fibular nerve. The sciatic nerve extends across the hip joint and is most commonly related to the situation sciatica, which is the results of compression or irritation of the nerve or any of the spinal nerves giving rise to it. The femoral nerve provides innervation to the muscles of the anterior thigh area which includes the hip flexors and the knee extensors. The tibial nerve provides innervation the posterior facet of the calf, as nicely as the lateral and plantar regions of the foot. The superficial fibular nerve supplies innervation the muscular tissues of the lateral facet of the calf, whereas the deep fibular nerve supplies innervation to the anterior facet of the calf. Both fibular nerves provide some innervation to the dorsal area of the foot as properly. The major nerves of the leg embody the femoral, sciatic, obturator, superior and inferior gluteal, deep and superficial fibular, tibial, pudendal, and medial and lateral plantar nerves. By Henry Vandyke Carter - Henry Gray (1918) Anatomy of the Human Body (See "Book" part below) Bartleby. Create your individual schematic of the lumbar and sacral plexuses by drawing every on a clean sheet of paper. Your drawing may be as detailed as you need to, or it can simply be lines exhibiting the delineation between the plexus and nerves. Using colored tape or post-it notes, please write a number that corresponds to the term from the record and place them in your mannequin. Identify and describe skeletal, muscular, and nervous system structures for the lower limb Check your understanding List of terms: 1. Apply your data of the skeletal, muscular, and nervous system structures of the leg to describe a specific example of leg movement. The main bones of the knee embrace the femur, the patella, the tibia, and the fibula to a lesser extent. Without the menisci, a substantial quantity of stress would be positioned to the superior floor of the tibia, in particular. The most necessary ligaments are the anterior cruciate ligament, posterior cruciate ligament, the fibular (lateral) collateral ligament, and the tibial (medial) collateral ligament. The two cruciate ligaments are named as a result of they cross within the knee joint and are named for where they attach on the tibia. The anterior cruciate ligament primarily prevents the tibia from sliding too far anteriorly or rotating too far internally. The tibial collateral ligament is fused to the articular capsule and medial meniscus. Because of this, the tibial collateral is far less versatile than the fibular collateral ligament. Recall that the quadriceps femoris muscle group features primarily to extend and stabilize the knee. All four muscular tissues fuse collectively and pass over the patella to insert on the tibial tuberosity. Image by Mysid - Vectorized and colorized in Inkscape, primarily based on Image:Knee diagram. Since this joint is primarily supported by muscular tissues and ligaments, accidents to any of these buildings can result in pain and/or knee instability. Most commonly, injury occurs when forces are applied to an prolonged knee, significantly when the foot is planted and unable to transfer. Anterior cruciate ligament injuries usually result from a forceful blow to the anterior knee, producing unnatural hyperextension, or when an individual makes a fast change of course that both twists and hyperextends the knee.
Purchase primaquine 15mg without a prescription
At this level medications quizzes for nurses buy primaquine 7.5 mg without a prescription, the posterior sheath is absent and the rectus abdominis muscle is separated from the belly peritoneum solely by a layer of fascia that lines the belly cavity (transversalis fascia) nioxin scalp treatment primaquine 15mg buy generic line. The proper rectus abdominis muscle has been removed in this picture to show the extent of the posterior rectus sheath. It is inferior to this point that only the transversalis fascia separates the rectus abdominis muscle from the peritoneum of the stomach cavity. The rectus sheath accommodates the superior epigastric artery (vein), inferior epigastric artery, decrease intercostal nerves (T7-T11), and subcostal nerve (T12). The superior epigastric artery is a terminal department of the internal thoracic artery that enters the rectus sheath between the sternal and costal portions of the diaphragm and descends posteriorly to the rectus muscle along with the superior epigastric vein. The inferior epigastric artery is a branch of the external iliac artery that runs through the transversalis fascia to attain the rectus sheath on the degree of the arcuate line. The exterior indirect, inner indirect, and transversus abdominis muscular tissues are equipped by intercostal nerves 7-11, the subcostal nerve (T12), and the primary lumbar nerve (L1). The rectus abdominis muscle is provided by intercostal nerves 7-11 and the subcostal nerve. Relaxation of the stomach muscular tissues occurs throughout inspiration to allow downward movement of viscera. Abdominal muscles are contracted to improve intra-abdominal pressure during pressured expiration, micturition, defecation, and parturition. The superior and inferior epigastric veins run alongside their arterial counterparts. Interestingly, the paraumbilical veins drain to the portal vein through the falciform ligament. Superficially, the anterior stomach wall superior to the umbilicus drains to anterior axillary nodes. The deep lymphatic drainage of the anterior abdominal wall follows the deep arteries. The inguinal area (groin) is the realm the place the anterior abdominal wall and thighs meet. During development, the preliminary position of the testes/ovaries is high within the posterior belly wall. The processus vaginalis continues to push outward through several layers: transversalis fascia, inside indirect musculature, and the aponeurosis of the external indirect muscle. As the processus vaginalis continues to push through the stomach wall, the inguinal canal is shaped. The layer of transversalis fascia becomes the deepest layer, whereas the aponeurosis of the exterior indirect muscle stays essentially the most superficial layer. The gubernaculum (directly posterior to the processus vaginalis) pulls the testes by way of the inguinal canal and into the scrotum, while ovaries remain in the pelvic cavity. As the testes move via the inguinal canal, their complement of vessels, nerves, and ducts purchase the same complement of layers as the inguinal canal. In females, the remnant of the gubernaculum (round ligament of the uterus) stays in the inguinal canal. Descent of the gonads is complete upon the obliteration of the processus vaginalis. If it remains patent, a weakening of the belly wall can happen, possibly resulting in a hernia. The canal is a tube shaped during gonad development which spans the region between the deep and superficial inguinal rings. As beforehand described, this ring of the inguinal canal results from an evagination of the transversalis fascia, a contributor to the formation of the interior spermatic fascia in males. The superficial ring of the inguinal canal is found at the decrease finish of the canal. The lateral and medial crura (attaching to the pubic symphysis and pelvic tubercle, respectively) form the edges of the arch. These tendinous crura are joined on the apex of the arch by the intercrural fibers. In males it additionally incorporates the spermatic twine, whereas in females it accommodates the spherical ligament of the uterus. The spermatic twine begins on the deep inguinal ring, runs through the inguinal canal, exits the inguinal canal by way of the superficial inguinal ring, and ends within the scrotum. The three fascia coverings of the spermatic twine are derived from layers of the anterior belly wall. These layers had been acquired throughout development with the descent of the processus vaginalis (now the tunica vaginalis within the scrotum) through the layers of the stomach wall. The cremasteric muscle is innervated by the genital branch of the genitofemoral nerve (L1,2). The exterior spermatic fascia was derived from the exterior indirect aponeurosis and fascia. This table summarizes the relationship between layers of the stomach wall and the fascia of the spermatic wire. Note that not all the layers of the stomach wall contribute to the spermatic twine, i. The vas deferens is the duct responsible for transporting sperm from the epididymis to the ejaculatory duct. The duct begins on the tail of the epididymis and passes up the spermatic wire through the inguinal canal, by way of the deep ring and lateral to the inferior epigastric vessels. A vasectomy is the ligation and chopping of the vas deferens throughout the spermatic twine inferior to the superficial inguinal ring (within the scrotum). It originates from the anterior floor of the abdominal aorta, simply inferior to the origin of the renal arteries. As the testis descends retroperitoneally throughout growth, is carries blood provide with it to the scrotum. The pampiniform plexus is a venous network responsible for draining blood from the testis and epididymis. The veins act to cool the constructions they envelop, such as the vas deferens & testicular artery. These veins permit the contents of the spermatic cord to maintain the cooler temperatures needed for spermatogenesis. The plexus converges at the inguinal canal (one on all sides of body) to form a proper or left testicular vein. This might cause greater pressure within the left renal vein and limit circulate from the left testicular vein, resulting in varicoceles on the left facet. The spermatic cord incorporates arteries, veins, ducts, nerves, and lymphatic vessels. When viewing constructions coming into the posterior aspect of the deep inguinal ring, one can see that the vas deferens and testicular vessels are passing through the spermatic twine. The genitofemoral nerve descends on the anterior floor of the psoas muscle, dividing just above the inguinal ligament into a genital branch (entering the spermatic cord through the deep inguinal ring) and a femoral department (entering the thigh by passing posterior to the inguinal ligament).
Primaquine 15mg purchase amex
Lyme disease is associated with a rash and polyarthropathy and the diagnosis is dependent upon demonstration of antibodies to the spirochaete Borrelia burgdorferi treatment sciatica buy 15 mg primaquine fast delivery. Conclusions Blood exams are useful by way of evaluation symptoms 0f parkinson disease primaquine 7.5mg purchase, prognosis and monitoring in rheumatological ailments. These Standards spotlight the importance of a multidisciplinary approach to the administration of musculoskeletal circumstances; for instance, Standard 10 of this document states that "People with inflammatory arthritis ought to have ongoing access to the local multidisciplinary team, whether or not that is primarily based in secondary care, or locally". The consultant, or one of their medical group, would assess the patient and formulate a treatment plan. Whether or not the patient noticed anyone else in the staff, corresponding to a physiotherapist, depended very a lot on the local services. However, instances have modified, and with this comes an growing recognition of the potential benefits that patients could achieve from a multidisciplinary method to their management. A multidisciplinary approach to administration is subtly different to "shared care", the place therapists and medical doctors from primary and secondary care manage sufferers and share information. Second, clinical-care pathways ought to be developed that, wherever potential, are underpinned by a robust evidence base. Refer urgently if any of the next apply: � the small joints of the hands or feet are affected � a couple of joint is affected � there was a delay of 3 months or longer between onset of signs and looking for medical advice. For care pathways to be translated into effective patient care, all people concerned will must have possession, be concerned in group collaboration and take part actively of their growth and subsequent implementation. However, the precise choices out there will depend on the native service provision. Physiotherapists Physiotherapists are trained within the assessment and management of locomotor and muscular problems. A pivotal a part of their position is educating sufferers about biomechanical dysfunction and actively promoting self-management by way of applicable exercise regimes. Some physiotherapists may undertake extra specialist roles within rheumatology, including administration of flares of inflammatory arthritis, guide remedy or hydrotherapy. Nurse specialists In secondary care, nurse specialists play an necessary position in assessing and managing patients with a variety of rheumatological complaints (Table 25. Nurse specialists typically act as a vital hyperlink between main and secondary care, and between the affected person and specialist providers, through offering telephone helplines or drop-in clinics where patients can obtain advice about acute problems similar to flare-ups. Chiropodists and podiatrists Chiropodists and podiatrists are particularly skilled to assess, diagnose and handle foot- and gait-related pathology. They will assess foot and decrease limb operate, footwear and gait to decide if this is contributing to soft-tissue and joint pathology. Treatment may contain affected person education, prescription footwear, orthoses (custom shoe inserts) or injection remedy. Doctors, allied health professionals, nurses Consultant rheumatologists Consultant rheumatologists are trained to assess and manage sufferers with a variety of musculoskeletal complaints, starting from non-specific back and neck pain to complicated multi-system conditions such as rheumatoid arthritis. Support companies Agencies such as the Arthritis Research Campaign (arc) and Arthritis Care (Table 25. They present an invaluable service, both to patients and to professionals, who can use their assets as a part of their treatment plan. It has not been potential to give attention to every single skilled that could be involved in the advanced care of patients with a rheumatological condition. Development of a competency framework for general practitioners with a particular curiosity in musculoskeletal/rheumatology practice. British Society for Rheumatology and British Health Professionals in Rheumatology guideline for the administration of rheumatoid arthritis (the first 2 years). It is estimated that the proportion of over 65s within the inhabitants will improve 3-fold within the subsequent 30 years, increasing the burden on health-care techniques from musculoskeletal issues. However, estimates are significantly larger in some populations and a prevalence of 6. Some elements improve the risk, whereas others are thought to offer a protective role in illness improvement. A consistent finding is that present or ever use of the oral contraceptive capsule has a protecting function. High intakes of antioxidants (-cryptoxanthin and zeaxanthin) found in some fruit and veggies could scale back the chance. The advantages of following a Mediterranean diet (high proportion of oily fish and vegetables) could confer a protecting function. The site most regularly affected is the knee, though the hip and hand are also generally affected. The heritability of cartilage volume, as a marker of degeneration, has been estimated at over 70%. This may be as a end result of direct cartilage harm or a results of increased stress on the cartilage because of the harm. Other rheumatic diseases the incidence of some of the different rheumatic illnesses seen in rheumatological practice is summarized in Table 26. It is comparatively uncommon in some African and Japanese populations however more frequent in Native Americans, with a prevalence of 6% reported in Haida and Bella Indians. There is an increased danger of the illness in relatives of probands, and results of twin studies show concordance charges of 50�75% in monozygotic twins. Infection could play an element in the illness, however the information are conflicting regardless of several decades of examine. Population research based mostly on self-reported signs estimate shoulder pain prevalence is between 20 and 40%. A recent study estimated that the prevalence of shoulder ache has doubled in males and quadrupled in ladies over the previous 40 years. Risk elements for shoulder ache embrace social class and mechanical and psychosocial elements. Workplace danger components for males growing shoulder ache include carrying weights, damp and cold working environment, working with hands above shoulder stage or stretching under knee degree and utilizing arms or wrists in a repetitive manner. Performing monotonous work has been related to a 3-fold increased risk of shoulder pain in both sexes. A variety of environmental triggers are thought to be threat factors for the illness. Risk elements for hyperuricaemia include obesity, hypertension, alcohol consumption, food plan and some genetic components. Both illnesses increase with age, peaking at around 70 years with a decline after that. Reports suggest that each diseases may be seasonal in incidence, but once more the results have been inconsistent. There are numerous stories that recommend infectious agents as a danger issue for these illnesses, and peak incidences have followed outbreaks of Mycoplasma pneumoniae, human parvovirus B19 and Chlamydia pneumoniae. It is more frequent in ladies than men, with on onset between 35 and 50 years of age. It is noticeably higher in African American, Asian and Afro-Caribbean populations than in white populations. There is strong proof for a genetic cause for the illness, and first-degree family members of patients are at an as much as 9-fold elevated threat of illness improvement. Twin research additionally show a high concordance price, supporting a genetic contribution for the disease.
Primaquine 7.5mg fast delivery
Enzymic action breaks the bond between myosin crossbridges and actin receptor websites medicine dictionary pill identification primaquine 15 mg fast delivery. Myosin crossbridges rejoin different actin receptor sites treatment 0f ovarian cyst buy primaquine 15 mg mastercard, each rejoining drawing the thin filaments closer to the centre of the sarcomere. As each sarcomere shortens the entire muscle fibre contracts Calcium ion is reabsorbed by the sarcoplasmic reticulum. Troponin and tropomysin once more inhibit the interplay of myosin and actin myofilaments, and the muscle fibre relaxes. Anaerobic respiration is in the end limited by depletion of glucose and a construct up of lactic acid within the muscle fibre. Muscle ache that lasts for a couple of days following train, nonetheless, outcomes from harm to connective tissue and muscle fibres inside the muscle. Instead, we cease due to psychological fatigue, the feeling that the muscles have tired. A burst of activity in a drained athlete because of encouragement from spectators is an instance of how psychological fatigue can be overcome. The increased amount of oxygen wanted in chemical reactions to convert lactic acid to glucose is the oxygen debt. Types of muscle contraction Muscle contractions are categorized as either isotonic or isometric. In isotonic contractions, the amount of rigidity produced by the muscle is fixed during contraction, but the size of the muscle adjustments; for instance, motion of the fingers to make fist. Clenching the fist 119 Human Anatomy and Physiology more durable and harder is an instance. For instance, when shaking hands, the muscular tissues shorten some distance (isotonic contractions) and the degree of pressure increases (isometric contractions). Isometric contractions are also liable for muscle tone, the constant tension produced by muscle tissue of the body for long durations. Muscle tone is answerable for posture; for example, maintaining the back and legs straight, the top held in upright position, and the abdomen from bulging. Muscle attachments Most muscular tissues prolong from one bone to another and cross no much less than one movable joint. Muscle contraction causes most physique actions by pulling one of many bones towards the other throughout the movable joint. For instance, some facial muscles connect to the pores and skin, which moves as the muscle tissue contract. The origin is essentially the most stationary end of the muscle and the insertion is the top of the muscle connected to the bone present process the greatest motion. Some muscle tissue have more than one origin, but the principle is the same-the origin act to anchor or 121 Human Anatomy and Physiology hold the muscle so that the pressure of contraction causes the insertion to move. For example, the biceps brachii causes the radius to transfer, resulting in flexion of the forearm. The triceps brachii muscle has three origins; two on the humerus and one on the scapula. The insertion of the triceps brachii is on the ulna and contraction ends in extension of the forearm. Of all the muscles contracting concurrently, the one mainly answerable for producing a particular movement is recognized as the prime mover for that motion. As prime movers and synergist muscles at a joint contract, different muscular tissues referred to as antagonists, loosen up. When those antagonist muscular tissues contract, they produce a movement opposite to that of these prime movers and their synergist muscular tissues. Naming skeletal muscle tissue Most of the skeletal muscles are named according to a number of of the following basis: 1. Direction of muscle fibres relative to the midline of the physique or longitudinal axis of a construction Rectus means the fibres run parallel to the midline of the physique or longitudinal axis of a construction. Example, rectus abdominis 122 Human Anatomy and Physiology Transverse means the fibres run perpendicular to the midline longitudinal axis of a structure. Example, transverse abdominis Oblique means the fibres run diagonally to the midline longitudinal axis of a structure. Location-structure to which a muscle is discovered intently related Example: Frontal, a muscle near the frontal bone Tibialis anterior, a muscle close to the front of tibia 3. Origin and insertion-sites where muscles originates and inserts 123 Human Anatomy and Physiology Example, sternocleidomastoid-originates on sternum and clavicle and inserts on mastoid process of temporal bone. Example, depressor labii inferioris Supinator: turns the palm upward or anteriorly. Example, obturator externus Example, Example, 124 Human Anatomy and Physiology Principal skeletal muscle tissue Although there are over 700 individual skeletal muscle tissue within the human body, an appreciation and understanding of skeletal muscle tissue may be accomplished by concentrating on the massive superficial muscular tissues and muscle groups. Table 6-1 via Table 6-4 summarizes the origin, insertion, and action of those muscle tissue. Head and neck muscular tissues Muscle Origin Insertion Action Muscles of facial features Occipitofrontalis orbicularis oculi Orbicularis oris Buccinator Zygomaticus muscles Levator labii superioris Corrugator supercilli Depressor anguli oris Mandible Lower lip close to nook of mouth Frontal bone Skin of eye forehead Lowers and draws collectively eye brows Depresses corner of the mouth Maxilla Upper lip Occipital bone Maxilla & frontal Maxilla & mandible Mandible & maxilla Zygomatic bone Corner of mouth Elevates corner of mouth Elevates higher lip Skin of eye brow Skin around the eye Skin across the lips Corner of mouth Flattens cheeks Closes lip Elevates eye brows Closes eye 125 Human Anatomy and Physiology Muscles of mastication Temporalis Massetor Muscles rapezius Sternocleidomas toid that Temporal region on facet of the cranium Zygomatich arch Occipital and vertebrae Sternum clavicle & bone Mandible Closes jaw Mandible Scapula and Clavicle Closes jaw Extends head and neck transfer the head Mastoid process of temporal bone Rotates head and flexes neck Table 6-2. Trunk muscles Muscle Origin Insertion Action Muscles that transfer the vertebral column Erector spinae Deep muscles Rectus abdominis External belly indirect Internal belly oblique Transversus abdominis Ribcage, vertebrae and iliac crest Iliac crest and vertebrae Rib cage Pubis Xiphoid strategy of sternum & lower ribs Iliac crest & facia of rectus abdominis Lower facia of rectus abdominis Xiphoid strategy of sternum, facia of rectus, abdominis pubis and ribs and Flexes vertebral Flexes vertebral & & rotates column; rotates column; back Ilium, sacrum, Superior vertebrae Ribs Vertebrae Extend, abduct, and rotate vertebrae Extend, abduct, and rotate vertebrae Flexes vertebrae; compress stomach vertebrae Vertebrae compress abdomen compress stomach Compress abdomen 126 Human Anatomy and Physiology Table 6-3. Upper limb muscles Muscle Origin Insertion Action Muscles that move the scapula Trapezius Serratus anterior Occipital bone and vertebrae Ribs Scapula clavicle Medial border of the scapula holds scapula in place rotates scapula Rotates scapula and pulls anteriorly Muscles that move the arm Pectoralis main Lattismus dorsi Deltoid Sternum, and clavicle Vertebrae Scapula clavicle Scapula Scapula and ribs, Tubercle humerus Tubercle humerus Shaft humerus Tubercle humerus Tubercle humerus of Adducts arm and flexes of of Adducts and extends arm Abducts, flexes, and extends arm Adducts and extends arm Extends arm Teres main Infraspinalis of of Muscles that transfer the forearm Brachilis Shaft of humerus Coracoids process of ulna Radial tuberosity Flexes and forearm Biceps brachii Coracoids means of Supinates scapula Shaft of humerus and lateral border of scapula Triceps brachii Olecranon strategy of ulna Extends forearm Muscles that transfer the wrist and fingers 127 Human Anatomy and Physiology Anterior arm muscular tissues Posterior forearm muscles Intrinsic muscle tissue fore Medial epicondyle Lateral epicondyle Carpals,metacar buddies, and phalanges Carpals,metacar pals, and phalanges Phalanges Flex wrist, fingers and thumb; pronate forearm Extend wrist, fingers and thumb; supinate forearm Abduct, adduct, flex, and extend fingers and thumb hand Carpals metacarpals Table 6-4. Define fascia, muscle bundle, muscle fibre, myofibril, myofilament, and sarcomere. Name and describe the main actions and innervations of the principal muscle tissue of the head and neck, upper extremities, trunk, and lower extremities. List the components of a reflex arc List the divisions of the nervous system Identify the main anatomical elements of the mind and spinal twine and briefly comment within the operate of every. Discuss spinal and cranial nerves 133 Human Anatomy and Physiology - Discuss the anatomical and practical traits of the two divisions of the autonomic nervous system Classify sense organs as particular or basic and clarify the fundamental variations between the 2 teams. Selected Key Terms the next phrases are defined within the glossary: Accommodation Acetylcholine Action potential Afferent Autonomic nervous system Axon Brain stem Cerebellum Midbrain Nerve Nerve impulse Neucleus Neuron Neurotransmitter Ossicle Plexus 134 Human Anatomy and Physiology Cerebral cortex Cerebrum Choroid Cochlea Conjunctiva Cornea Dendrite Diencephalons Effector Efferent Epinephrine Ganglion Gray matter Hypothalamus Lacrimal Medulla oblongata Meninges Pons Proprioceptor Receptor Reflex Refraction Retina Sclera Semicircular canal Spinal wire Stimulus Synapse Thalamus Tract Tympanic membrane Ventricle Vestibule White matter General Function None of the physique system is able to functioning alone. All are interdependent and work collectively as one unit so that ordinary circumstances within the body might prevail. Both techniques transmit data from a hundred thirty five Human Anatomy and Physiology one part of the physique to one other, however they do it in several ways. The nervous system transmits data very rapidly by nerve impulses carried out from one physique area to one other. The endocrine system transmits data extra slowly by chemical compounds secreted by ductless glands into blood steam and circulated from glands to different elements of the physique. Conditions each inside and outdoors the physique are constantly changing; the aim of the nervous system is to respond to these internal and external modifications (known as stimuli) and so trigger the body to adapt to new circumstances. The nervous system has been compared to a phone change, in that the brain and the spinal twine act as switching centres and the nerve trunks act as cables for carrying messages to and from these centres.