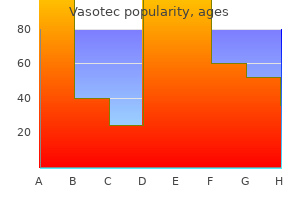
Vasotec
Vasotec dosages: 10 mg, 5 mg
Vasotec packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Generic 10 mg vasotec fast delivery
The splenic vein is cradled in a groove operating the length ofthe upper border ofthe posterior surf prehypertension 126 order vasotec 5 mg line. Numerous small branches drain from the tail and body of the pancreas in to the apposed floor ofthe vein prehypertension 120-139 over 80-89 5 mg vasotec buy with visa. The inferior mesenteric vein lies deep to the left posterior parietal peritoneum and ascends in shut proximity to the underlying infrarenal aorta. The proper gastric vein lies along the lesser curvature of the abdomen beneath the gastric root of the gastrohepatic omentum. The left gastric vein spans the gap between the esophagogastric junction and the posterior wall of the omental bursa mendacity alongside the left gastric artecy. It descends diagonally over the celiac trunk beneath the posterior peritoneum of the omental bursa to attain the portal vein. Small pyloric and duodenal veins also enter the portal vein near the gastric veins. The gastroepiploic arch connects the terminal splenic vein with the superior mesenteric vein and runs within the gastrocolic omentum where it receives dnrinage from the omentum and larger curvature of the stomach. It is associated with a variety of hepatic and extmhepatic problems which have been properly described e1Bewhere. Peripheral dilation is most harmful in the submucosal esophageal plexus connecting the portal circulation to the azygous system. Resultant esophageal varicosities are in peril of erosion and big hemorrhage. Beyond portal decompression sw:gery, there are two modem indications for exposure of the portal venous system: restore of traumatic injuries7�8 and resection and reconstruction of the portal and superior mesenteric veins in patients with invasive pancreatic tumors 1�10 the next dialogue considerations exposure of the portal vein and its tributaries in consideration of performing decompression procedures, repair of traumatic injuries, or reconstruction in sufferers with invasive pancreatic cancer. Alternatively, a midline incision could also be more appropriate in sufferers undergoing exploratory laparotomy for trauma or pancreaticoduodenectomy for most cancers. The hepatic flexw-e of the colon may often require mobilization to enhance publicity, but pointless dissection must be averted to decrease blood loss. The portal vein is normally distended and easily palpable as the most posterior structure in the hepatoduodenal ligament. It is essential to place the incision posteriorly and never too close to the free margin of the hepatoduodenalligament. U the incision is fastidiously extended superiorly so far as the liver hilum and inferiorly as far as the pinnacle of the pancreas. Gentle traction positioned on the portal vein exposes major branches, including the pyloric, duodenal, right gastric, and coronary veins, that drain in to its medial surfaces. After meticulous ligation and division of all portal vein tributaries are ensured, the portal vein can be exposed and fully mobilized from the extent of the pancreas to its bifurcation at the liver hilum. A midline stomach incision produced from a degree midway between the umbilicus and xiphoid process to the top of the pubis offers wonderful exposure and can be prolonged superiorly as essential. The incision must be carried to the left ofthe umbilicus to forestall entry in to the engmged umbilical vein. A transverse midabdoo:rinal incision is a helpful various however may be related to increased blood loss from venous collateral. The superior mesenteric artery can be palpated at the base of the transverse mesocolon; the vein lies to the right of the artery near the midline. A 7-cm transverse incision is made in the peritoneum on the root of the transverse mesocolon, and the superior mesenteric vein is carefully exposed. If needed, a superior T extension can be made on to the transverse mesocolon for added publicity. Multiple well-vascularized lymphatics overlying the vein require cautious dissection and meticulous management to avoid hemorrhage. Still, sufficient of the superior mesenteric vein can usually be isolated over the uncinate course of to allow creation of a big anastomosis. Alternatively, a brief H-graft configuration could be brought more directly from the vena cava to the posterior floor of the superior mesenteric vein. Grafts brought to the mesenteric vein from the vena cava on this trend are routed around the third portion of the duodenum and again anastomosed to the anterior surface of the superior mesenteric vein over the uncinate process. The patient is placed in the supine position with the decrease chest and stomach prepped and draped. Warren and Millikan12 advocate a "hockey stick" incision 1 to 2 em under the left costal margin, extending across the midline to the lateral border of the best rectus muscle. On getting into the stomach cavity, the falciform ligament and the umbilical vein are ligated and divided. After dividing adhesions between the posterior wall of the stomach and the pancreas, the larger curvature of the stomach is elevated, allowing cephalad retraction of the posterior abdomen. The posterior parietal peritoneum between the pancreas and the duodenum is relatively avascular and must be incised from the extent of the superior mesenteric vessels to the tail of the pancreas. The left adrenal and gonadal branches should be divided near the renal vein to allow wide mobilization. In preparation for anastomosis, the splenic vein should be divided as near the splenic-portal- mesenteric junction as possible and brought on to the left renal vein. An higher midline incision supplies excellent publicity, although a supraumbilical transverse incision may be used as a substitute. The retroperitoneal space is entered through a vertical incision within the posterior peritoneum over the infrarenal aorta. The incision is carried superiorly to include division of the ligament of Treitz, allowing rightward reflection of the third and fourth portions of the duodenum. The left renal vein is identified because it crosses the aorta within the superior incision. The vein is encircled, and its gonadal and adrenal branches are divided to allow wide mobilization. The inferior mesenteric vein should be identified as it courses alongside beneath the posterior parietal peritoneum to the left of the aorta and tJaced superiorly to locate the splenic vein. Anterior and cephalad retraction of the inferior border ofthe pancreas exposes the splenic vein coursing along the posterior pancreatic surface. A 20-year experience with portal and superior mesenteric venous accidents: has anything changed Techniques and outcomes of portal vein/superior mesenteric vein reconstruction using femoral and saphenous vein throughout pancreaticoduodenectomy. After crossing the pectineal line of the pubis, the vessels cross the pectineus musc:le en path to the subsartorial femoral canal. The boundary marking the transition between the exterior iliac and customary femoral arteries is the inguinal ligament. The sheath matches snugly across the vessels except on the medial side, where a narrow channel (femoral canal) Psoas major m. The hernia dissects and breaches the medial femoral sheath below the inguinal ligament to prolrude. The lateral margin of the triangle is shaped by the sartorius muscle, the medial margin by the adductor longus muscle, and the cephalad base of the Deep circumflex iliac a. Between these boundaries, the triangle seems as a depressed plane when the thigh is flexed in exterior rotation.
Purchase vasotec 5 mg amex
Often correlation between gross blood pressure 200 100 vasotec 5 mg generic on-line, microscopic arteria pack discount 10 mg vasotec with amex, and imaging findings is important to determine one of the best T class. Lymph nodes must be evaluated by thinly slicing and inspecting all nodal tissue in order to establish all macrometastases (metastases > 0. This system captures details about the extent of most cancers at the main website (tumour or T), the regional lymph nodes (nodes or N), and spread to distant metastatic websites (metastases or M). For individual patients, this info is essential for making decisions in regards to the management of native illness, as properly as to decide the value of systemic remedy. Determining tumour stage can be essential for organizing teams of similar patients for comparison in scientific trials, 20 research, with pathological affirmation after biopsy in some circumstances. The more and more widespread apply of initiating remedy earlier than definitive surgical therapy. Determining stage each earlier than and after therapy supplies essential prognostic data 221, 650. Alternatively, some subtypes of cancers are associated with a lower incidence of lymph-node metastases and will metastasize primarily via blood vessels 930,931. Immunohistochemical studies can be utilized to distinguish lymphatics from small capillaries and, in some circumstances, additional delicate foci can be recognized 929,930. Lymph-node status the status of the axillary lymph nodes is crucial single prognostic issue for all besides a small subset of breast carcinomas. Nodal metastases are strongly correlated with tumour dimension and the variety of invasive carcinomas 213,230,1451, 1581. Disease-free survival and overall survival diminish with every further positive node 920,976,1521. The ratio of positive to unfavorable nodes additionally supplies prognostic data and might adjust for differences in surgical and pathology practices that result in variable numbers of nodes evaluated 1522,1596. However, failure to examine all nodal tissue can lead to lacking macrometastases in as much as 40% of positive nodes 149,1343. Detection of smaller metastases might require further ranges in to paraffin blocks and/or immunohistochemical studies. More than 80% of those girls survive without recurrence at a median follow-up of eight years 1561. In chosen instances during which larger metastases could additionally be troublesome to detect, similar to lobular carcinomas, immunohistochemical studies may be helpful 299, 1490. Neither palpation nor available imaging techniques are reliable for the exclusion of nodal metastases, as most sufferers current with just a few nodes concerned by small metastases. Cancers drain to one or two sentinel nodes in the axilla, or rarely to other nodal basins, which may be recognized intraoperatively by either dye or radioactive tracer. Sentinel-node biopsy has confirmed to be a useful technique to separate node-positive from node-negative sufferers with reduced morbidity 74,682, 839. In the setting of presurgical or neoadjuvant remedy, small nodal metastases are indicative of an incomplete response to systemic remedy and have the same significance as bigger metastases 699. A complete response in recognized lymph-node metastases is more predictive of ultimate Staging 21 outcome than is the response within the major carcinoma 350,1226. Sentinel-node biopsy could be employed after treatment, although the false-negative rate is slightly higher 198,1050. Although adverse nodes are a very favourable prognostic factor, 10�30% of patients will finally develop distant metastases. There can be a small group of cancers that seem to metastasize haematogenously with out the involvement of nodes. For example, although basal-like carcinomas are a poor prognostic group, this is the molecular subtype least likely to exhibit intensive nodal involvement 1581. For these patients, different prognostic markers shall be extra necessary than nodal staging. Since all are targets and/ or indicators of highly efficient therapies towards invasive breast cancer in numerous clinical settings, accurate evaluation is important and necessary 33,242, 360. It is the accountability of every pathology laboratory evaluating these biomarkers to present accurate and reproducible outcomes. Stained slides are evaluated microscopically to determine the proportions and intensity of optimistic cells. A clinically positive check for each receptors is outlined as nuclear staining in 1% of tumour cells, and a unfavorable result as < 1%. These tips make many other recommendations supposed to promote correct reproducible outcomes, such as necessary confirmation of unlikely negative outcomes. There is a direct correlation between ranges of expression and response to hormonal therapies, and even tumours with very low ranges (1% optimistic cells) have a significant probability of responding 932, 1274. The remaining two discordant phenotypes are related to intermediate response A B. Several new molecular strategies for determining the standing of hormone receptors, in addition to different important biomarkers, which may be more highly effective than immunohistochemistry in predicting response to hormonal remedy and prognosis, are being developed 840, 843,1024,1059,1359. Studies show that the gene is amplified in approximately 15% of tumours in sufferers with primary breast most cancers, and that amplification is extremely correlated with elevated protein expression 33,242,383. Other chromogenic strategies of in situ hybridization that can accurately determine gene copy quantity using routine bright-field microscopy have gotten well-liked 1087A. However, the term is most commonly used to describe modifications seen after neoadjuvant therapy (also termed "main systemic therapy" or "presurgical remedy"), during which treatment (chemotherapy, endocrine remedy, and/ or focused therapy) is administered before surgical excision. In addition, some sufferers with large cancers may consequently become eligible for breast conservation 163,175. Kulka Post-therapy specimens the residual carcinoma or tumour mattress have to be discovered so as to evaluate response to remedy, and that is facilitated by the position of clips earlier than treatment. However, gross changes may be delicate, making pretreatment clip placement valuable. Residual cancers usually become softer and tougher to palpate, besides in cases of absent or minimal response. The macroscopic size of identifiable residual tumour or multiple tumour foci, as nicely as distances from the resection margins, ought to be recorded. More commonly, carcinomas turn into much less cellular and are sometimes present as scattered small nests throughout the tumour mattress. The size and cellularity of foci of the overall residual most cancers ought to be recorded, because the extent of residual invasive carcinoma, together with lymph-node status, is a strong predictor of long-term survival 221. In a number of cases, the remaining cancer cells become weird, possessing giant and irregular nuclei. The cytoplasm of the residual tumour cells may turn into vacuolated in about 40% of instances 939. In some circumstances, the only residual cancer is in lymphatic spaces and this discovering has been related to recurrence after neoadjuvant therapy 250A. Nevertheless, histological grade remains a prognostic factor after neoadjuvant remedy and must be reported 179. After an entire response, only a unfastened, oedematous, vascularized fibroelastotic area of connective tissue with continual inflammatory cells and macrophages might mark the tumour bed.
Vasotec 5 mg order free shipping
In addition blood pressure questions and answers vasotec 5 mg proven, promoter mutations and enormous exon deletions have additionally been recognized arrhythmia yoga vasotec 10 mg with mastercard. The syndrome is characterised by the development of colorectal carcinoma, endometrial carcinoma and different cancers. Other broadly used standards are the revised Bethesda pointers, that are less stringent 1478 (Table sixteen. Breast tumours With the principle exception of a single investigation 1291, no extra of breast carcinoma has been noticed in households with Lynch syndrome in contrast with the final inhabitants 2,90,482,1504,1559. The mean age at diagnosis reported for Lynch syndrome-associated breast most cancers varies from forty six 1504 to 66 years 1298. The threat of developing cancer depends on the predisposing gene, sex and environmental elements. Among extracolonic tumours from sufferers with Lynch syndrome, the relative danger is highest for carcinoma of the endometrium, ovaries, ureter, renal pelvis, and small bowel, that are due to this fact probably the most specific for Lynch syndrome 1558. Colorectal carcinomas are sometimes recognized at an early age (mean, 45�50 years) and the identical also applies to many extracolonic tumours, a minimal of when in comparison with the corresponding sporadic tumours 1503. It is related to heterozygous germline mutations in one 192 Genetic susceptibility: inherited syndromes Table 16. While > 80% of mutations are specific to each family, prevalent founder mutations occur in certain populations 1086. Characteristics of variants with reported outcomes of functional and/or in silico testing are available in a database. Occurrence of these mutations is clearly decrease (< 30%) in kindreds not meeting the Amsterdam standards 1013,1582. This has been proven to apply to virtually all colorectal carcinomas and extracolonic cancers of the Lynch-syndrome spectrum 531. Linkage studies lack the ability to identify common lower-penetrance variants, and these have been sought by way of case� control affiliation research. Early studies focused on polymorphisms in genes although to be functionally relevant, corresponding to genes concerned in hormone synthesis and metabolism, but this method has typically proved ineffective 1102. Although the dangers conferred by common loci are modest, genotyping in very large collaborative research can present definite proof of affiliation, and greater than 1300 loci for more than 200 widespread illnesses or traits have been identified by this approach ( Taken together, these loci explain about 8% of the familial risk of breast most cancers. It is probably going, nonetheless, that many further loci have been missed owing to lack of statistical energy, so the general contribution of widespread variants to breast-cancer susceptibility is probably much larger. It is important to note that, in almost all instances, the gene(s) driving the association are still unknown. Identification of the causal variant can be problematic, owing to the sturdy linkage disequilibrium amongst neighbouring markers. The causal variants could additionally be related to higher risks of breast cancer than the markers identified. While the dangers associated with the frequent low-penetrance alleles are modest, these dangers appear to combine multiplicatively, so that the entire impact on risk may be substantial. While discrimination is probably too poor to present helpful threat prediction in isolation, it could turn into more necessary as extra alleles are identified, and will already be helpful in girls with a household history of the illness or in combination with different danger components. Reprinted with permission from Churchill Livingsone Press, London,� (2013) Elsevier. Department of Pathology, Netherlands Cancer Institute, Amsterdam, the Netherlands Schnitt S. Gerhard Domagk Institute of Pathology, University of M�nster, M�nster, Germany Nielsen B. Correlation between medical outcome and development factor pathway expression in osteogenic sarcoma. Morphologic and molecular evolutionary pathways of low nuclear grade invasive breast cancers and their putative precursor lesions: additional evidence to assist the idea of low nuclear grade breast neoplasia household. Dermal lymphatic invasion and inflammatory breast most cancers are unbiased predictors of outcome after postmastectomy radiation. High prognostic significance of residual disease after neoadjuvant chemotherapy: a retrospective research in 710 patients with operable breast cancer. Wide spectrum screening keratin as a marker of metaplastic spindle cell carcinoma of the breast: an immunohistochemical study of 24 sufferers. Adelaide J, Finetti P, Bekhouche I, Repellini L, Geneix J, Sircoulomb F, CharafeJauffret E, Cervera N, Desplans J, Parzy D, Schoenmakers E, Viens P, Jacquemier J, Birnbaum D, Bertucci F, Chaffanet M (2007). Malignant adenomyoepithelioma of the breast with malignant proliferation of epithelial and myoepithelial parts: a case report and review of the literature. The results of chemotherapy on breast most cancers tissue in regionally advanced breast most cancers. Breast papillomas: present management with a concentrate on a model new diagnostic and therapeutic modality. Cylindroma (dermal analog tumor) of the breast: a comparability with cylindroma of the pores and skin and adenoid cystic carcinoma of the breast. A review and meta-analysis of pink and processed meat consumption and breast most cancers. Cowden syndrome and reconstructive breast surgical procedure: Case reports and evaluation of the literature. Biological options of human premalignant breast disease and the development to cancer. Ductal carcinoma in situ and the emergence of range throughout breast cancer evolution. Relationship of sialylLewis(x/a) underexpression and E-cadherin overexpression within the lymphovascular embolus of inflammatory breast carcinoma. The role of oestrogen and progesterone receptors in human mammary development and tumorigenesis. Comparison of age distribution patterns for various histopathologic forms of breast carcinoma. Risk of invasive breast cancer after lobular intra-epithelial neoplasia: evaluation of the literature. Columnar cell lesions and subsequent breast cancer threat: a nested case-control examine. Infiltrating lobular carcinoma of the breast: tumor traits and clinical outcome. Accumulation of chromosomal imbalances from intraductal proliferative lesions to adjoining in situ and invasive ductal breast cancer. Invasive tubular carcinoma of the breast frequently is clonally related to flat epithelial atypia and low-grade ductal carcinoma in situ. Azoulay S, Lae M, Freneaux P, Merle S, Al Ghuzlan A, Chnecker C, Rosty C, Klijanienko J, Sigal-Zafrani B, Salmon R, Fourquet A, Sastre-Garau X, Vincent-Salomon A (2005).
Generic vasotec 5 mg with visa
Sporotrichosis Sporotrichum schenckii blood pressure korotkoff sounds order 5 mg vasotec mastercard, a fungus regularly found in soil or on backyard vegetation blood pressure of 120/80 cheap 5 mg vasotec overnight delivery, produces cutaneous and subcutaneous lesions and inflammation of the lymph vessels (lymphangitis). This indolent infection is characterized by a pilot lesion at the web site of inoculation, adopted by the looks of a succession of satellite lesions, which progress proximally along a lymphatic chain. The lesions are raised, purple, swollen, and often about 1 cm in diameter; the center might ulcerate and drain. The therapy of selection is topical utility of potassium iodide, which is effective within the benign form of the disease. Sporotrichosis may remain localized or unfold systemically to involve different organ systems. Wound packed open with gauze soaked in dilute povidone-iodine resolution, then covered with fluffed gauze Bulky dressing applied with wrist partly prolonged, metacarpophalangeal and interphalangeal joints slightly flexed. The deep compartments of the hand could turn into infected by direct inoculation by way of penetrating wounds or by extension of infection in adjoining areas. Such infections are comparatively rare, however when current they trigger rapid deleterious adjustments and are susceptible to spreading. Unless treated with incision and drainage, deep infection may cause everlasting deformity. Infection of Midpalmar Space the midpalmar space lies underneath the flexor tendons of the ulnar three fingers and over the deep fascia covering the intrinsic muscles. Ulnarly, the hypothenar muscular tissues and, radially, the adductor pollicis muscle define the house, which is partially separated by fibrous septa that attach the palmar flooring to the central ridges of the metacarpal shafts. Purulence might enter or extend through the lumbrical canals or break through in to the carpal canal or thenar house. Symptoms such as ache on movement, swelling, and marked tenderness could rapidly increase in severity. Treatment is by incision, which follows pores and skin creases and is centered to enable access to the midpalmar space and retraction of the flexor tendons. Usually, the purulence is beneath stress when the midpalmar area is opened and could be aspirated and the house irrigated. Extensions in to adjoining areas may be recognized by massaging the palm, starting at the perimeter. Infection of Thenar Space the thenar house lies underneath the flexor tendons of the index finger and over the adductor pollicis muscle. The septum to the third metacarpal defines the ulnar border, and the thenar muscular tissues define the radial border. The infection could lengthen in to the lumbrical canal of the index finger and over the distal facet of the adductor pollicis muscle. A dorsal thenar house infection on the dorsal aspect of the adductor pollicis muscle could dissect underneath the primary dorsal interosseous muscle. An incision along the thenar space must avoid the recurrent motor department of the median nerve. Collar Button Abscess these sort of abscesses derive their name from the dumbbell-shaped contour of the abscess across the margin of the superficial transverse metacarpal ligament in one of many web areas. Infection of Parona Space the Parona space lies deep to the flexor tendon sheaths in the distal forearm and volar to the pronator quadratus muscle. Infections are often because of direct inoculation or extension from an infection of the tendon sheaths. An abscess may be drained by way of a direct palmar incision if the radial and ulnar bursae are involved. Branch of median nerve to thenar muscle tissue (in phantom) Infection of thenar house from tenosynovitis of index finger because of puncture wound. Palmar aponeurosis Lumbrical muscle Pus in web area Metacarpal Midpalmar area Sagittal part reveals an infection of web area (collar button abscess). Infections from Human and Animal Bites Teeth carry a wide selection of virulent organisms, and a bite might inoculate these organisms deeply in to tissues of the hand. Most dogs and cats are carriers of Pasteurella multocida, an organism that produces a quickly spreading inflammation which will penetrate subcutaneous and subfascial areas in addition to tendon sheaths and deep compartments. More aggressive and earlier therapy is required for cat bites as a outcome of delayed surgical therapy results in very slow decision of an infection. Human bites carry streptococcal, staphylococcal, spirochetal, and gram-negative organisms. Penetration of the metacarpophalangeal joint by an incisor may lead to a destructive septic arthritis and dissemination of infection in to the adjacent spaces. Lymphangitic erythematous streaks begin to kind over the dorsum of the hand, progressing in only a few hours in to the forearm and then in to the arm. On examination, the affected person appears anxious, protects the concerned arm, and will shiver with chills. The wound and the lymphangitic streaks are tender to the touch, as are the gentle, swollen epitrochlear and axillary nodes. There could also be a small serous drainage at the wound website, which ought to be cultured and Gram stained. Because streptococci are the usual causative organisms, treatment with penicillin or cephalosporin is began instantly. The perimeter of the erythema on the wound site and the lymphangitic streaks could be marked with a pen for later reference, and the scale of the nodes is famous. Necrotizing Fasciitis Also referred to as a Meleney ulcer, necrotizing fasciitis is a extreme manifestation of lymphangitis that progresses in a frightening method within a number of hours. Anaerobic or microaerophilic streptococci are believed to be the same old trigger, however these microorganisms are tough to tradition. Tissue necrosis develops rapidly behind an advancing wall of irritation that limits penetration by antibiotics. The pores and skin lesions are incised and drained or aspirated to acquire fluid for culture. Intravenous infusion of aqueous penicillin should be instituted instantly; additional antibiotics may be recommended by an infectious illness specialist. Even when the necrotizing lymphangitis is managed early, however, autoamputation may be a sequela and demise is an occasional end result. Other Hand Infections the previous discussion is merely an introduction to the higher scope of infections of the hand. Mycobacterium Epitrochlear lymph nodes Lymphangitis Site of infection Necrotizing fasciitis (Meleney ulcer) marinum is an organism incessantly associated with injuries because of marine actions. Rare invaders of the musculoskeletal system are fungal infections, together with coccidioidomycosis and blastomycosis. Clostridium perfringens may colonize crushed muscle within the hand, producing fuel gangrene. Rare viral infections transmitted from domestic animals sometimes produce lesions on the hand, and irritation that mimics an infection. The introduction of antibiotics has dramatically improved the prognosis for infections of the hand. For optimum treatment, however, the proper analysis should be established, the organism identified, the purulence drained, and an applicable rehabilitation program instituted. Intravenous line additionally established in opposite limb for use if issues develop.
5 mg vasotec free shipping
Adductors of vocal twine: They are lateral cricoarytenoid hypertension online generic vasotec 5 mg without prescription, thyroarytenoid hypertension teaching plan cheap vasotec 10 mg with visa, and interarytenoid muscular tissues. The ground of mouth forms the upper limit of neck anteriorly whereas posteriorly higher border is base of skull. Surface anatoMy the following landmarks of floor anatomy are essential for neck examination as well as for planning the surgical incision. Anterior and posterior neck triangles separated by sternocleidomastoid muscle Mastoid: It provides insertion to sternocleidomastoid muscle. Mandible: the submandibular gland may be palpated slightly below the ramus of mandible. The marginal mandibular department of facial nerve crosses the decrease border of mandible superficial to facial vessels just anterior to masseter muscle. The cricothyroid membrane located between thyroid and cricoid cartilages is the site of emergency tracheostomy. Trachea: the cervical trachea can be shifted to either side as a end result of thyroid and superior mediastinal tumors. The accent nerve programs across the roof of posterior triangle and enters the anterior border of trapezius at the junction of its center and lower third. Blood provide: Branches of occipital and superior thyroid arteries (branches of external carotid artery). Trapezius muscle: this huge muscle makes the posterior boundary of posterior triangle and elevates the shoulder. The digastric and omohyoid muscle tissue divide these triangles in to further sub-triangles. The anterior and posterior bellies of digastric and superior belly of omohyoid divide the anterior triangle in to four triangles: seventy four provide as the vessels penetrate the superficial fascia. The house between superficial fascia and investing layer of deep cervical fascia contains following buildings: 1. The inner lamina covers medial surface of pterygoid muscle up to the cranium base tympanic bone, styloid course of and types stylomandibular ligament. Submandibular: It is bounded by the lower border of mandible and anterior and posterior bellies of digastric. Contents embody submandibular salivary gland, lymph nodes, facial vessels and marginal department of facial nerve. The contents embrace infrahyoid strap muscles and constructions which lie deep to them in central compartment like thyroid and parathyroids, larynx and trachea, laryngopharynx and cervical esophagus and carotid sheath. Its contents include accent nerve, lymph nodes, fibrofatty tissue and nerves of cervical plexus. At the transverse processes of cervical vertebra it divides in to two divisions: anterior (alar) and posterior (prevertebral). Prevertebral division: It extends from cranium base down the length of vertebral column as much as coccyx. It types the floor of posterior triangle and facilitates gliding motion of pharynx during the swallowing. Submental nodes, two to eight in quantity, lie on the mylohyoid muscle in the submental triangle, which is located between right and left anterior bellies of digastric muscle tissue and the hyoid bone. Submandibular nodes, that are in relation to submandibular gland and facial artery, lie in submandibular (digastric) triangle, which is situated between anterior and posterior bellies of digastric muscle and bounded superiorly by the decrease border of mandible and an imaginary line drawn between the angle of mandible and mastoid. Occipital nodes, on the apex of the posterior triangle, are situated each superficial and deep in to splenius capitus muscle. Internal jugular chain, which is additional divided in to higher (jugulodigastric node), center and decrease teams, lie anterior, lateral and posterior to inside jugular vein and extends from the digastric muscle to the subclavian vein. The posterior cervical triangle lies between posterior border of sternocleidomastoid, anterior border of trapezius and the clavicle below. Anterior cervical nodes, which lie between the two carotids and below the extent of hyoid bone, include two chains: anterior jugular chain and juxtavisceral chain. Middle deep cervical group: Afferents from oral cavity, oropharynx, hypopharynx, larynx, and thyroid. Afferents from scalp, skin of the neck, nasopharynx, occipital and postauricular nodes; Efferents to transverse cervical chain. Medial supraclavicular (scalene nodes): Afferents from breast, lung, stomach, colon, ovary and testis. Paratracheal nodes (recurrent laryngeal nerve chain): Afferents from thyroid lobes, subglottic larynx, trachea and cervical esophagus. Section 1 w � lymph Nodes Not Clinically Palpable � retropharyngeal nodes: lateral (rouviere) and medial teams: Afferent from nasal cavity, paranasal sinuses, onerous and taste bud, nasopharynx, and posterior wall of pharynx; Efferents to upper internal jugular group. Afferents from anterior a part of the ground of mouth and ventral surface of tongue; Efferents to submandibular or upper jugular nodes. The deep cervical jugular groups obtain in addition to their direct areas of drainage all the efferents from the pericraniocervical ring, efferents from the superficial cervical nodes and efferents from different paravisceral deep nodes (such as retropharyngeal, infrahyoid, prelaryngeal, pretracheal, paratracheal and subclavian). All the lymph from the head and neck lastly drains in to ipsilateral decrease deep cervical group (terminal group). Efferents from the latter converge and type (right and left) jugular lymph trunks that descends on its vein to its termination on the jugulosubclavian venous junction (thoracic duct on left side). Metastasis in these nodes, which embrace lower part of taBle 2 Levels of cervical lymph nodes 77 1. It removes metastases to cervical lymph nodes and their surrounding fibrofatty tissues. Following important buildings, which though are encountered through the surgery, should be saved. Cervical sympathetic trunk and thyrocervical trunk giving inferior thyroid artery lie posterior to carotid sheath. Section 1 Modified Neck Dissection Modified neck dissection is just like radical neck dissection but with certain modifications, which embody preservation of one or more of the next constructions: Spinal accent nerve Internal jugular vein Sternocleidomastoid muscle. Selective Neck Dissection In selective neck dissection, in addition to the three nonlymphatic structures (spinal accent, sternocleidomastoid fig. The inferior thyroid artery arises from the thyrocervical trunk and pierces the prevertebral fascia medial to carotid sheath and enters in to the posterior part of thyroid lobe. Inferior parathyroids: They are posteriorly placed on the lower poles inferior to inferior thyroid artery. Thyroid gland Thyroid gland develops from midline thyroid diverticulum that forms in the floor of foregut and migrates caudally to its adult place. The cyst is mostly seen close to the hyoid bone but may be found on the base of tongue (lingual cyst). Nerves preserved in radical neck dissection: They embrace vagus, hypoglossal and phrenic. Elective neck dissection: In medullary carcinoma of thyroid, elective neck dissection is acceptable. Rests of the 23 species, which are coagulase-negative, can survive on inanimate objects corresponding to implants, intravascular traces and prosthetic valves. The nasopharynx may be colonized with doubtlessly pathogenic bacteria with out sick effect in majority of individuals. Staphylococcus aureus this coagulase-positive Staphylococcus usually produces golden colonies on blood agar.
Bifidobacteria. Vasotec.
- How does Bifidobacteria work?
- Prevention of diarrhea in infants, when used with another bacterium called Streptococcus thermophilus.
- Are there any interactions with medications?
- Are there safety concerns?
- Preventing a complication after surgery for ulcerative colitis called pouchitis.
- What is Bifidobacteria?
- What other names is Bifidobacteria known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96858
Buy cheap vasotec 5 mg
Surgical restore of the ruptured tendon is best accomplished inside the first several weeks after damage hypertension 7101 vasotec 5 mg cheap with mastercard, before the tendon becomes significantly retracted blood pressure medication vision safe 10 mg vasotec, and could be performed via a single-incision or two-incision method. Chronic injuries may be troublesome to repair as a result of the tendon could also be too scarred and retracted to be brought again to bone. Chronic accidents could do properly with nonoperative management centered on bodily therapy to regain as a lot strength and function as potential, but supination weak spot is usually still noticeable. Rupture of the distal triceps tendon is an even rarer harm than rupture of the distal biceps but may happen more equally in both men and women. The mechanism of harm is usually attributable to a sudden, forceful extension of the elbow against resistance, and rupture often happens on the tendon insertion on the olecranon. As with distal biceps rupture, scientific findings embody swelling, ecchymosis, and beauty deformity. Surgical restore of the ruptured tendon can be best carried out throughout the first a quantity of weeks after injury, before the tendon turns into considerably retracted. Chronic accidents also may require reconstructive methods with graft tissue, such as Achilles tendon allograft, to span a defect. Disruption or attenuation of this ligament will result in medial or valgus elbow instability. Typically this may be a persistent overuse harm, similar to with repetitive overhead use or throwing. Rarely, isolated, acute rupture of this ligament can occur from a valgus load, corresponding to a fall on an outstretched hand. In persistent throwing injuries, ache is usually gradual in onset along the medial aspect of the elbow and associated with the acceleration phase of pitching, when valgus stress throughout the elbow is best. Tearing usually happens in the midsubstance of the ligament or on the distal insertion with these accidents. Associated pathologic processes may be present in throwers, including ulnar neuritis, posteromedial olecranon osteophytes, unfastened our bodies, or osteochondritis dissecans of the capitellum. Valgus instability may be troublesome to elicit in an awake patient on examination because of muscle guarding, but patients will sometimes complain of pain and/or apprehension with valgus stress testing. Treatment is initially nonoperative and contains relaxation and activity modification, followed by a graduated rehabilitation and/or throwing program. Surgery is indicated for failure of nonoperative administration and consists of ulnar collateral ligament reconstruction with autograft. In the uncommon cases of acute, isolated rupture of the ulnar collateral ligament, surgical repair of the torn ligament can be carried out. When the elbow is introduced in to extension with this maneuver, the radial head will subluxate or dislocate, whereas elbow flexion and/or pronation will scale back the radial head again in to anatomic position. Valgus Valgus stress testing for medial elbow instability With the elbow in a barely flexed place, a valgus stress is applied. Objective widening and/or affected person pain and apprehension on the medial side of the elbow can suggest instability. Intraoperative lateral fluoroscopic picture demonstrates widening of the elbow joint because of posterolateral instability. This ligament is the primary restraint to varus stress of the elbow, and ligament disruption leads to posterolateral rotatory instability. Symptoms embrace lateral elbow pain and instability complaints, similar to catching or giving means of the elbow. As with the medial side of the elbow, instability could additionally be difficult to elicit in an awake affected person on examination because of muscle guarding, but patients could complain of pain and/or apprehension with varus or posterolateral stress testing (see Plate 2-40). Treatment is initially nonoperative and contains rest, exercise modification, and a rehabilitation program. A hinged elbow brace may be useful within the acute setting to present stability while the injury is healing. The repetitive valgus loads may create compressive forces throughout the lateral aspect of the elbow at the typical site of a pathologic course of in the capitellum. It is believed that these forces trigger repetitive microtrauma and vascular insufficiency or harm to the capitellum that may result in separation of the articular cartilage from the underlying subchondral bone. The situation occurs after the capitellum has almost completely ossified and includes both the articular cartilage and the underlying bone. If the articular cartilage turns into separated from the subchondral bone, it can turn out to be a unfastened physique within the elbow joint. Symptoms embrace activity-related lateral elbow pain which will enhance with relaxation from the offending activity. Mechanical symptoms, such as clicking or locking, may be current if a unfastened fragment develops. On examination, tenderness to palpation is noted over the capitellum and a joint effusion could additionally be present. Range of motion of the elbow could produce crepitus, and patients commonly lack the terminal 10 to 30 degrees of elbow extension. Limitation of elbow flexion or of forearm pronation and supination may also occur however is much less common. Plain radiographs can show lucency or fragmentation at the capitellum and a possible loose body if a fragment has broken off. For intact lesions without mechanical symptoms, therapy is initially nonoperative and includes relaxation and exercise modification, with use of nonsteroidal antiinflammatory agents as needed, followed by a graduated rehabilitation program and return to participation in the sport. Internal fixation of intact lesions may be performed both open or arthroscopically if nonoperative administration fails. Displaced lesions or free fragments typically require surgical excision of the fragment with drilling or microfracture of the capitellar defect. Newer strategies of articular cartilage implantation at the second are being attempted in defects to try to restore normal articular cartilage, rather than the fibrocartilage produced by a microfracture approach. Panner disease typically occurs within the dominant elbow of boys in the course of the interval of energetic ossification of the capitellar epiphysis at between 7 and 12 years of age, with a peak at age 9 years. The pathologic course of is just like that of LeggCalv�-Perthes disease and is believed to be brought on by interference in the blood provide to the growing epiphysis, which leads to resorption and eventual restore and substitute of the ossification middle. The exact reason for this avascular necrosis, or bone infarct, continues to be debated, with popular theories together with continual repetitive trauma, congenital and hereditary components, embolism (particularly fat), and endocrine disturbances. Tenderness and swelling alongside the lateral side of the elbow with lack of terminal elbow extension are additionally frequent. Initial radiographic changes can seem just like osteochondritis dissecans, with fragmentation of the capitellar epiphysis, but whereas lesions of osteochondritis dissecans can often progress to loose fragments, free bodies are uncommon in Panner illness. Symptomatic treatment of Panner disease is enough, as a result of the situation is self-limited, with the epiphysis turning into revascularized and returning to a normal configuration with time. Rest and exercise modification normally relieve the ache and allow gradual return of elbow motion. Use of a long-arm solid or splint for three to four weeks could additionally be essential until ache, swelling, and native tenderness subside. The long-term prognosis is excellent, with full decision of symptoms in most sufferers, although a slight lack of elbow extension may persist in some.
5 mg vasotec proven
A revision amputation may be a better therapy alternative blood pressure chart and pulse vasotec 5 mg buy lowest price, especially within the older affected person arrhythmia on ekg discount vasotec 10 mg otc. Prolonged Ischemia Either heat (32�C) or chilly (5� to 10�C) ischemia seriously reduces the likelihood of a profitable replantation. Once the replantation procedure begins, the half goes by way of a second period of heat ischemia until vascular continuity is restored. Cooling (cold ischemia) to about 10�C clearly helps to protect the amputated half. Given sufficient cooling, main replantations have been successfully carried out eight to 16 hours after amputation and minor replantations have been successful even after 18 to 30 hours. Clamps operating suture may be used, fastidiously avoiding pursemay be used but very cautiously. Second forceps applied simply distal to first and slid farther downstream to milk blood from intervening section. Treatment on the scene of the accident and at first medical contact strongly impacts the end result of later replantation. Improper dealing with of the amputated half or stump can significantly compromise the ultimate outcome. The patient have to be hemodynamically secure earlier than either transportation or replantation is tried. If bleeding persists, nonetheless, it should never be stopped with the blind utility of a hemostat, because this will likely additional damage the neurovascular buildings. Graft harvested from dorsum of finger or volar aspect of wrist; for vein replantations in decrease limb of constructions bigger than digit, graft obtained from saphenous vein. Digital nerves comprise solely sensory fibers and are repaired with simple sutures by way of epineurium solely. The severed half is cleaned of any gross contamination and overseas materials and cooled to cut back its metabolic fee. A severed digit should be wrapped in moist gauze and positioned in a watertight plastic bag, which is then immersed in ice water. The amputated part should not be allowed to are available to direct contact with any ice, and dry ice ought to by no means be used. Properly cooled, a digit may be successfully replanted within 30 hours of amputation. The amputated part is cleaned of all gross contamination, wrapped in a moist towel, and positioned in a plastic bag. Alternative technique is to compress finger pulp and note time for return of turgor and shade similar to normal finger. The part is then positioned in an insulated container (but not in contact with the ice) and maintained at 10�C. Thus ready, the amputated half is clearly labeled and rapidly transported to the replantation center. Cold ischemia can preserve muscle as much as 8 to 12 hours, after which irreversible changes could occur. Warm ischemia, which results from improper cooling, can lead to irreversible adjustments in as little as 4 to 6 hours, thus preventing profitable replantation. Several makes an attempt have been made to reduce ischemia time by perfusing the amputated limb with various substances corresponding to oxygenated fluorocarbon solutions. At present, probably the most reliable fluid seems to be autologous arterial blood combined with heparin. Perfusion plus cooling may make major replantations possible as much as 12 to 16 hours after injury. In the emergency department, tetanus prophylaxis and a broad-spectrum antibiotic are administered as quickly as possible. Once the choice to undertake replantation is made, the severed half is taken to the operating room. While one staff prepares the affected person for surgery, the other staff completely debrides the amputated half, viewing it under magnification. All devitalized and heavily contaminated tissue is excised, together with frayed tendon ends, comminuted bone fragments, however only a small margin of skin, as a result of coverage is important and pores and skin is more resilient than deeper tissues. Frayed tendon ends are excised as a end result of Pulse oxygen monitor Tracing exhibits occluded blood provide the injury to the exposed tendon surfaces significantly increases the risk that adhesions will subsequently kind and restrict motion. Bone is trimmed to (1) take away avascular bone that would initiate the event of osteomyelitis; (2) provide flat, congruent surfaces for secure bone fixation; and (3) present the mandatory skeletal shortening to facilitate tension-free vessel anastomoses and nerve coaptations after debridement. An interosseous wire or a Kirschner wire can be positioned in the bone of the amputated part to facilitate later fixation. The distal arteries, veins, and nerves are recognized and tagged with nice sutures. Only full-thickness pores and skin flaps are mirrored; the subcutaneous tissue and veins are left intact for later dissection under microscopic visualization. While the amputated half is being prepared, the patient is transferred to the working room and regional anesthesia is run (preferably an axillary block). Regional anesthesia offers some sympathetic blockade and vasodilation in addition to pain reduction. The surgeon totally debrides the stump, shortening the bone and tendon to permit easier anastomosis of vessels and coaptation of nerves. Once corresponding buildings within the stump and the amputated half have been identified, replantation is begun. Because stability is crucial for the vascular reconstruction, bone fixation is carried out first. The technique of bone fixation should be acceptable for the sort and level of amputation and supply stable fixation for early mobilization. Fixation gadgets embody interosseous wires, Kirschner wires, and compression plates and should reduce further soft tissue disruption. Replantation on the phalangeal stage can be secured with interosseous wires with or without the added stability of a Kirschner wire; some surgeons favor to use crossed Kirschner wires. Replantations on the joint stage require a removable fixation gadget if the joint is to be preserved; otherwise, any commonplace approach for arthrodesis of small joints is appropriate. If contamination is critical, however, an exterior fixator must be used to reduce the risk of infection. Severed palmar metacarpal arteries from deep palmar arch to frequent digital arteries ligated to keep away from hematoma. Kirchmayr (Kessler) sutures are used to restore flexor tendons, and interrupted figure-of-eight sutures are used for extensor tendons. Repair of Blood Vessels and Nerves After restore of bone and tendon, microvascular clamps are utilized to the prepared arteries and veins, the tourniquet is launched, and the blood move is famous. Flap with adequate subcutaneous tissue dissected free with vascular pedicle getting into at one finish and leaving at other. Repairing rather than resecting injured and compromised vessels to avoid use of vein grafts nearly at all times ends in failure as a end result of thrombosis occurs virtually instantly in these injured vessels. Generally, the arteries are repaired first to reduce ischemia time and to enable the surgeon to assess the adequacy of the venous debridement and determine which veins are greatest fitted to restore.
Purchase vasotec 5 mg overnight delivery
Chronic erythematous/atrophic candidiasis this could be a type of denture sore mouth which may remain asymptomatic blood pressure veins vasotec 5 mg sale. Initial remedy: Prednisone 1 mg/kg supplemented by azathioprine or mycophenolate moftil hypertension diet plan vasotec 5 mg buy generic line. Direct immunofluorescence: Linear IgG fluorescence along the basement membrane is characteristic. Lesion: Group of thin-walled, delicate and short-lived clusters of multiple small vesicles which like herpangina rupture and type ulcers surrounded by inflammation. Marginal gingivitis: Classically gingiva seems erythematous, boggy and tender with broad spread vesicles and ulcers. Provocations: Some of the frequent precipitating factors are emotional stress, fatigue, fever, being pregnant or immune deficiency states. The site of affection is the vermilion border of the lip, skin vermilion junction and adjacent skin. Unusual presentation: Widely scattered vesicles and ulcers in affiliation with ache, tenderness and fever in adults. Lesions: Lesion begins on the interdental papillae and then spreads to free margins of the gingivae. Treatment: It consists of Systemic antibiotics which additionally cover the anaerobes (penicillin or erythromycin and metronidazole). Nutritional: Hematinic and other deficiency states similar to vitamin B12, folic acid and iron. Absence of vesicles and blistering and involvement of solely nonkeratinized mucosa differentiate it from herpes an infection. Topical application of steroids and cauterization with 10% silver nitrate help many patients. Major aphthous ulcers Less common (10%) More than 10 mm Posterior oral cavity/oropharynx Deep with sharp margins Usually single 6 weeks Very painful Present With scarring Herpetiform-type aphthous ulcer Least widespread (5%) Pinhead to 2 mm Wide unfold, not often keratinized mucosa Shallow crater type Multiple 7�10 days Moderate Usually absent Without scarring Frequency Size of ulcer Site of ulcer Type of ulcer Most widespread (85%) Up to 10 mm Nonkeratinized mucosa of anterior oral cavity Central necrotic space surrounded by red halo 7�10 days Moderate Usually absent Without scarring w Section four Number of ulcers Multiple Duration Pain Odynophagia Healing fig. It is usually associated with both herpes simplex an infection or drug ingestion (antiseizures and sulphonamides). Diagnostic function: Hemorrhagic crusts on the vermilion portion of lips with edema and severe tenderness are the distinctive characteristic. Mucositis of most cancers chemotherapy (such as methotrexate, 5-fluorouracil and bleomycin) manifests as erythema, edema and ulceration. Symptomatic therapy: Analgesics, oral hygiene, bland mouth rinses, topical steroids, antifungal, and anesthetics. Drugs like penicillin, tetracycline, sulfa drugs, barbiturates and phenytoin might trigger erosive, vesicular or bullous lesions within the oral cavity. About one-fourth of mucosal melanomas resemble benign lesions therefore biopsy becomes mandatory. Mucosal melanotic macule: About 10 mm macular zone of homogeneous hyperpigmentation with well-defined margins. Clinical Features: the extreme formation of keratin causes elongation of the filiform papillae on the dorsum of the tongue. Preexisting melanosis presents lateral spread or superficial spreading melanoma in adults. Lesion and its Site Well outlined, macular grayish-black focal often 4 mm dimension (1 mm to 1. Treatment: Thick important tongue tie needs transverse surgical release with vertical closure. Leukemia: Oral findings embrace pale mucous membrane, gingival hypertrophy and petechial hemorrhages. Other viruses, which might cause acute viral parotitis, are: coxsackie viruses A and B, enteric cytopathic human orphan virus, cytomegalovirus and lymphocytic choriomeningitis virus. Fever normally subsides earlier than the resolution of glandular edema, which can take several weeks. The peak incidence happens within the spring in temperate climates (little variation in tropics). The saliva from different glands (submandibular and sublingual glands) contains excessive molecular weight glycoproteins that competitively inhibit bacterial attachment to the epithelial cells of the salivary ducts. Painful swelling of the gland causes displacement of the pinna, otalgia, trismus and dysphagia. Usually one aspect parotid will swell first followed by enlargement of the opposite gland in 1�5 days. Complement fixing viral (V) antibodies towards outer floor hemagglutinin appear later than S antibodies and persist at low ranges for many years. Streptococcus pyogenes, Streptococcus viridans, Streptococcus pneumoniae and Haemophilus influenzae (communityacquired cases). Incision and drainage: In addition to the treatment of acute parotitis abscess wants incision and drainage. An anterior based mostly facial flap treatment chapter 36 remedy It begins with aggressive medical remedy and contains: Prompt fluid and electrolyte alternative, oral hygiene, reversal of salivary stasis and antimicrobial remedy. Salivary flow should be stimulated by sialogogues such as lemon drops and orange juice. Regular exterior and bimanual massage, starting from the distal mattress of the gland and working in the direction of duct drainage helps tremendously in drainage. Antimicrobial remedy, which could need change after the culture results, ought to be continued for 1 week after decision of symptoms. Antibiotics embrace augmented penicillin (Beta-lactamase producing bacteria in 75% cases) and antistaphylococcal penicillin or a first-generation cephalosporin, vancomycin or linezolid (for methicillin-resistant S. With blunt dissection and radial incisions in the parotid fascia abscess is drained. Rare problems are osteomyelitis, thrombophlebitis of the jugular vein, septicemia, respiratory obstruction and even death. Infections are either through oral cavity (most common) or blood borne (usually gram-negative bacteria). Fever, anorexia, irritability and failure to acquire weight are current in affected child. Recurrent parotitis of childhood is the second most common inflammatory salivary gland disease of childhood (8 months to sixteen years) after mumps. An acute inflammatory lesion with diffuse glandular edema: It may be confused with an acute sialadenitis or an abscess. Complete surgical excision: In cases by which the prognosis is unsure or the lesion is proof against medical remedy. Associated cervical lymphadenopathy is more commonly unilateral and positioned within the excessive jugular nodes or preauricular areas. Smears and stains for sulfur granules and the organisms: Needle aspiration of the mass or a fistula swab. Surgical excision is important to take away extensive fibrosis and sinus tracts, when antibiotics fail. Complete surgical excision of the involved salivary gland and nodes is the treatment of selection. It outcomes from cutaneous inoculation attributable to scratch trauma from a home cat.