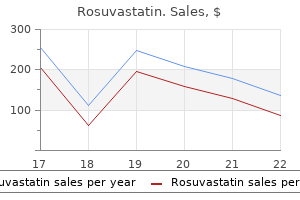
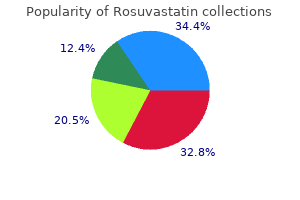
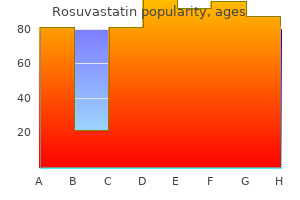
Rosuvastatin
Rosuvastatin dosages: 10 mg
Rosuvastatin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Order rosuvastatin 10 mg with mastercard
Electrosurgical techniques similar to cholesterol za wysoki dieta buy 10 mg rosuvastatin with amex these used in the bladder have been utilized for small distal ureteral neoplasms cholesterol levels for adults discount rosuvastatin 10 mg with mastercard. Historically, resection was the primary to be used for therapy of higher tract neoplasms [58, 59]. Rigid ureteral resectoscopes, just like a long model of a pediatric resectoscope, can be used in a similar way to different resection procedures for tumors within the distal ureter. The loop takes a small chunk of tissue and it might become essential to clear the loop earlier than eradicating the next piece of tissue. Extreme care must be taken to avoid resecting through the complete thickness of the ureteral or renal pelvic wall, and in addition to avoid fulgurating a large area of the ureter, which may end up in scarring and stricture formation [60]. Chapter 41 Ureteroscopic Diagnosis and Treatment of Upper Urinary Tract Neoplasms 443 laser can penetrate to a depth of approximately 5�6 mm, it may not have an effect on the whole depth of the tumor. Coagulated tissue is eliminated with a grasper or basket to expose portions of the tumor in any other case not visible ureteroscopically. It is a solid-state pulsed laser that may fragment calculi, and coagulate, ablate, and remove tissue. This laser produces light at a wavelength of 2100 nm, which can be carried alongside low water content fiber. This laser is especially useful for ureteral lesions since it can ablate and remove a visually occlusive neoplasm to open the lumen for inspection extra proximally [65�67] (see Video 41. The laser fiber must be positioned involved with or very close to the tissue to be treated. It is often necessary to discontinue treatment to allow the field to clear, since considerable debris is shaped throughout treatment. Bleeding occurs often and can be controlled better at decrease energies or by shifting the fiber barely away from the tissue to diffuse the laser beam and improve coagulation. There can also be clinical proof that a longer pulse duration, similar to seven hundred ms, somewhat than the 350 ms usually used for lithotripsy, may even enhance coagulation (see Video forty one. The very limited penetration allows precise control and the laser, thus, can be used for lesions positioned on the stage of the iliac vessels and the renal pelvis near the renal vessels. Great care is employed to keep away from ablation and resection through the wall of the ureter or renal pelvis itself. The argon laser has major theoretical benefits for endoscopic treatment as well. Wavelengths of 488� 514 nm have been used to deal with superficial bladder cancer and also ureteral neoplasms. The penetration is limited to 1 mm and the laser gentle may be delivered with a fiber of 300 or 600 m diameter. Johnson reported treating tumors with continuous wave argon laser energy with a quartz fiber, utilizing a contact mode with the power set at 5 W [68]. There was passable ablation of tumors in all three sufferers, but other confirmatory reviews are still not out there. The strategies used for therapy, the location and characteristics of the tumors, and follow-up methods and length have varied widely. There have been asynchronous recurrences in three patients which remained low grade and no affected person required surgical therapy during the examine interval. Several bigger collection since these earlier reviews have expanded the acceptable limits of remedy, including larger proximal lesions, and a few have included larger grade tumors. Overall, this has resulted in a relatively high recurrence price with a wide variation and an growing need for nephroureterectomy, however secure development of recent bladder tumors [70�81]. Successful remedy depends upon thorough remedy of the primary neoplasm without irreversible injury to the organ system, coupled with the dearth of local recurrence of the neoplasm as properly as a scarcity of metastases. Chapter 41 Ureteroscopic Diagnosis and Treatment of Upper Urinary Tract Neoplasms 445 local recurrence. As noted above, the recurrence for ureteral lesions is approximately 12�18% and higher when more proximal lesions had been eliminated. Renal pelvic lesions handled surgically recur at a fair larger price of 48�66% [49, 50, 79]. In collected series reporting ureteroscopic treatment of upper tract tumors through the early experience by way of 1995, there was a better recurrence fee for renal pelvic lesions (40%) than ureteral lesions (25%). However, throughout the next 5 years, there was a rise in the recurrence of ureteral tumors (43%) with renal pelvic tumors stable at 37%. Thus, it might be speculated that the distinction is related to the ureteroscopic treatment of larger and extra proximal ureteral lesions in the later years. We have found that many of the recurrent lesions are small and may be treated endoscopically. Only when there are extensive and fast recurrences does nephroureterectomy become necessary (Table forty one. These series are also characterised by excessive diseasespecific survival, with the two notable exceptions of the series reported from the Mayo Clinic of sufferers presenting initially with bladder tumors, and in those in whom crucial indications such as a solitary kidney prompted their endoscopic remedy. It is notable that in most of the sufferers, biopsy affirmation was not available and high-grade recurrences developed [86, 88, 89]. Some of those characteristics are similar for to these for threat of recurrence for bladder tumors. There can be a better danger of recurrence for high-grade tumors treated either ureteroscopically or by open surgery. There is proof that positive urinary cytology at the time of therapy is a poor prognostic signal. The impact of the situation of the first tumor, whether within the intrarenal collecting system or ureter, has been inconsistent, with some series reporting the next price for intrarenal neoplasms and others discovering no difference or extra frequent recurrence after ureteral primaries. However, multifocal lesions have constantly been seen to be associated with more frequent recurrences, both within the higher tract and within the bladder. Tumor location Bladder tumors There is critical threat of new bladder tumors growing in patients with higher tract neoplasms. In a abstract of several series reporting laparoscopic and open neph- roureterectomy, the subsequent bladder tumor fee was 31. However, there was a variety in each group: 10�55% within the laparoscopic group and 15�45% within the open surgical group [90]. Additionally, one collection in contrast bladder recurrences after retroperitoneoscopic or open nephroureterectomy with out finding any difference [91]. Among sufferers with higher tract tumors treated ureteroscopically, the common subsequent bladder tumor prevalence price was 38. In two series of patients without previous bladder tumors, the rate was 34% and 33%, respectively (Table 41. Some series have noted that the bladder tumor price is expounded to the grade of the primary tumor, while the effect of grade was not thought of in others. One report 446 Section 3 Ureteroscopy: General Principles high-grade higher tract neoplasm. There is a few evidence that high-grade lesions will recur more regularly, however long-term successes have additionally been reported [77].
Syndromes
- Cutting the bone and changing its alignment to relieve stress on the bone or joint (osteotomy)
- You have a family history of heart disease
- May appear in the nose and mouth
- Rapid pulse
- North-central states, mostly in Wisconsin and Minnesota
- Head MRI scan
- Brain biopsy
Buy 10 mg rosuvastatin
The contrasting char acteristics of acute kidney harm in developed and creating coun tries cholesterol levels for heart disease rosuvastatin 10 mg buy cheap on line. Continuous hemofiltration supplies smoother control of ultrafiltered quantity and gradual correction of metabolic abnormalities in unstable patients cholesterol ratio and risk buy cheap rosuvastatin 10 mg on-line. These therapies are helpful when large amount of fluids have to be eliminated in sick and unstable patients. If interstitial nephritis is suspected, the offending agent ought to be withdrawn and oral corticosteroids given. The outlook is satisfactory in acute tubular necrosis without complicating factors. Other elements related to poor outcome include delayed referral, presence of complicating infections and cardiac, hepatic or respiratory failure. Maintenance of vitamin and prevention of infections is extraordinarily crucial in enhancing outcome. Renal failure may sometimes be the first manifestation of a congenital anomaly of the urinary tract. Symptoms of renal failure could also be insidious, together with lethargy, puffiness and a few decline in urine output. Renal vein thormobosis is suspected in at-risk neonates with hematuria, enlarging flank mass, thrombocytopenia and azotemia. Features suggestive of urinary tract obstruction embody an abdominal mass, hypertension and oligoanuria. Serum creatinine levels are high at birth (reflecting maternal levels) and reduce to below 0. Failure of discount or rise of serum creatinine indicates impaired renal operate. Sudden distention of peritoneal cavity might cause respiratory embarrassment or apnea. Since chiefly shigatoxins 1 and a pair of are implicated, the sickness can also be called shigatoxin E. The microangiopathic lesions mainly affect interlobular arteries and result in severe hypertension and progressive renal insufficiency. Defective cobalamin metabolism leads to a extreme form presenting in early infancy. Following a prodrome of acute diarrhea or dysentery, sufferers present sudden onset of pallor and oliguria. The capillary lumen is narrowed by swollen endothelial cells, blood cells and fibrin thrombi. A variety of medicine are dialyzable and applicable amounts should be added to supplement for their losses. The consequence is expounded to the underlying condition unless the renal failure is prolonged beyond a few days. They are characterized by microangiopathic hemolytic anemia, thrombocytopenia and acute renal insufficiency. Cytotoxin mediated injury to endothelium within the renal microvasculature leads to localized coagulation and fibrin deposition. A classification of hemolytic uremic syndrome and thrombotic thrombocytopenic purpura and related problems. Peritoneal or hemodialysis could also be essential to forestall compli cations of renal insufficiency. Plasma exchanges are initiated as early as possible, performed day by day until hematological remission, and then much less regularly. Patients with anti-factor H antibodies benefit from immunosuppression with brokers that cut back antibody production. Factors suggestive of poor consequence embrace oligoanuria for greater than 2 weeks, extreme neurological involvement and presence of cortical necrosis. At the initial stages, administration aims at sustaining nutrition and retarding development of the renal failure. Later, remedy of issues and renal replacement remedy in the type of dialysis or transplantation is required. Loss of urinary concentrating capacity ends in frequent passage of urine, nocturia and elevated thirst. Resistance to the action of development hormone, the degrees of that are increased, is considered to be responsible for progress failure. Abnormalities in metabolism of calcium and phosphate and bone illness outcomes from hyperphosphatemia, lack of renal formation of 1, 25-dihydroxyvitamin 03, deficiency of calcium, chronic acidosis and secondary hyperparathyroidism. The blood pressure could additionally be elevated and optic fundi present hypertensive retinopathy. Severe proximal muscle weak point, peripheral neuropathy, itching, purpura and pericarditis are late options. Investigations Treatment of Reversible Renal Dysfunction Common circumstances with potentially recoverable kidney operate embody an obstruction in the drainage, recurrent urinary tract infections with vesicoureteric reflux and decreased renal perfusion as a end result of renal arterial stenosis. Retarding Progression of Renal Failure Hypertension and proteinuria result in elevated intra glomerular perfusion, adaptive hyperfiltration and pro gressive renal damage. Longterm remedy with angiotensin converting enzyme inhibitors has been proven to scale back proteinuria and may retard development of renal failure. The affected person should be investigated to find the reason for renal failure and detect reversible factors. Blood counts and ranges of urea, creatinine, electrolytes, pH, bicarbonate, calcium, phosphate, alkaline phos phatase, parathormone, protein and albumin are obtained. Blood ranges of ferritin and transferrin saturation are obtained in patients with anemia. A food plan excessive in polyunsaturated fat, such as corn oil and medium chain triglycerides and complex carbohydrates is most popular. Excessive use of diuretics, overzealous restriction of salt and gastroenteritis might lead to dehydration that ought to be corrected. Blood must be transfused slowly, since it might aggravate hypertension and coronary heart failure. Urinary tract and different infections ought to be promptly treated with effective and least poisonous drugs. Optimization of caloric and protein intake and remedy of mineral bone disease is necessary. Administration of recombinant human progress hormone improves growth velocity in youngsters with persistent renal failure. Early recognition and management of malnutrition, mineral bone illness, metabolic acidosis and electrolyte disturbances ought to take priority over the establishment of therapy with development hormone. Mineral bone disease is a significant issue in children because it happens in the course of the period of lively development. Some infants are polyuric and lose large amounts of sodium requiring salt supplementation.
10 mg rosuvastatin trusted
Ureteroscopy beneath spinal versus general anaesthesia: morbidity and stone clearance cholesterol foods that are good rosuvastatin 10 mg buy generic on-line. American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery); Fleisher cholesterol medication lawsuit rosuvastatin 10 mg order otc, L. Executive abstract: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Ureteroscopic lithotripsy beneath local anesthesia: analysis of the effectiveness and patient tolerability. Ureteroscopy as an out-patient process: the Singapore General Hospital Urology Centre experience. Percutanous nephrolithotomy under general versus combined spinalepidural anesthesia. Impact of physique mass index on price and clinical outcomes after percutaneous nephrostolithotomy. Lung air flow and perfusion in inclined and supine postures close to anesthetized and mechanically ventilated wholesome volunteers. Blood utilisation in elective general surgery circumstances: requirements, ordering and transfusion practices. American Society of Anesthesiologists Task Force on Preanesthesia Evaluation: Practice advisory for preanesthesia evaluation: a report by the American Society of Anesthesiologists Task Force on Preanesthesia Evaluation. Preoperative laboratory screening in wholesome Mayo patients: cost-effective elimination of exams and unchanged outcomes. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. Comparative results of extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy. Complications of extracorporeal shock wave lithotripsy and percutaneous nephrolithotomy. Urolithiasis in patients with spinal wire accidents: threat components, management, and outcomes. College of Cardiology/American Heart Association Task Force on Practice Guidelines. Preoperative pulmonary analysis: figuring out and reducing dangers for pulmonary issues. A combined "civil� mechanical�electrical�electronic�biomedical" mixed effort is required, coordinated by the needs, preferences, and safety of the medical/surgical group. Apart from the shortage of sensible publications and particulars in this area, the highly technical nature of many of the issues, and the issue of speaking them, typically result in mistakes in planning being made at a quite simple level. It is necessary that planning is ideal, keeping in mind future needs, as subsequent adjustments or renovations are tedious and pose super economic burden [1]. Most surgical meetings at present commit a significant session to the stay operative workshop. The other drawback is economic restriction, particularly in semi-government aided or personal hospitals. The state-of-the art design enables hasslefree motion of kit, surgeon ease in viewing a number of screens, and environment friendly information archival, management, and relay system. It is critical to anticipate the average variety of procedures that will be carried out. Meeting these challenges requires a multidisciplinary group and a well-planned process that addresses all elements from long-term targets to exacting particulars. The inside air supply area stays free from contaminants drawn in from the room setting. In this fashion the area around the operating desk is stored in a high state of cleanliness through the operation, with an especially low pathogen level of lower than 10 colonyforming units/m3. The sterile air distributors could be easily indifferent or swung away for fast and financial filter modifications. Architect, engineer, tools planner, construction manager, and key tools distributors should all be included in the team [2]. Strategic equipment placement is crucial to improve efficiency and security inside the surgical space. The booms, which might move in each course, considerably reduce muddle and interconnect tools, releasing ground house and simplifying cleaning. They make the most of the house above the false ceiling, thereby enhancing sterile set-up and lowering upkeep as a result of cable breakage. Booms, however, require a major quantity of structural support, which have to be coordinated with the lighting, mechanical, and electrical techniques above the false ceiling. Pendant providers Two ceiling pendants for pipeline companies must be designed; one for the surgical group and one for the anesthesiologist. The anesthetic pendant ought to be retractable, have limited lateral motion, and supply a shelf for monitoring gear. It should have oxygen, nitrous oxide, four bar strain medical compressed air, medical vacuum, scavenging terminal shops, and a minimum of four electric sockets. Moreover, some carts even have room to hold the laparoscopic insufflator and electrocautery models. The ground should have a slight tilt from all the partitions, converging on the water drain outlet. The floor surface have to be slip resistant, strong, and impervious, with minimal joints. Individual cassettes made from painted sheet steel are clipped in to the grid to form a suspended metal ceiling. The individual cassettes may be removed and reinstalled to allow maintenance and refitting work. This space contains: � Cables for varied a number of equipment booms, corresponding to oxygen, nitrous oxide, compressed air, vacuum, electrical wires. The ceiling air provide with the sterile air distributor is probably considered one of the most necessary elements for hygiene in the working room. Bacteria, viruses, and dust particles are trapped instantly before the air enters the room. The sterile air distributor generates a homogenous and low-turbulence displace- Walls the radiation protection of a general-purpose fluoroscopy suite necessitates a wall thickness in all directions equal to 2 mm of lead (15 cm of concrete or 25 cm of brick with plaster). As for the floor, the floor of the partitions have to be slip resistant, robust, and impervious, with minimum joints. Laminated polyester or easy paint provides a seamless wall surface; tiles can break and epoxy paint can chip. There ought to be provision for an X-ray movie illuminator, wall-mounted digicam, plasma display screen, and drawers for endoscopic disposables, recessed in to the wall. The data output from the C-arm may be related to one of the hanging screen displays so as to be in easy view of the working surgeon. Colorcorrected fluorescent lamps are preferred to produce even illumination of no less than 500 Lux at working top, with minimal glare. Lights should be freely movable both in the horizontal and vertical planes, and for this motion equipment booms are typically preferred. Sterilization (see additionally Chapter 1) There must be a separate room for cleaning and disinfection of endoscopic devices, which should have enough air flow to exhaust toxic vapors and airborne pathogens.
Buy 10 mg rosuvastatin fast delivery
Certain ethnic groups are inclined to lowering cholesterol without medication uk generic rosuvastatin 10 mg have smaller or bigger infants cholesterol medication and kidney disease cheap 10 mg rosuvastatin mastercard, and male fetuses are usually bigger than females. The manufacturing of lecithin is elevated by cortisol and other factors that stress the fetus. Diabetes delays lecithin manufacturing and leaves the infant of the diabetic mother at larger threat of respiratory misery syndrome. The liver, pancreas and gall bladder are all out-pouchings of the endoderm that varieties the fetal gut. Fetal anaemia is related to a hyperdynamic circulation, whereas fetal hypoxaemia is associated with redistribution of blood flow. Fetal structural defects are typically obvious at 18�22/40 as morphogenesis is generally complete. The measurement of serum alpha-fetoprotein is a screening test for neural tube defects rather than a diagnostic take a look at. Chorionic villus sampling has the next rate of being pregnant loss than amniocentesis, though both are low in experienced hands. The aetiology is multi-factorial, with well-defined environmental, genetic, pharmacological and geographical elements implicated. Pre-conceptual folate supplementation of the maternal food regimen reduces the chance of growing these defects by about half. Talipes is associated with oligohydramnios due to the decreased intrauterine area. Fetal neuromuscular circumstances interfere with swallowing and subsequently are associated with polyhydramnios. Intrapartum complications are extra frequent with the second twin than with the primary. Spontaneous preterm labour is always a danger in twin being pregnant, where the typical gestation is 37 rather than 40 weeks. Internal podalic model could also be a helpful technique for delivery of the second twin, however would be inappropriate for the primary. The elevated distension of the uterus throughout twin pregnancy gives a greater probability of postpartum haemorrhage and a prophylactic syntocinon infusion is often given postpartum. However, this risk is excessive approaching time period with monoamniotic monochorionic twins. Monzygotic twins may be either di- or monochorionic, depending on when splitting of the conceptus occurs. Monochorionic twins have a 15 per cent likelihood of developing twin-to-twin transfusion syndrome and ought to be followed with repeated growth scans in the third trimester. Multi-fetal discount must be carried out round 11�12 weeks to account for pure pregnancy loss. Although it reduces the probabilities of extreme preterm delivery, multi-fetal discount increases the possibility of pregnancy loss earlier than viability. In regular pregnancy, the impact of invasion of the trophoblast in to the spiral arterioles is to convert them in to large-bore, low-resistance, large-capacitance vessels. The placenta is responsible for manufacturing of a number of hormones throughout being pregnant, together with human placental lactogen. The placenta is split in to cotyledons, every of which accommodates a primary stem villus. Multiple being pregnant is also a risk factor, probably linked to the larger placental space. Labetalol is helpful in lowering maternal blood pressure, and magnesium sulphate is used primarily for seizure prophylaxis. Antiphospholipid syndrome and fetal karyotype abnormalities are each threat components. Increased perinatal mortality and intra uterine dying are as a consequence of reduced placental perfusion and fetal hypoxia, rather than fetal blood loss. The cervix ought to be evaluated with a sterile speculum examination somewhat than a digital examination to reduce the danger of introducing infection. This ought to ideally be performed after the mom has been supine for some time to help establish amniotic fluid pooling in the speculum. Courses acquired lower than 48 hours or greater than 7 days from supply are nonetheless of benefit. Antenatal steroids can be given on the suspicion of preterm labour, however care must be taken with multiple doses. Nifedipine can be utilized to arrest preterm delivery as it acts to inhibit intracellular calcium release. Atosiban is a particular oxytocin receptor antagonist and subsequently reduces uterine contractions. Labetalol is an alpha- and beta-receptor antagonist used within the discount of blood strain. Any girl delivering after preterm rupture of the fetal membranes is susceptible to postpartum haemorrhage and endometritis. The problems with mitral stenosis in being pregnant stem from the shortcoming of the stenotic valve to address the rise in cardiac output that being pregnant calls for. Maternal mortality is reported at around 2 per cent and adverse fetal end result is immediately related to the severity of the stenosis. The couple ought to be offered genetic counselling relating to the danger of the fetus having cystic fibrosis or being a service. Pancreatic perform is affected in ladies with cystic fibrosis and eight per cent will develop gestational diabetes in being pregnant. Ideally, vaginal delivery ought to be the aim; nonetheless, the second stage may be shortened within the event of maternal exhaustion. Nutritional status impacts the iron stores, and repeated being pregnant and poor social components might result in anaemia, as will the increased iron necessities of multiple being pregnant. Blood transfusion should be averted, if potential, because of the small risk of antibody manufacturing and transfusion reaction. This is because vitamin K-dependent clotting components throughout the new child may be reduced and result in haemorrhagic disease. Although magnesium sulphate is the therapy of choice for an undiagnosed seizure throughout labour, intravenous benzodiazepines. These embrace hepatosplenomegaly, microcephaly, intrauterine growth retardation, hyperbilirubinaemia, intracerebral calcification and mental retardation. In the third trimester, 75�90 per cent of infections are transmitted, but the risk of fetal harm is type of zero at time period. Fetal varicella syndrome occurs in a minority of contaminated fetuses (approximately 1 per cent). No case of fetal varicella syndrome has been reported when maternal infection has occurred after 28 weeks.
Rosuvastatin 10 mg trusted
A combined antegrade and retrograde endoscopic strategy for the management of urinary diversion-associated pathology cholesterol score of 5.1 rosuvastatin 10 mg with visa. Preoperative analysis A thorough historical past and physical examination ought to be carried out preoperatively cholesterol level in fish eggs rosuvastatin 10 mg generic on line. History details that will illuminate an increased risk of inauspicious access should be elicited. Advance knowledge of those risk components permits for preoperative planning in addition to acceptable counseling of sufferers concerning risks and the potential for failed access. History of benign prostatic hyperplasia and/or bladder outlet obstruction must be elicited. A large occlusive prostate might impede bladder access and, if friable, may impair visualization secondary to bleeding. A massive intravesical median lobe may obscure visualization of 1 or each ureteral orifices. Chronic bladder outlet obstruction can also cause bladder trabeculations or diverticula, which may distort intravesical anatomy and hinder the identification of the orifices. A history of pelvic or retroperitoneal radiation, or of trauma, may improve the likelihood of scar tissue formation, leading to tissue or anatomic distortion. Abdominal aortic aneurysms ought to be famous as they could cause extrinsic compression of the ureter and/or deviation. Patients with retroperitoneal fibrosis, which can be secondary to quite a few processes. Prior open or endoscopic interventions may increase the risk of ureteral stricture illness and thus hinder access. Prior surgical procedure may alter anatomy, together with ureteral reimplantation with neoureterocystotomy. Reimplantation can also convey risk of vesicoureteral anastomotic stricture or reflux. Review of prior operative stories could information access concerning location of the new orifice. Other pertinent details of the patient history include use of anticoagulants or antiplatelet agents. There is proof that ureteroscopic interventions in sufferers taking these agents are protected, significantly within the administration of stone illness [1]. Another essential detail of the history is whether a affected person demonstrates signs or symptoms of urinary tract infection, or danger elements for colonization of the urinary tract. Those with colonization ought to be positioned on culture-specific antibiotics previous to surgery to reduce risk of urosepsis with instrumentation. Patients should be knowledgeable of the risk of failed entry and the attainable want for ureteral stent placement with abortion of the process and/or percutaneous nephrostomy tube placement. The more completely sufferers are endorsed preoperatively, the higher belief will persist postoperatively if these conditions occur, and subsequent counseling of the patient will be facilitated. Standard access Rigid cystoscope (30 and 70o lens) with light twine, digital camera, and irrigation fluid (Albarran bridge if desired) Nitinol guidewires: 0. The steps of the process ought to be anticipated and the scrub desk organized to ensure a easy succession of occasions. Additional tools for tough access circumstances may be required at the discretion of the surgeon (Table 37. If entry fails, the affected person could require a percutaneous approach or nephrostomy tube, which could be positioned by the urologist or interventional radiologist. Balloon dilators are helpful for accessing anatomically tight or strictured segments of ureter. Dimensions of balloon dilators range by manufacturer; we sometimes use 4-, 6- or 10-cm dilators with 12�15F balloons inflated to 12 atm. Dimensions of available commonplace ureteral balloon dilators include balloon lengths of 4�10 cm, inflated balloon diameters of 12�18F (4�6 mm), and dilation pressures as much as 30 atm. Fluoroscopy (C-arm or table) is required to information positioning of wires, catheters, and ureteral entry sheaths, and to allow retrograde pyelography. Placement of the versatile ureteroscope may be carried out with fluoroscopic steering over the working guidewire up to the extent of disease. Fluoroscopy can additionally be useful for identification of radioopaque stones and following the fragmentation of a stone throughout laser lithotripsy. The surgeon should confirm that fluoroscopy is appropriately positioned and may be simply manipulated previous to surgery. When advancing the wire in to the orifice, it may be very important ensure the end of the cystoscope sits instantly on the orifice to forestall buckling or curling of the wire in the bladder. Methods of addressing an lack of ability to advance the preliminary wire are mentioned beneath. With the first wire in the appropriate place, the bladder is emptied through the cystoscope (side port or sheath) to maximize the chance of successful passage of a catheter and/or ureteroscope through the intramural ureter. At this time, we suggest placement of a Standard retrograde entry for flexible ureteroscopy Depending on institutional protocol, the surgical website. The kind of anesthesia will rely upon an in depth dialog between the anesthesiologist, surgeon, and affected person, and could also be influenced by numerous factors. The patient is positioned in the dorsal lithotomy place, and prepped and draped in commonplace sterile trend. A single dose of prophylactic antibiotic is administered previous to the procedure if the preoperative urine culture is unfavorable. If the affected person has a positive preoperative urine culture, they want to be handled with a full course of culture-specific antibiotics previous to intervention. Alternatively, deep venous thrombosis prophylaxis may be given with subcutaneous heparin or low molecular weight heparin. After cystoscopic analysis of the bladder, the relevant ureteral orifice is recognized and cannulated with a guidewire. The guidewire may advance via the top of the rigid cystoscope immediately in to the orifice, or a 5F open-ended catheter may be required to present the proper angle for intubation of the orifice. Intravenous furosemide can be concomitantly administered to expedite excretion from the kidneys. A flexible cystoscope can additionally be utilized to determine the orifice beneath the lobe and in sufferers with a really high using bladder neck, which prohibits bladder entry with a rigid scope. Accessing the orifices with flexible cystoscopy could be technically challenging as irrigant move and visibility are inferior to those with a inflexible scope, and reaching the right angle for entry of the orifice could also be difficult. Additionally, the utilization of an Albarran deflecting bridge or an angled-tip angiographic catheter. Preoperative imaging could be helpful in delineating higher tract anatomy, including ectopic ureters; urographic imaging is particularly helpful. Review of prior operative stories may present steering regarding location of ureteral orifices after ureteral reimplantation. A safety wire allows for ureteral stent placement at any time ought to there be iatrogenic damage or an lack of ability to proceed. It may also stop loss of access to the higher urinary tract during the surgery. A retrograde pyelogram can be performed through the dual-lumen catheter prior to second wire placement if it has not been performed earlier.
Alstonia Bark (Fever Bark). Rosuvastatin.
- What is Fever Bark?
- Dosing considerations for Fever Bark.
- Fever, hypertension, diarrhea, malaria, and arthritis-like pain (rheumatism).
- Are there safety concerns?
- Are there any interactions with medications?
- How does Fever Bark work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96452
10 mg rosuvastatin purchase mastercard
Antegrade imaging is probably the most invasive choice cholesterol in foods buy 10 mg rosuvastatin free shipping, however cholesterol lowering diet plan 10 mg rosuvastatin order with mastercard, and carries risks of bleeding and adjoining organ damage. Chapter forty four Distal Ureteral Strictures 475 To quantify obstruction in a noninvasive manner, renal scintigraphy with diuretic washout provides the most correct evaluation [31]. Renal scintigraphy also permits the evaluation of differential renal perform, which can assist information remedy options. A renal unit contributing lower than 15% of total renal function is associated with poor outcomes. If renal operate is lower than 25% on the ipsilateral facet, statement alone is an affordable option [32]. Temporary drainage with a percutaneous nephrostomy may be entertained and equivocal operate reassessed after 4�6 weeks with renal scintigraphy, prior to definitive therapy. Endoluminal ultrasonography has been a promising technique in assessing ureteral strictures. While it has fallen out of favor somewhat, endoluminal ultrasonography can provide helpful anatomic detail of a stricture, together with stricture size, the presence of extraluminal vascularity, and the extent of periureteral scarring and fibrosis. With experience, this modality can establish potential causes or related conditions, corresponding to ureteral endometriosis, retroperitoneal fibrosis, and surgical clips and staples [33]. Ultrasonography requires the ureteral caliber to permit the passage of a 6F probe and requires transurethral introduction through cystoscopy. It is, therefore, only useful in partially obstructing distal ureteral strictures. Treatment options Temporary reduction of obstruction ensuing from ureteral strictures is often achieved using ureteral stents or percutaneous nephrostomy. Stents for distal strictures ensuing from extrinsic obstruction usually are an unsuccessful long-term resolution, with percutaneous drainage usually needed after delayed stent failure [37]. Definitive remedy options for distal ureteral strictures include balloon dilation and ureteroscopic endoureterotomy. Ureteral balloons differ in size (4�10 cm) and inflated diameter (4�10 mm), and might face up to maximum pressures of 40�225 kilos per square inch (psi). While views differ on the optimum balloon size and technique, we prefer a 4-cm lengthy, 6 mm (18F) Preoperative preparation Prior to intervention, all urinary tract infections ought to be treated and confirmation of therapy established with documentation of sterile urine preoperatively. Prophylactic preoperative antibiotics are indicated in all patients and can be given as single-dose remedy or continued for one to two doses after the procedure [34, 35]. Any suspicion of coagulopathy should immediate evaluation with applicable testing and ought to be corrected preoperatively. The affected person is often positioned in a dorsal lithotomy place for retrograde ureteroscopic approaches. If concurrent antegrade entry is probable, the affected person is placed in a inclined split-leg place [36]. However, as consolation with supine percutaneous renal access increases, mixed antegrade and retrograde approaches may be carried out in a dorsal lithotomy position with the ipsilateral flank raised. Retrograde or antegrade ureterography under fluoroscopy is performed concurrently with remedy to map therapy. Initial entry with an angled hydrophilic floppytipped guidewire could additionally be needed to traverse some strictures. Cold-knife incisions can be carried out with straight, hook, or half-moon configured blades under direct vision via a inflexible ureteroscope. Incisions are made under endoscopic visualization and always with guidewire access management (when not precluded by complete obstruction) [44]. Using a cold-knife incision has the benefit of a relatively low local inflammatory and cicatricial response due to the dearth of power transmitted [45]. Cold-knife endoureterotomy has total high charges of success for main and salvage procedures. The largest sequence to date of distal endoureterotomies carried out with a cold knife was reported by Eshghi and Lifson, showing a 95% success rate for 100 strictures in 89 sufferers [28]. Electrocautery can be utilized to incise distal ureteral strictures via ureteroscopy using 2�3F ball-tip electrocautery probes. While electrocautery boasts better hemostasis than a cold knife, it results in a extra substantial local tissue response, which carries a excessive stricture recurrence risk. Electrocautery requires the entry guidewire to be a well-insulated wire, or alternatively a slim ureteral catheter, to prevent longitudinal transmission of the current. A few studies have evaluated the efficacy of electrocautery in the distal ureter, including one by Ghoneim et al. Combining accuracy and lowered local response, laser endoureterotomy is associated with essentially the most favorable outcomes for distal ureteral strictures. Thirteen patients with stricture disease secondary to stone disease underwent laser endoureterotomy with a hit price of 56% [48]. Ureteral stenting after therapy of distal strictures is generally not contested. Stent use theoretically prevents recurrent stricture formation and urine extravasation, and promotes healing [1]. The choice of stent sort and measurement has been the topic of much debate, without defini- balloon for most strictures. The success fee of retrograde balloon dilation for ureteral strictures has been estimated to be 48�88%, with a 10�29-month follow-up [1]. Predictors of durable success for balloon dilation embrace nonischemic strictures which would possibly be lower than 1. In contrast, sufferers with ischemic strictures of longer lengths have demonstrable poor outcomes after balloon dilation with a patency price of 16. The balloon helps establish the diseased segment (as demonstrated by "waisting") and offers tamponade following cauterized incision. With solely fluoroscopic steering potential, cautious affected person and stricture selection is required to help reduce hemorrhage risk. Additionally, the chopping wire should be oriented in an anteromedial position when incising the ureter distal to the iliac arteries, and will by no means be used at the stage of iliac vessel crossing. For an incision to be efficient, chopping ought to be extended via the total thickness of the ureteral wall until periureteral fat is seen or till an adequate luminal diameter has been established. Without direct visualization, this interprets in to contrast extrusion on a subsequent retrograde ureterogram. Incision additionally ought to extend at least 2 mm proximal and distal to the area of stricture, and never just till balloon waisting is lost. They used a mix of approaches (retrograde, antegrade, and combined), and found 90% success with a sturdy median follow-up of 36 months. The use of endoluminal ultrasonography previous to balloon endoureterotomy utilizing the Acucise gadget reduced related issues in a research by Hendrikx et al. The group found no bleeding in a series of 27 patients following endoluminal ultrasonographic markings of periureteric structures. Ureteroscopic endoureterotomy A limitation of balloon endoureterotomy for ureteral strictures or ureteropelvic junction obstruction is the lack of direct visualization. We choose the use of a 7F double pigtail stent, though two 6F stents or a gently tapered endoureterotomy stent (6/10F) are viable alternatives. Asymptomatic sufferers with normal early postoperative imaging ought to be reimaged at 6-month intervals for as much as 3 years, as strictures are most likely to recur inside the first 3�36 months [32, 49, 51].
Rosuvastatin 10 mg buy with mastercard
At this point cholesterol levels equivalent rosuvastatin 10 mg trusted, it is important to cholesterol medication no muscle pain rosuvastatin 10 mg purchase on line reanalyze urine cultures that have been obtained preoperatively or throughout surgical procedure and, primarily based on their outcomes, redirect antibiotic remedy. It is imperative to modify the antibiotic routine to a tradition directed one when attainable. If severe sepsis/septic shock is acknowledged, apart from empiric antibiotic therapy, prompt treatment within the intensive care unit ought to include repletion of intravascular quantity with large amounts of crystalloid intravenous fluids. Pressors are administered as needed to maintain blood strain, central venous pressures are monitored, and fluids are administered to preserve a stress of 8�12 cmH2O. Bicarbonate and low-dose steroids could also be used and good blood glucose control maintained. Tight blood glucose control by administration of insulin doses up to 50 U/h is related to a discount in mortality. Recombinant activated protein C (dotrecogin alpha) is a model new drug that has been accredited for therapy of severe sepsis. Conclusions Septic issues in genitourinary surgery are a lifethreatening state of affairs that urologists want to keep away from during their practice. Reduction in surgical antimicrobial prophylaxis expenditure and the rate of surgical web site an infection by means of a protocol that controls using prophylaxis. Workgroup: Antimicrobial prophylaxis for surgical procedure: an advisory statement from the National Surgical Infection Prevention Project. Extracorporeal shock wave lithotripsy 25 years later: Complications and their prevention. Fever after shockwave lithotripsy: risk factors and indications for prophylactic antimicrobial therapy. Incidence and risk factors of bacteriuria after transurethral resection of the prostate. The postoperative bacteriuria rating: A new approach to predict nosocomial an infection after prostate surgery. Antibiotic prophylaxis for transurethral prostatic resection in men with preoperative urine containing lower than a hundred,000 micro organism per ml: a systematic evaluation. Severe sepsis and septic shock: Review of the literature and emergency department management pointers. Evidence based mostly prescription of antibiotics in urology: a 5-year review of microbiology. Discarding antimicrobial prophylaxis for transurethral resection of bladder tumor: A feasibility study. Mid stream urine C&S check is a poor predictor of infected urine proximal to the obstructing ureteric stone or contaminated stones: a potential medical examine. Stone and pelvic urine tradition and sensitivity are better than bladder urine as predictors of urosepsis following percutaneous nephrolithotomy: A prospective scientific study. Does a smaller tract in percutaneous nephrolithotomy contribute to excessive renal pelvic strain and postoperative fever Interaction of intracorporeal lithotripters with Proteus mirabilis inoculated inside artificial calcium and struvite stones. Inactivation of bacteria inoculated inside urinary stones-phantoms utilizing intracorporeal lithotripters. Percutanoeus nephrostomy versus ureteral stents for diversi�n of hydronephrosis brought on by stones: A potential, randomized scientific trial. Perioperative antimicrobial prophylaxis in transperitoneal tumor nephrectomy: does it decrease the speed of clinically important postoperative infections Antimicrobial prophylaxis in radical prostatectomy: 1-day versus 4-day therapies. Single-dose orally administered quinolone seems to be enough antibiotic prophylaxis for radical retropubic prostatectomy. Infectious issues in patients with continual bacteriuria undergoing main urologic surgery. Factors predisposing to urinary tract infections after J ureteral stent insertion. Procalcitonin as a diagnostic take a look at for sepsis in critically unwell adults and after surgical procedure or trauma: A systematic evaluate and meta-analysis. This chapter addresses anticoagulants and the management of sufferers on anticoagulants for specific urologic problems and procedures. In order to adequately perceive the mechanism of motion of the anticoagulants, a short evaluate of the hemostasis and coagulation cascade is important. Hemostasis requires appropriate operate of 4 key parts: platelet activation and aggregation, the clotting cascade, termination of clot formation, and fibrinolysis. Normal hemostasis Normal hemostasis requires a physiologic balance between prothrombotic and anticoagulant components. Vascular injury leads to the initiation of clotting and depends on three components: the vascular wall, platelets, and the coagulation cascade [1]. This is accomplished in three steps: adhesion, aggregation, and the secretion of procoagulant proteins that interact between platelets and endothelial cells, as well as between individual platelets. The second necessary step in thrombosis is the initiation of the coagulation cascade. The coagulation cascade is a series of steps in which proenzymes are transformed to activated enzymes, and the ultimate product is fibrin. At the site of vascular damage, the extrinsic pathway is initiated, starting with the discharge of tissue factor from endothelial cells. Factors Xa and Va symbolize a last frequent pathway for both the extrinsic and intrinsic pathways. Many of the proenzymes in the coagulation cascade are dependent upon vitamin K as a cofactor, and therefore antagonists such as warfarin will disrupt the coagulation course of. Drug-mediated anticoagulation Warfarin Warfarin is a vitamin K-dependent anticoagulant. This pathway causes oxidative reduction of vitamin K, which then allows for carboxylation of clotting factors from their inactive to active type. Therefore, warfarin administration ends in the inability to synthesize active vitamin K-dependent clotting elements. The results of this can be a delayed impact of antithrombotic activity till pre-existing energetic clotting components are expended. Careful monitoring of warfarin ranges is necessary as many variables can affect the efficacy of a given dose. These variables include vitamin K stores/intake, medical circumstances (liver disease, thyroid illness, an infection, fever, coronary heart failure), and medications (quinolones, antifungals, trimethoprim�sulfamethoxazole, amiodarone, rifampin, barbiturates, levothyroxine, metronidazole). It could be given as both intravenous and subcutaneous injection, and due to this fact anticoagulation administration can be carried out as an outpatient directed by the clinician. That incidence will increase to as high as 50% within the first 3 months after an initial occasion [4]. In 2008 the American College of Chest Physicians introduced guidelines relating to management of these patients talking vitamin K antagonists [5, 6]. Patients had been stratified according to threat (high, moderate, low) of either arterial or venous thromboembolic event based on the underlying need for anticoagulation (Table 5.

Rosuvastatin 10 mg visa
A shorter period between urinary diversion and balloon dilation was a more probably predictor of success cholesterol lowering foods wikipedia purchase 10 mg rosuvastatin with amex, though this was not uniform [6 cholesterol ratio of 4.2 10 mg rosuvastatin discount amex, 12, 23, 39�46]. The poor durable outcomes of this technique could also be explained by the physiologic effects of balloon dilation. Single-step, high-pressure balloons enable radial dilation of the stricture without the shearing trauma related to serial stepwise catheter dilation [29]. Additionally, hydraulic trauma to the neighboring wholesome ureter could result in additional ischemic harm [30]. Retrograde approaches While antegrade or mixed antegrade/retrograde approaches are generally utilized within the management of ureteroenteric strictures, direct retrograde access can conversely be tried to decrease the potential morbidity of percutaneous techniques. Initial retrograde access may be challenging secondary to inability to find the ureteral orifice throughout the intestinal mucosal folds of the diversion or tough location or angle of the ureteral orifice. Additionally, entry to the orifice could also be prohibited in sufferers with very lengthy or tortuous diversion limbs. Identification of the ureteral orifice may be aided by the excretion of indigo carmine following intravenous administration [35]. Also, contrast instillation within the urinary diversion might allow for better delineation of the suitable diversion limb and placement of the ureteral anastomosis [36]. Retrograde access is mostly not feasible in sufferers with nonrefluxing anastomoses secondary to the antireflux mechanism [37]. However, in different sufferers, as soon as the ureteral orifice has been identified, a straight or angled-tip 0. Wire development by way of the obstructed segment may be difficult in sufferers with vital stenosis or lengthy (> 1 cm) strictures and require antegrade approaches. Following wire placement previous the extent of obstruction, any of the previously discussed endoscopic strategies could also be utilized. Endoureterotomy Incision of the strictured ureteral section, whether by chilly knife, electrocautery, electroincision or laser, is the present endoscopic normal [23]. The technique is predicated on animal research by Davis in 1943 with intubated ureterotomy [49]. Davis noted that incised ureters healed over a stent by regrowth of the urothelium and subsequent easy muscle inside roughly 6 weeks. Later animal research involving endoureterotomy noted that there have been no significant difference in tissue harm, periureteral edema, and irritation regardless of the chopping modality used [48]. In 17 research involving 147 endoureterotomy procedures, total success was reported in 30�100% (mean 66%) of instances at a mean follow-up of 10�60 months (Table forty five. Study Number of procedures Diversion kind Mean follow-up (months) Success rate (%) Stricture size Stricture diameter Balloon size Time to conduit creation vs procedure Duration/ cycles/ strain Stent size (French) Stricture location (left, right) Stent length (weeks) Cold-knife incision 43 Poulakis et al. Chapter forty five Endoscopic Management of Ureteroenteric Strictures 489 slicing modalities tough. However, other experiences with this modality are fairly restricted in the literature. Electrocautery and holmium laser incisions have been related to comparable imply success charges of 69% and 72%, respectively, although imply follow-up in the laser teams was shorter (17. Both methods allow for precise incision beneath direct visualization and hemostatic management with instrumentation acquainted to most urologists. The electroincision group was primarily composed of Acucise remedies, though one study utilized a 7F electric papillotome [57]. The imply patency charges following electroincision (48%) have been lower as in comparability with the other endoureterotomy modalities, but higher than balloon dilation alone [13, 23, 53�57]. As famous with major balloon dilation, all studies utilized stents at the conclusion of the procedure. However, there was no consensus as to stent dimension (6�22F) and duration of stenting (1. Predictors of postoperative success included shorter stricture size (< 1 cm) and right-sided stricture, though this was not uniform in all research [3, 5, thirteen, 23, 24, 26, 28, 30, 38, 51�58]. Patients with poor ipsilateral renal operate (< 25% of complete renal function) have been unlikely to preserve patency after endoureterotomy [13]. Improvements in long-term patency rates following endoureterotomy may be contingent on a greater understanding of the therapeutic process of the ureter following incision. Unlike during open revision of the anastomosis, healing of the tissue happens through secondary intention. Animal studies since the seminal reviews by Davis observe a predominance of myofibroblasts in the course of the preliminary healing period, suggesting that therapeutic might, in part, happen via wound contraction. Thus, the ureteral stent could function a mold during healing rather than as a scaffold for cell regeneration [59]. This finding could clarify some reports that bigger stent sizes had been associated with improved outcomes [13, 60]. Increased collagen deposition resulting in fibrosis and scarring has additionally been noticed in histologic specimens of failed ureteral stricture repairs [61]. Local injection of adjunctive triamcinolone may block collagen formation and subsequent scarring [25]. Though reported use throughout endoureterotomy is limited, steroid injection following stricture incision has been beneficial in choose sequence [13, 26]. As noted in the included citations, a 6-week stent interval was mostly utilized, likely based on the findings of Davis. However, some porcine research have noted extra favorable histologic changes with a shorter stent duration, notably for strictures larger than 2 cm [62]. Continued research is necessary to decide the optimal healing parameters following ureteral endoureterotomy. Ureteral stenting Chronic indwelling ureteral stent placement could additionally be thought of in sufferers with vital comorbidities or extra probably in patients with a limited life-expectancy secondary to their main disease. Review of eleven publications detailing 86 procedures utilizing various ureteral stents for primary ureteroenteric stricture remedy noted successful fee of sixteen. One evaluation of 20 procedures famous solely a 45% long-term patency rate at a mean follow-up of 26 months. Repeated antegrade or retrograde insertion of the stent, notably in sufferers with ileal conduits, may be difficult and should require novel methods to assist with insertion [73]. The literature regarding use of the relatively new metallic double-pigtail stent for ureteroenteric strictures is also limited. In six cases of ureteroenteric stricture, placement of a metallic double-pigtail stent only had a 50% prolonged success as compared to 100 percent patency in 25 procedures for malignant obstruction [63]. Complications the reported issues following endoscopic administration of ureteroenteric strictures are generally related to the surrounding anatomy and comorbid diseases. Specific surgical issues directly related to balloon dilation are few. A sequence of 14 electrocautery procedures noted one ureteroenteric fistula that healed following prolonged stent placement [26]. In a multicenter trial of Acucise incisions, the authors famous common iliac artery 490 Table 45. Chapter forty five Endoscopic Management of Ureteroenteric Strictures 491 accidents in 4% of sufferers and cautioned in opposition to the use of the system in ureteroenteric strictures [56]. In the conventional anatomy, the distal ureteral section is provided laterally by branches of the inferior vesical artery.
Buy rosuvastatin 10 mg free shipping
The wavelength of a particular laser determines the physical properties of a laser in the clinical use setting cholesterol pills recall rosuvastatin 10 mg purchase amex. The small measurement of the supply tip facilitates glorious entry in restricted areas cholesterol ratio target purchase 10 mg rosuvastatin with mastercard, while its steel encasement prevents the breakage of this quartz fiber. A, Lateral view of the glenoid puncture web site with crucial adjacent structures. B tympanum ossicles, and middle ear; and the entire length of the medial facet of the capsule represented by the lateral pterygoid. Internal Arthroscopic Anatomy Posterior Recess the primary construction encountered upon coming into the joint is the synovium. The synovial membrane is mesenchymal in origin and a continuation of the cambium layer of the periosteum. B, Coronal view on the degree of the articular eminence (lateral-to-medial) with the adjacent anatomic structures. The medial synovial drape appears usually as a grey, translucent synovial lining. In the background of the medial aspect of the drape, the pterygoid shadow displays with a red/purple tinge. Intermediate Zone In the middle of the joint, the fibrocartilage of the glenoid fossa is seen, thin, white, and never very reflective. Anterior to the glenoid fossa and alongside the again slope of the articular eminence, the fibrocartilage becomes whiter and extra reflective of light and likewise takes on a basic look of striae formation that runs anterior to posterior. Changing the angle of view inferiorly, with the condyle ahead, a half of the disk could be seen as milky white, extremely reflective of sunshine, and without striations. The clear junction between the synovium and the posterior band of the disk is represented by a red-white line the place the capillary proliferation stops and the disk begins. A U-shaped depression or flexure between the synovial juncture and the posterior band of the disk can be observed. With the condyle seated, the disk covers the condyle and the flexure deepens considerably to the traditional anatomic position of the disk. Toward probably the most lateral depth of the joint are the articular eminence and the trough inside the eminence the place the disk strikes with the condylar translation. Anterior Recess In the anterior pouch, the anterior slope of the articular eminence is obvious. Meticulous cadaver middle cranial fossa dissection reveals the proximity of the articular glenoid fossa to the temporal lobe dura mater. The synovial lining is grayish with a translucent background and delicate in consistency. The normal synovium has a mild amount of capillary proliferation, diffuse all through the lining. With condyle ahead, the oblique protuberance is a fibroelastic band that protrudes in to the retrodiskal tissue. The synovium is tightly connected and has a gray, translucent background with mild capillary proliferation extensively dispersed throughout. The synovium can additionally be connected tightly to the anterior facet of the ascending facet of the articular eminence. The vertical striae of the drape are nonexistent, and the background consistency is deep purple secondary to the reflection of the pterygoid muscle fibers, a lot nearer in this area. The posteroanterior trough on the medial aspect of the joint is the place the synovium descends off the medial synovial drape after which attaches to the disk in the same fashion because the medial trough. From this point, approximately 10 mm anterior and 2 mm inferior to the road, the maximum concavity of the fossa is located. From a caudolateral place, the needle penetrates the tegument in the preauricular crease, roughly 10 mm inferior to the Holmlund-Helsing line, at the junction of the tragus and pina. Stenosed or fibrotic joints will sometimes take less fluid and the strain required to insufflate the joint is elevated ("early rebound"). Hypermobile joints or joints with disk perforations with out adhesions could require more fluid. The cannula is held in the right hand for a proper joint puncture or within the left hand for a left joint puncture. The index controls the tip, and the palm of the hand controls the base of the cannula. With the condyle forward, the pollicis of the nondominant hand palpates the steady zygomatic course of corresponding to the utmost concavity of the glenoid fossa immediately caudal. This puncture is carried out in a deliberate and cautious fashion, attempting one move through the lateral capsule in to the joint space. Multiple lacerations of the capsule from multiple makes an attempt trigger issues with extravasation through the course of the operation. The trocar is then advanced till contact is felt with the osseous structure superiorly. The zygomatic arch is felt between the pollicis of the nondominant hand and the index finger of the dominant hand. The preoperative examination ascertains joint mobility, articular bruits, and most necessary, the diploma of issue of the upcoming punctures. Once the anesthesiologist administers the muscle relaxant, all myofascial components related to condylar movement or disk operate are eradicated. An inconsistent but common discovering in patients with non-reducing disk derangements is the absence of this normal eminence subluxation. The postoperative dictation must include this explicit remark pertaining to the examination under anesthesia. By firmly urgent the condyle anterosuperior in opposition to the posterior slope of the eminence, then translating transferring the condyle in all excursions, simulating mastication mechanics, clicking and crepitus can simply be achieved. Cannula and trocar are advanced to the inferolateral facet of the zygoma, then inferiorly stepped off the osseous ledge. Instrumentation maintains continuous osseous contact all through this a half of the procedure. A posterior or straight angulation might end result in the laceration of the cartilaginous anterior wall of the external auditory meatus and, presumably, the perforation of the tympanic membrane and violation of the middle ear. Upon elimination of trocar from the cannula, the reflux of fluid confirms perforation of the capsule. The center portion of the cannula should, at this point, lever off the lateral facet of the lateral margin of the glenoid fossa. Before inserting the scope, the surgeon backwashes the joint in order to take away all blood and synovial fluid. The assistant insufflates the joint with 2 to three mL of fluid in order to keep joint distention. The function of the outflow needle is to set up a patent irrigation needle and, on the similar time, preserve the joint adequately distended for intra-articular instrumentation. A 22-gauge, 11/2-inch needle is inserted roughly 5 mm anterior and 5 mm inferior to the fossa puncture site, under joint insufflation.
Buy rosuvastatin 10 mg mastercard
The obstructed ureteral section was resected and the ureteroureterostomy was carried out laparoscopically over a ureteral stent cholesterol levels metric system discount rosuvastatin 10 mg fast delivery. In a retrospective review involving eight laparoscopic ureteroureterostomy sufferers cholesterol off rosuvastatin 10 mg buy on-line, Nezhat et al. Laparoscopic ureteroureterostomy is also an possibility for managing mid-ureteral obstruction because of a retrocaval ureter. Laparoscopic administration of ureteral injuries using a main ureteroureterostomy has additionally been described, albeit in just a few circumstances. When a ureteral harm happens throughout a laparoscopic procedure, for example, it can be primarily repaired over a stent utilizing intracorporeal laparoscopic suturing without the necessity for open conversion. The peritoneum is incised along the road of Toldt and prolonged caudally over the iliac vessels and medial to the medial umbilical ligament. The colon is mirrored medially and the entrapped ureter recognized with the indwelling stent appearing as a guide. Meticulous dissection is carried out to mobilize the ureter, liberating it from adjoining structures. Similar to the open surgical technique, a vessel loop can be positioned across the ureter to facilitate mild traction throughout mobilization. A biopsy of the retroperitoneal fibrotic process can be helpful if clinically indicated. Follow-up is predicated on serial evaluations, similar to the algorithm employed after open surgical repair. Two sufferers have been discharged home within 3 days postoperatively, whereas one patient had a lengthy hospital stay as a end result of Clostridium difficile colitis. Patency of the anastomosis was radiographically demonstrated at 6-month follow-up. At a imply follow-up of 13 months (range 6�33), all four renal items confirmed no proof of obstruction and no affected person required repeat surgical procedure. The total scientific experience in laparoscopic ureteroureterostomy is broadening [46]. As with ureteroureterostomy, laparoscopic method ought to mirror the open surgical process. Resecting a generous portion of decrease pole parenchyma and exposing a suitable calyx for anastomosis is key. Viable proximal ureter is spatulated and anastomosis performed with interrupted absorbable suture, generally over a ureteral stent. Postoperative management and follow-up is identical to that employed with pyeloplasty. Both ureteroureterostomy and ureterocalicostomy replicate glorious minimally invasive interventions for moderate size ureteral strictures or injuries. Conclusions With advances in approach and endoscopic instrumentation, urologists are generally employing minimally invasive therapies to address various urologic issues, together with ureteral obstruction. As progress continues in the field of endourology and laparoscopy, additional urologic procedures will be performed using a minimally invasive method, decreasing patient morbidity, while sustaining or increasing remedy efficacy. In this era of the endoscopist, minimally invasive remedy of ureteral strictures has not only turn out to be standard at teaching facilities, but is also generally employed in group settings worldwide. Laparoscopic Boari flap When the diseased ureteral section is distal and deemed too lengthy for main repair or when ureteral mobility is simply too restricted to perform a tension-free ureteroureterostomy or a Psoas hitch ureteroneocystostomy, a Boari flap repair is a helpful various. Evaluation of bladder operate must be carried out preoperatively in addition to the aforementioned evaluation of the ureteral stricture. Additionally, the bladder must be of enough capability to allow for creation of a sufficiently long Boari flap; in any other case different choices should be thought-about. A laparoscopic Boari flap has been successfully employed to treat long distal ureteral defects and strictures. Following open surgical ideas, the bladder is mobilized from its peritoneal attachments and the most superior contralateral bladder pedicle is divided, permitting larger mobility toward the ipsilateral ureter. The ipsilateral bladder pedicle, together with the superior vesical vasculature, is preserved and the affected ureter is rigorously mobilized, with care taken to protect its blood provide. Once the viable proximal ureter is outlined, a posterolateral bladder flap is outlined based on the vascular provide of the ipsilateral superior vesical artery. The bladder flap is created and anastomosed to the spatulated ureteral finish over a stent in a tension-free, References 1. Longterm outcomes of endourologic and percutaneous administration of ureteral strictures in bilharzial patients. Relief of urinary tract obstruction in tuberculosis to enhance renal operate: Analysis of predictive elements. Submucosal calculi: endoscopic and intraluminal sonographic prognosis and remedy choices. High failure fee of indwelling ureteral stents in sufferers with extrinsic obstruction: Experience at 2 establishments. Comparison of acucise endopyelotomy and endoballoon rupture for administration of secondary proximal ureteral stricture within the porcine model. The cold-knife approach for endourological administration of stenosis within the upper urinary tract. Endopyelotomy and endoureterotomy with the acucise ureteral cutting balloon system: preliminary experience. Endopyelotomy: comparability of ureteroscopic retrograde and antegrade percutaneous methods. Electrolysis for recanalization of urinary amassing system obstructions: A percutaneous strategy. A combined antegrade and retrograde approach for re-establishing ureteral continuity. Long-term results of the therapy of complete distal ureteral stenosis utilizing a slicing balloon catheter system. Ureterolysis for extrinsic ureteral obstruction: A comparison of laparoscopic and open surgical techniques. Strictures are the second most commonly handled disorder, outmoded only by obstructing ureteral calculi. Distal ureteral strictures can be defined as an irregular narrowing involving the lower third of the ureter. Such an impact can lead to pain, an infection, calculus formation, or renal dysfunction. It is the latter sequela that principally critically beckon the need for correct and reliable diagnosis, and effective and durable therapy. However, advances in ureteroscope design, method, and expertise have decreased the morbidity and mortality related to endoscopic restore. The obvious improve in incidence of clinically important distal ureteral strictures paralleling the increased range in remedy options may not be a coincidence. This can be partly explained by the iatrogenic nature of a large proportion of strictures recognized right now. Endoscopic administration of higher tract calculi and other problems has evidently come at a value.