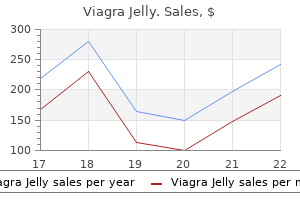
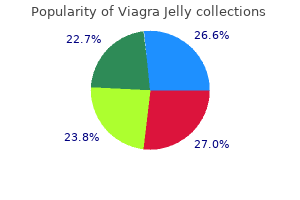
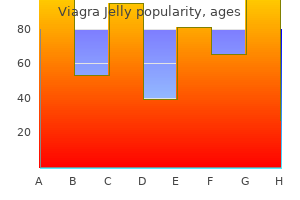
Viagra Jelly
Viagra Jelly dosages: 100 mg
Viagra Jelly packs: 10 pills, 30 pills, 60 pills, 90 pills, 120 pills

Viagra jelly 100 mg discount mastercard
Blunt dissection and entry point barely on the lateral side will forestall this complication erectile dysfunction urology tests cheap viagra jelly 100 mg otc. Nonunion Nonunion might happen as a result of erectile dysfunction zyrtec order viagra jelly 100 mg mastercard insufficient preparation of the joint, compression not achieved, Charcot joints, an infection and unstable fixation. This is the explanation for the location of dynamic locking screws in some of the newer nail designs. There is gross varus fracture website and ankle and nonunion in the metaphyseal space. If larger nail is used fracture may occur, intraoperatively or in the postoperative interval. Malunion Fusion could occur with varus, valgus or equinus deformity with extreme loading in some areas which can result in pain and ulceration. The failed screws should be removed and a model new screw is inserted within the dynamic gap. Neighboring Joint Arthrosis When each ankle subtalar joints are fused, midtarsal joints have extra mobility and excessive load is positioned on these joints. The therapy is to fuse the painful arthritic joints often the midtarsal joints. Osteomyelitis may have excision of all useless neurotic bone, gentle tissue and staged reconstructive procedures. In conclusion, simultaneous fusion of ankle and subtalar joints in a single stage is an efficient salvage process. For higher outcome, a great joint preparation, compression of fusion websites, proper positioning of the foot and secure fixation are key rules. Modern design of retrograde tibial nail appears to be a super implant, which is a load-sharing system and allows better positioning of the foot in relation to tibia and compression of fusion websites. Short-term outcome of retrograde tibiotalocalcaneal arthrodesis with a curved intramedullary nail. The success of tibiotalocalcaneal arthrodesis with intramedullary nailing-a systematic evaluate of the literature. Tibiotalocalcaneal arthrodesis utilizing a supracondylar femoral nail for advanced tuberculosis arthritis of the ankle, J Orthop Surg. Retrograde ankle arthrodesis utilizing an intramedullary nail; comparability of patients with and without diabetes mellitus. Neolithic man is thought to have survived amputation as evidenced from the skeletons with amputated stumps and from the knives and saws made of stone used at that time. Even the murals of La Tene and the drawings on the Peruvian pottery depict human figures with amputated stumps. In the olden times, amputations have been practiced not only for disease but additionally as a punishment for criminals and as rituals to appease Gods and even within the follow of Black Magic. It is taken into account that the first account of amputation as a purposeful medical process is found in the Hippocratic Treatise and it was concerned with amputation for vascular gangrene. Subsequent invention of tourniquet by Morel in 1674 made the job of surgeons simpler. With the introduction of anesthetics (nitrous oxide by Horace well in 1844 and ether by Morton in 1846) and antiseptics and subsequently asepsis, surgeons could refine the methods of amputation. The early amputations were of the guillotine type which slowly gave approach to the flap amputations. The modern idea of slicing pores and skin, muscle and bone at different levels was popularized by Benjamin Bell of Edinburgh. Better understanding of prosthetic wants has led to improved amputation strategies; higher engineering has led to better gadgets to replace human features. Incidence � Age-more frequent in 50�70 years of age � Sex- more in Men 75% � Lower limb > Upper limb. The control of bleeding was a significant drawback and early surgeons dipped the stump in boiling oil to safe hemostasis. Ambroise Pare (1536) improved the design of artery forceps and he was mentioned to be the primary to use ligatures for the control of bleeding after amputation. General Principles Indications Indications for amputations range based on availability of ability, amenities and line of remedy adopted. Many limb cancers are treated by amputations, but in some advanced centers limb preservation surgeries are accomplished. Although the designs and the usability of the prostheses proceed to advance, a well carried out amputation is important for optimum outcomes. Therefore, it could be considered as a "reconstructive" procedure, and ought to be deliberate and carried out as such. Characteristics Low power Injuries Stab wounds, simple closed fractures and small-caliber gunshot wounds Open or multiple-level fractures, dislocations and moderate crush accidents Shotgun blast (close range) and high-velocity gunshot wounds Logging, railroad and oil rig accidents Stable blood strain in subject and in working room Unstable blood pressure in field but conscious of intravenous fluids Systolic blood pressure <90 mm Hg in area and conscious of intravenous fluid only in working room Pulsatile limb with out indicators of ischemia Diminished pulses without indicators of ischemia No pulse on Doppler imaging, sluggish capillary refill, paresthesia and diminished motor exercise Pulseless, cool, paralyzed, and numb without capillary refill Score 1 Lack of Circulation Irreparable loss of blood provide of a diseased or injured limb is an absolute indication. In the presence of diabetes, tissues heal poorly and are extra vulnerable to an infection. The amputation can be early, intermediate or late relying on the timing after injury as shall be mentioned later in sort of amputation. Thermal burns, frostbite or electrical burns are other accidents that will require amputation (Table 1). Ischemia group 1 2 three None Mild Moderate 0* 1* 2* Limb Scoring Systems Mangled extremity score system is straightforward and predictive and preferable to other methods. Bony, delicate tissue, vascular and nerve injuries ought to be separately assessed and observe for a day or more, as the first assessment could also be unpredictable. Chronic osteomyelitis and/or contaminated nonunions that are immune to therapy are relative indications for amputation and prosthetic fitting as that is cheaper, will enhance operate in shorter time, and allow extra regular actions. Amputation and prosthetic becoming is an obvious indication for persistent infected trophic ulcer in an anesthetic limb where the part is functionally ineffective. Three components are related to cause diabetic gangrene: (1) Vascular insufficiency due to obliteration of vessels, (2) Neuropathy, (3) Infection which flourishes die to excessive sugar within the fluid. This could be an absolute indication of amputation Removal of an element or all of a congenitally irregular limb may be indicated if prosthetic fitting is prone to enhance the function. It ought to be documented in all circumstances of severe trauma or an infection, especially in these circumstances, which can require amputation in the future. A second opinion is immensely helpful particularly within the present era of increasing litigation should be thought-about. Late Amputation Symptomatic malunions, nonunions which have resisted all surgical efforts, and so forth. Amputation have to be carried out with great care and be considered a reconstructive process, just like complete hip arthroplasty (internal amputation of the hip joint) or mastectomy (amputation of breast) somewhat than an ablative process. This could also be: � Guillotine amputations where all the tissues from pores and skin to bone are reduce at the similar degree and the wound is left open for further administration. This is completed as an emergency to save life of patient in cases of gangrene, crushed limbs, etc. The accepted ideal stump lengths are 23�28 cm from larger trochanter in above-knee amputations, thirteen cm from the tibial articular surface in below-knee amputations, 10 cm above elbow in amputations by way of arm, and 17 cm from olecranon in forearm amputations.
Purchase 100 mg viagra jelly visa
The humeral model must be adjusted 5�10� away from the direction of dislocation erectile dysfunction causes natural treatment 100 mg viagra jelly purchase amex, i erectile dysfunction viagra free trials viagra jelly 100 mg buy generic online. The humeral prosthesis must be inserted such that the fin lies simply posterior to the bicipital groove. The humeral head offset measures from the geometric middle of the humeral head to the lateral fringe of the greater tuberosity. Preservation of this offset is important in sustaining the effectivity of the lever arm of the supraspinatus and deltoid. This is a more difficult task in an acute trauma setting as compared to an arthritic joint (Bunker et al. A limited objectives method must be followed and defined to the patient preoperatively such that expectations are real. An uncooperative patient with insufficient postoperative rehabilitation can result in lower than adequate results. The subacromial bursa should be excised taking care at occasions not to injury the axillary nerve as it passes round on the deep surface of the deltoid muscle. Capsular contractures need to be released: the anterior capsule launched from the glenoid, the inferior capsule launched from the humerus and the posterior and superior capsule incised. Bone grafting for a medialized glenoid would possibly help, although as a end result of poor bone quality, fixation is tough. However, several authors believe that preserving the humeral head is possible and thus has its deserves (Lee and Hansen, 1981; Kofoed, 1983). They counsel that though avascular necrosis does occur in these fractures, the humeral head is shortly vascularized by creeping substitution which prevents humeral head collapse. Primary arthroplasty is mandatory in head splitting or depressed fractures of the humeral head. They reported a great or satisfactory end in 80% of sufferers presenting with four half fractures. Whilst dissecting a varus head, one must watch out in not damaging the axillary nerve. The larger tuberosity very often malunites in a posterior and superior position. If left uncorrected, it would impinge and the rotator cuff can be dysfunctional (altered lever arm). The capsule or the cuff might be torn resulting in a high threat of postoperative dislocation. Late Presentation Technical considerations: Patients presenting late with fracture dislocations pose different problems. Malunion of the pinnacle to the shaft often requires a corrective osteotomy to restore the posterior and medial offset. Considerable progress has been made over the years in finding a correct prosthesis for such shoulders which current with nonfunctional/dysfunctional motor models (cuff muscles). Paralysis of both the deltoid and rotator cuff with full loss of function additionally excludes a shoulder arthroplasty. An irreparable rotator cuff is a relative contraindication to glenoid alternative. Preoperative Planning and Evaluation A cautious scientific analysis would include an in depth historical past and an assessment of the glenohumeral joint, acromioclavicular joint and the subacromial area. Joint stability ought to be assessed as unstable joints consequent to bone loss would most actually require grafting. Standard roentgenograms including a true anteroposterior view and an axillary view should be obtained. These views provide data relating to degenerative changes of the glenohumeral joint, humeral head elevation, tuberosity position, glenohumeral put on, subluxation and osteophyte formation. An axillary view could show posterior glenoid erosion, generally seen in osteoarthritis. Some surgeons prefer the anesthetic machine to be positioned at the foot end of the affected person. Patient Positioning Others Recurrent Dislocation Multiple episodes of dislocation cause severe injury to the pinnacle and glenoid. Hemophiliac Arthropathy Hematologic administration would finest be left to an experienced hematologist. The shoulder is positioned over the edge of the table such that extension of the arm is possible. The head is positioned over a hoop and a cap over the pinnacle helps hold the hair away from the surgical web site. The commonplace headrest portion of the table is replaced with a neurosurgical support. The anesthetist and the machine could presumably be positioned on the foot finish of the desk to create area for the assistant and preserve a sterile field. Gilpes retractors assist separate the subcutaneous fat and outline the deltopectoral groove along which the cephalic vein traverses. The cephalic vein is retracted laterally preserving the venae comitantes from the deltoid draining into it. The undersurface of the deltoid is freed from the subacromial bursa and rotator cuff. A tenotomy of the upper quarter of the pectoralis main tendon helps acquiring a great exposure of the head and glenoid. The anterior circumflex humeral artery is ligated and divided on the lower border of the subscapularis. The axillary nerve could be located beneath the strap muscles, close to the inferior margin of the subscapularis. This entails placing one finger on the undersurface of the coracoid, and then with a sweeping motion bringing the finger to the underside of the subscapularis, beneath the strap muscular tissues. Applying gentle rigidity beneath the anterior facet of the deltoid over the terminal finish of the axillary nerve with the other hand would produce a tugging sensation over the finger. Care is taken to avoid damaging the acromial insertion of the deltoid while working in this space. Stay sutures are positioned and a vertical incision is made through the subscapu laris and capsule 1 cm medial to its insertion. In sufferers with a preoperative inner rotation contracture, a Zlengthening of this tendon is most popular. The subscapularis is reflected medially and the incision continued by way of the inferior capsule the place it inserts into the humeral neck, maintaining clear of the axillary nerve. The humeral head is dislocated by externally rotating it and simultaneously releasing the inferior capsule from the humeral neck. Restoration of Joint Mechanics the Humeral Head Diameter the typical head dimension in cadaveric studies (Boilleau and Walch, 1992; Ianotti et al. Most prosthetic designs have a neck shaft angle of 45� which is integrated within the cutting jig. Inappropriate cuts may be accommodated whilst utilizing cemented prostheses through the use of a smaller stem in valgus/varus. However, uncemented or pressfit designs are unforgiving and a gap between the collar and shaft would be seen.
Buy 100 mg viagra jelly otc
A minimal 5-year follow-up of an oxidized zirconium femoral prosthesis used for total knee arthroplasty erectile dysfunction treatment boots order viagra jelly 100 mg line. Modular fixed-bearing whole knee arthroplasty with retention of the posterior cruciate ligament erectile dysfunction freedom book viagra jelly 100 mg cheap fast delivery. Progressive subluxation and polyethylene put on in whole knee replacements with flat articular surfaces. Randomised, managed double blinded trial of oxidised zirconium & cobalt chrome in 17. Posterior cruciate supplementing whole knee replacement using conforming inserts and cruciate recession. Total knee arthroplasty in patients with angular varus or valgus deformities of > or = 20 levels. A study of polyethylene and modularity points in >1000 posterior cruciate-retaining knees at 5 to eleven years. Factors affecting vary of movement in complete knee arthroplasty using excessive flexion prosthesis: A potential examine. Twenty-year evaluation of meniscal bearing and rotating platform knee replacements. Knee kinematics with a high-flexion posterior stabilized total knee prosthesis: an in vitro robotic experimental investigation. Range of movement in total knee arthroplasty: a potential comparison of high-flexion and standard cruciate-retaining designs. Does a mobile-bearing, highflexion design increase knee flexion after total knee alternative Do high flexion posterior stabilised total knee arthroplasty designs improve knee flexion All-polyethylene tibial elements are equal to metal-backed elements: systematic review and meta-regression. Tibial part designs in major whole knee arthroplasty: ought to we reconsider all-polyethylene part The Anatomical Graduated Component total knee alternative: a long-term analysis with 20-year survival evaluation. Cemented tibial component fixation performs higher than cementless fixation: a randomized radiostereometric research evaluating porous-coated, hydroxyapatite-coated and cemented tibial parts over 5 years. The long-term consequence of uncemented Low Contact Stress complete knee alternative in patients with rheumatoid arthritis: results at a imply of 22 years. The early outcomes of high-flex whole knee arthroplasty: a minimum of 2 years of follow-up. Long-term followup of anatomic graduated parts posterior cruciate-retaining complete knee alternative. The improvement of extensile approaches has significantly simplified the removal of solidly mounted elements with out compromising bone stock. Such exposures embrace extensor mechanism reflecting strategies both proximally by quadriceps snip or patellar turndown, or distally by tibial tubercle osteotomy. Alternatively, a femoral peel, an epicondylar osteotomy or a quadriceps myocutaneous method could additionally be required. There should be a low threshold to consider considered one of these specialized approaches throughout revision knee arthroplasty. In this setting, the extensor mechanism is usually at threat of disruption or avulsion, and the danger of periprosthetic fracture is increased. A broad publicity facilitates the protected extraction of elements, allows an correct assessment of any bone loss, and permits straightforward softtissue balancing and accurate positioning of the new elements. This has led to the development of extensile approaches involving the bone, the soft-tissues or both. These include extensor mechanism reflecting techniques such as the quadriceps snip, the patellar turndown, or tibial tubercle osteotomy, and ligament reflecting strategies such as the femoral peel or medial epicondylar osteotomy. The growth of those extensile approaches has simplified the publicity of the joint and the removal of the components with out compromising bone inventory or endangering the integrity of the extensor mechanism. There ought to be a low threshold to think about one of these specialized approaches within the planning of any revision knee arthroplasty. Preoperative Assessment Revision arthroplasty surgery requires cautious preoperative planning. The choice of surgical method is among the most essential parts of this plan. This demands a careful evaluation of potential pitfalls on all sides of the joint, the identification of solutions to those issues, and the provision of back up plans should there be any surprising intraoperative findings or problems. A carefully deliberate strategy will keep away from excessive delicate tissue devitalization, uncontrolled bone avulsions and extreme retraction and manipulation, all of which can result in periprosthetic fractures or poor implant positioning and fixation. Moreover, a managed delicate tissue release or osteotomy is extra easily repaired, and is extra more doubtless to present a steady rapidlyhealing reconstruction. A thorough historical past, bodily examination and acceptable imaging are crucial previous to revision knee arthroplasty. The alignment of the knee, the consequences of earlier surgery corresponding to tibial osteotomy or patellectomy, and the peak of the patella could well dictate the required method, significantly if earlier hardware has to be eliminated on the similar time. Preoperative radiographs will decide the size and fixation of all components with specific regard to the extent of the tibial cement mantle that will require a tibial osteotomy for access. Conversely, patella infera could counsel interstitial fibrosis; which can be a requirement for proximal advancement of the tibial tubercle. The common health and mobility of the pores and skin and capillary return at the wound edges ought to be inspected. If possible, the strategy should decrease further delicate tissue scarring by using previous healed incisions. Otherwise, the selection of publicity for revision of a failed knee arthroplasty is to a large extent influenced by the mobilization of the extensor mechanism. Knees with lower than 90� of motion have lost much of the elasticity of the quadriceps tendon and patellar ligament. Lack of mobility of the patella in the coronal plane also indicates scarring of the extensor mechanism. Obesity, scarring and a tight quadriceps mechanism contribute to excessive forces at the tibial tubercle. Infected knee replacements commonly have extensive scar formation which increases the stiffness of the delicate tissues4 and the danger of patellar tendon avulsion. This decision may be made intraoperatively, however should all the time be considered in preoperative planning so as to keep away from inadvertent avulsion of the patellar tendon throughout eversion of the patella. Poor quality skin may require preliminary gentle tissue enlargement or flap coverage which can be performed both earlier than revision surgical procedure or at the identical sitting. In all instances, the patella and its borders, the quadriceps tendon, the patellar tendon, the tibial tubercle and all previous scars must be recognized and marked preoperatively. In some cases, a new incision may be made if the previous pores and skin incisions prevent affordable access to the joint. Transverse scars could also be crossed perpendicular to the scar with minimal compromise of the junctional zone.
Order viagra jelly 100 mg otc
Total Elbow Arthroplasty the modern designs of total elbow alternative principally are of two varieties erectile dysfunction pumps cost generic viagra jelly 100 mg online, coupled or uncoupled designs gas station erectile dysfunction pills cheap viagra jelly 100 mg overnight delivery. The coupled designs are subclassified into constrained and semiconstrained/sloppy hinge varieties. It has got triangular humeral and quadrangular ulnar stems that are mounted with the help of bone cement contained in the medullary canals of respective humerus and ulna. Thus, humeral prosthetic stem and humerus become single assembly during forearm rotations, thereby, reduces pressure at humeral bonecement interface. The hinge elements are assembled together and screwed down with a main hinge screw and secured additional by a locking screw. The motion bearing floor of the main screw is easy and thinner in diameter than the inner diameter of the outlet of humeral hinge component. This supplies a niche between the movement bearing surfaces leading to partial articular contact throughout elbow motions, therefore minimal steel dust liberation. There is 7�10� varusvalgus laxity between the hinge elements, however limited axial rotation. The forces across the prosthesis are dissipated primarily to the surrounding gentle tissues, thus defending the bonecement prosthesis interfaces. They are indicated in salvage conditions, especially in cases of in depth bone loss across the elbow. In apply, they produce a quantity of issues like subluxations or dislocations of interprosthetic joint, misalignment, insecurity, loosening of prosthetic stem and triceps rupture. They are inbuilt varusvalgus laxity on the hinge section which permits dissipation of forces over the prosthesis to the surrounding delicate tissues-so less strain occurs at bonecement prosthesis interfaces. Among their issues an infection price averages 2%, late loosening and revision price common 5%. The metallic sloppy hinge prosthesis is designed to replace primarily posttraumatic ankylosed elbows; additionally relevant for other causes of ankylosed or unstable elbows. A pneumatic tourniquet is utilized to the higher part of arm and preoperative antiseptic preparation and draping accomplished, whereas the arm is kept over the chest. Exposure of medial facet of olecranon and coronoid course of is done by erasing and mobilizing the ulnar head of flexor carpi ulnar laterally together with the ulnar nerve. In the presence of preservation of forearm movements, radial head excision may be avoided. A subarticular Lshaped cut is made at the higher end of ulna preserving the insertions of triceps at the upper finish of olecranon course of posteriorly and brachialis on the anterior facet of coronoid course of. A comparability is made between the vertical peak of the hinge of the prosthesis and the amount of gap occurred between the minimize ends of humerus and ulna in the position of full extension and flexion. In the presence of inadequate gap because of contracture of muscles, resection of more bone from the lower finish of humerus is done to accommodate the prosthetic hinge. Reaming of humeral medullary canal is finished with the assistance of triangular humeral rasp. Size of the prosthesis stem is decided from snugly becoming dimension of its stems within the medullary canal of humerus and ulna. Very slender medullary canals of humerus or ulna are enlarged by electric drilling underneath Carm management, to forestall false passage of prosthetic stem. Carm control is effective throughout drilling, cementing and insertion of prosthetic stems. Final fixation of the prosthetic stems is completed by handbook pressurization and hammering with the assistance of special elbow impression. In posttraumatic flail elbow with loss of olecranon and detach ment of triceps insertion, the latter is reattached to the proximal ulna and adjoining soft tissues by Ethibond suture or stainless-steel wire suture passed via transverse drill hole made in the higher end of ulna after reaming its medullary canal previous to cementing the ulnar stem. In cases of old sideswipe injuries of elbow the place size of triceps muscles may be shortened, Zplasty of triceps could additionally be required for its reattachment to the upper part of ulna. The alignment of lock screw holes is additional confirmed by the lock screw hole probe as properly as by matching the longitudinal grooves over the medial face of the hinge. Heavy weight lifting or physically strenuous work with the replaced elbow have to be prevented. Results of Prosthetic Replacement of Elbow Results of Elbow Arthroplasty in Post-traumatic Ankylosis or Instability17,18 the sloppy hinge elbow arthroplasty supplied passable relief of ache in 83. In posttraumatic series, other semiconstrained design like CoonradMayo prosthetic substitute supplied vital reduction of pain in 76% cases in common 6 years followup. Suction drain is positioned across the prosthesis hinge and brought out medial to ulnar nerve. Muscles are stitched in both medial and lateral sides of the wound which is closed in layers. The five failures required removing of prosthesis however retained acceptable elbow perform as a result of periprosthetic fibrosis connecting the adjacent bone ends and reorientation of muscle balance. Mean ToTal elbow arThroplasTy pronation was 68�, supination 62� and increased arc of 22�. In later series of 10 patients with rheumatoid arthritis having ankylosis in seven and unstable elbows in three, sloppy hinge arthroplasty was done. Our sloppy hinge elbow replacement like different semiconstrained designs appears to be a viable proposition. Complications of Baksi Sloppy Hinge Elbow Arthroplasty Several issues were skilled throughout early part of studies, but with the expertise of improved surgical method, implant design and postoperative care the incidence of complica tions had been much less. Among the early complications, preoperative fracture olecranon process occurred in 1. Among the late problems of authentic sloppy hinge, aseptic loosening of prosthesis occurred generally around the humeral stem, rarely ulnar. Fixed flexion 10�30� (average 25�) deformity occurred at elbow in majority, breakage of humeral stem of prosthesis (1. Results of application of current version of sloppy hinge elbow prosthesis among sequence of patients studied since the yr 2004, confirmed no occurrence of radiolucent line or loosening around the humeral stem throughout last 8 years followup. Elbow erosion across the flanges of the stem was noted solely in two cases, and disassembling of prosthesis occurred in a single. In the presence of loosening in longterm followup, many elbows of our patients, retained passable elbow movements with the arm by the side of the physique or in abduction. Subsidence of the prosthetic stems within the presence of loosening allowed further approximation of bone ends for their anchorage by periprosthetic fibrous tissues occurred following possible minimal metal dust liberation guaranteeing stability. When prosthesis wanted removing, the adjoining bone ends have been approximated with Ethibond sutures passed transversely via drill holes of the adjacent bone ends and tied together in "figureof8" trend in front of them to ensure extra scarring. Good stability in sagittal plane and fair in coronal plane with arm in abduction was famous due to anchorage of bone ends by mature periprosthetic fibrous tissues and reorientation of muscle balance. Mobilisation of elbow by free fascia transplan tation with report of thirty one cases, Surgery, Gynecology and Obstetrics. Studies on bodily properties of a newly designed elbow prosthesis and its clinical analysis after its implantation. Sloppy hinge prosthetic elbow replacement for posttraumatic ankylosis or instability. Modification of Baksi sloppy hinge elbow to decrease the stresses at the humeral bonecement interface.
Buy viagra jelly 100 mg cheap
The bony surfaces are opposed erectile dysfunction rings viagra jelly 100 mg purchase mastercard, and compressed with either cancellous screws inserted percutaneously or with an exterior fixator erectile dysfunction doctor called 100 mg viagra jelly order. A 12 cm lengthy incision is made along the lateral margin of Achilles tendon starting distally at its insertion and extending proximally. Peroneal tendons are retracted laterally, whereas flexor hallucis longus, tibialis posterior and neurovascular bundles are retracted medially. Methods of Arthrodesis Intra-articular4 There are three methods commonly used to remove articular cartilage. Remove the cartilage from tibia and talus concentrically following the curve of each bone. Osteotomize the tibia perpendicular to its long axis with a large osteotome or oscillating noticed. This method permits correction of varus/valgus, however shortens extremity greater than first technique. Fixation Options External Fixation Charnley launched the idea of compression arthrodesis. Calandruccio triangular frame produces compression, controls motion in all three planes and is comparatively straightforward to apply. More current designs embody ring or round exterior fixators that make the most of tensioned wires rather than massive threaded pins, theoretically decreasing the incidence of pin tract an infection, whereas alignment may be changed as required. These frames are cumbersome for the affected person to use, require a great deal of affected person compliance for pin tract care and are expensive. Ankle is opened anteriorly, and dislocated utterly by plantar flexion of the foot. Two small bone levers are positioned behind lower finish tibia to protect tibial nerve and blood vessels. The bone is divided with hand saws 6 mm from articular floor, and 90� to lengthy axis of tibia. The reduce surfaces are placed in shut apposition, and an identical pin is handed by way of physique of talus parallel to first pin. Foot is saved elevated until postoperative swelling settles, and the patient is mobilized with crutches. At 5 weeks, the plaster and pins are eliminated, and a below-knee-walking plaster is applied and retained till union is sound usually up to 8�10 weeks. A suitable-sized sandbag underneath ipsilateral buttock is used to keep the place of the limb. A motorized burr, ideally a barrel-shaped burr, is used to prepare the subchondral surfaces. A standard anteromedial (medial to the tibialis anterior tendon) portal is used for the arthroscope, after skin incision and blunt dissection with small clip. An anterolateral (lateral to the extensor digitorum communis) portal is established in the same means. Care ought to be taken to not injure the lateral superficial peroneal nerve positioned subcutaneously. If there are difficulties in reaching posteriorly, normally more bone needs to be resected anteriorly. In contrast, the medial gutter is ready thoroughly over the entire of the medial malleolus. Punctuate bleeding from bone could be demonstrated with maximal suction on the power devices. The joint ought to be positioned in neutral flexion, 0�5� hindfoot valgus, and some degrees of exterior rotation compared with the contralateral aspect. For normal fixation, two preferably parallel guidewires are inserted from the posteromedial side of the tibia through stab incisions. Obtaining rigid fixation is the first priority; understanding compression is critical in obtaining an arthrodesis. However, compression screws may not provide adequate compression or rigid immobilization in patients with poor bone high quality. The current development towards internal fixation is an effort to circumvent the problems encountered with external fixation. Through lateral incision, distal tibial plafond is transected 2�3 mm proximal to articular cartilage proper angle to transverse axis of tibia to present a bleeding cancellous floor. The talus is then positioned on tibia with the knee flexed 90� and tibia vertical. Pin is left in place, and last position is evaluated for neutral, plantar versus On the operating desk, sterile wound dressings and a belowknee splint is utilized. From weeks 2 to 8 postoperatively, the affected person is allowed partial weight bearing in plaster. From postoperative weeks eight to 12, full weight-bearing in a removable boot is allowed. At 12 weeks if clinical and radiological control is judged satisfactory, full weightbearing with out safety is allowed. Patient got here to us after 8 months (late presentation); (C and D) Tibiotalo-calcaneal fusion was accomplished by cancellous lag screws dorsiflexion, slight hindfoot valgus and posterior translation and rotation. The pin is then retracted, and osteotomy is accomplished using the preliminary cut as a template. The 4 elements of position are now checked with tibia held vertical by the assistant and the knee flexed 90�. The plantar facet of foot is easiest to visualize and should be at right angle to the anterior aspect of tibia. Hindfoot valgus is greatest seen from the pinnacle side of the desk and once more it might be better to err on the aspect of valgus. Rotational alignment is judged from opposite side noting the connection of the first internet space to tibial tuberosity. Finally, translation of the talus posteriorly on tibia may be checked by palpation and direct visualization. First screw is started on anterior surface of the lateral talar body and is directed into the posteromedial tibia. Second screw started on the anterolateral floor of tibia directed into posteromedial facet of talus. Postoperatively, Robert-Jones compression dressings with a stirrup splint are utilized. A well-padded brief leg nonweightbearing forged is usually positioned on third postoperative day. Headlessscrews: Arthroscopic ankle arthrodesis is a longtime procedure within the therapy of severe ankle arthritis.

Yerbamate (Mate). Viagra Jelly.
- How does Mate work?
- Constipation, depression, urinary tract infections (UTIs), heart conditions, kidney and bladder stones, mental and physical tiredness (fatigue), chronic fatigue syndrome (CFS), fluid retention, headaches, low blood pressure (hypotension), weight loss, and other conditions.
- Are there any interactions with medications?
- Are there safety concerns?
- Dosing considerations for Mate.
- What is Mate?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96804
Purchase viagra jelly 100 mg without a prescription
Achilles Tendinitis An extra heel wedge of sponge rubber in the midsole space can be used to elevate the heel impotence natural supplements 100 mg viagra jelly order with visa. Metatarsalgia In metatarsalgia erectile dysfunction treatment duration cheap viagra jelly 100 mg without a prescription, a sponge rubber rocker backside insert within the midsole area of the foot is beneficial. Foot Orthoses Heel Wedges Used to handle rearfoot problems like fixed or functional hindfoot varus, valgus or equinus deformity. It additionally simulates effect of foot flat by simulating plantarflexion � Desirable characteristic in an orthosis that restricts plantarflexion. Heel Flares and Offset Heel Heel flare increases the width of heel on either medial or lateral facet. In offset heel, as well as the offset extends proximally and offers reinforcement or buttressing to the heel counter. It wraps round medial and lateral sides of foot with proximal trim traces inferior to malleoli along with provide plantar support and medial hindfoot posting. Orthosis holds the ankle at neutral or slight plantarflexion with a dorsiflexion cease preventing knee flexion. Limiting ahead rotation of tibia throughout stance maintains ground response vector anteriorly producing knee extension second. A rocker sole on the shoe facilitates smooth ahead movement of the body in mid and terminal stance. Anterior Shell Toe off Ankle Foot Orthosis these are created from carbon fiber composites. Electronic and microprocessor managed knee mechanisms use foot plate or tilt sensors to determine if the stance controls ought to be on or off. It permits the patient to safely negotiate uneven, ascending and descending surfaces and supply for stumble recovery. Clinical features of lower extremity orthoses, Elegan Enterprises, Oakville, Ontario, 1990. Stance Control Knee Ankle Foot Orthosis these have a mechanism to prevent knee flexion in stance however allow free knee movement in swing. The lock may be mechanical or electromechanical and the controllers are mechanical or electronic. Factors determining quantity and depth of physiological reactions to warmth are: � the level of tissue temperature: the suitable therapeutic range extends from 40�C to 45. Dosimetry: the therapist is guided by feeling of delicate warmth on the part of patient. Techniques of Application Condenser approach: the affected part of the affected person is saved between two capacitor plates. Condenser pads: the capacitor plates are flexible and are enclosed in rubber or plastic material. These are absorbed in tissues with high water content material and permit chosen heating of muscle. Noncontactapplicators-Types: A detector: Antenna with hemispherical reflector (diameter 9. Both produce beam with cross-sectional sample with highest intensity in the form of a hoop. Direct contact applicators produce vigorous responses with little stray radiation. If tissues are in parallel, higher present move happens in tissues with greater conductivity. If tissues are in series, the tissues with biggest resistance are heated most for the explanation that current flow is same via all. Areas the place subcutaneous fats thickness is minimum, a condenser applicator may be used to warmth deeper buildings. Inductivecoupling:Electrical conductivity of muscle is bigger than fat, so extra muscle heating happens. Standardsforequipment:Tissue substitutes have been developed from which particular absorption fee may be calculated. Equipment ought to be powerful enough to produce most likely an absorbed energy in tissues greater than 200 watts/kg. Propagation and Absorption of Microwaves in the Tissues Dielectric properties of the medium and specific resistance or conductivity are responsible for energy absorption. Tissues with excessive water content, such as musculature, and fluid media, corresponding to found within the eye or sweat beads, are prone to absorb extra microwave energy than bone. If objective is to heat complete joint, the joint ought to be exposed from all elements as in case of ultrasonic remedy. Tuning must be optimal after which output by way of machine is adjusted, otherwise small actions of patient may change impedance of circuit so that elevated present flow may happen. The publicity of stray radiation to the physiotherapist is controversial, and should be taken care of. Dosimetry: Vigorous effects may be produced with ahead energy on of the order of 50 watts, with a mean intensity of 500 mW/ cm2. To safeguard towards tolerance levels, ache ought to still be used as warning sign and vigorous responses must be prevented in absence of such a ache sensation. The ultrasound beam produced by therapeutic applicator is nearly cylindrical in shape, so, if the diameter of the transducer is small then the angle of divergence will be greater than whether it is giant. The "interference" or "close to subject" is the area of ultrasound beam extending from the applicator floor to the location of most distant depth maximum. In this area, the maxima and minima of the depth are situated near one another. Beyond this point, the beam has a extra uniform intensity and this space known as the "far" or "distant area". So, therapeutically applicator with radiating floor of 7�13 cm2 is most handy and effective for therapeutic utility. Physics: the waves are propagated in the type of longitudinal compression waves, so propagation is decided by presence of medium able to getting compressed. Gaseous cavitations: In the phase of rarefaction, the biological gases in the dissolved media come out to kind gasoline bubble which collapse on next part of compression. The gases which go in or come out depend on surface space of bubble which is extra in rarefaction. Thus, the gas that goes out in compression is less as in comparability with the gasoline goes within the bubble in rarefaction. Electrical and chemical phenomena have been described as results of gaseous cavitations. Mechanical destruction can also be produced when the cavities collapse or when the fuel bubbles develop massive sufficient to vibrate in resonance with sound waves. This prevalence of gaseous cavitations could be prevented by utility of exterior pressure of sufficient magnitude. The depth of penetration is outlined as that depth at which the depth drops to one-half of its worth at surface.
Syndromes
- Difficulty swallowing (dysphagia)
- Dietary changes
- Loss of memory that continues over time or gets worse
- Abdominal swelling (distention)
- Protein-losing gastroenteropathy
- Bleeding
- Vomiting
- A pink or purple color to the normally white part of the eye
Viagra jelly 100 mg cheap with mastercard
Therapy: Treatment consists of simple excision and is really helpful for symptomatic patients erectile dysfunction and icd 9 viagra jelly 100 mg on line. The overlying pores and skin is clean impotence for males order viagra jelly 100 mg mastercard, yellowish and infrequently shows an evident keratin-filled orifice. Definition: It is a rounded construction full of keratin debris, deriving from sequestration of proliferating benign epidermal or follicular keratinocytes inside the outer pores and skin layers, resulting in cyst formation and distension. Etiology: It could additionally be a late complication of traditional feminine genital surgery, a results of skin traumas, or a consequence of pilosebaceous duct obstruction. Vulvar epithelial inclusion cyst as a late complication of childhood feminine conventional genital surgery. The ulcers are often multiple, delicate, lined by a grayish material, and may be shallow or deep. Inflammatory inguinal adenopathy is usually unilateral and occurs in roughly 50% of sufferers. Definition: Chancroid is a sexually transmitted an infection characterised by necrotizing genital ulceration, which may be accompanied by inguinal lymphadenitis. Etiology: It is attributable to Haemophilus ducreyi, a small, Gram-negative, facultative anaerobic bacillus, which is transmitted sexually by direct contact with purulent lesions. Epidemiology: It is prevalent in Africa, the Caribbean basin and South-West Asia, and sporadically happens in the developed world, often associated with commercial sex work in metropolitan areas and associated to people returning from endemic international locations. Clinical course: In its early phases, small tender inflammatory papules, soon turning into pustules, could also be noticed at the web site of inoculation (vulva, cervix, and perianal area). Without therapy, ulcers could last weeks to months earlier than undergoing self-healing. Diagnosis: Combinations of clinical diagnosis and microbiological cultures are "gold standards" for the diagnosis of chancroid. Differential prognosis: Lymphogranuloma venereum, granuloma inguinale, herpes simplex, and syphilis. Therapy: Oral antibiotic therapy (erythromycin, azithromycin, ceftriaxone, and ciprofloxacin) is usually effective. Epidemiologic, medical, laboratory, and therapeutic options of an city outbreak of chancroid in North America. The preliminary lesion is a papule or nodule that arises at the web site of inoculation from 8 days to 12 weeks after sexual contact with an infected associate. The most commonly affected sites in girls are the labia minora, the pubis, the fourchette, and/or the cervix. The ulcers, that are commonly observed in the pores and skin folds, could also be tender or painless, gradually enlarge centrifugally and develop subcutaneous granulomas, often with out lymph node involvement. Rarely, a proliferative reaction ensues with the formation of huge, vegetating, hypertrophic, or verrucous lots, which may resemble genital warts. Dry ulcers may evolve into scarring plaques and be related to lymphedema and swelling. Definition: It is a continual sexually transmitted disease that leads to ulcerative, domestically destructive lesions. Etiology: the causative agent is Klebsiella granulomatis, a Gram-negative pleomorphic bacillus, formerly often known as Calymmatobacterium granulomatis, which is hypothesized to have low infectious capabilities because repeated publicity is usually necessary for scientific infection to happen. Epidemiology: this infection is endemic in tropical and subtropical areas (Western New Guinea, the Caribbean, Southern India, South Africa, South-East Asia, Australia, and Brazil), but very uncommon in temperate climates (Europe and North America). Abdominal visceral dissemination with fever, malaise, anemia, and weight reduction might happen. In the late levels of the illness, lymphatic native harm, leading to elephantiasis-like swelling of the exterior genitalia, is a frequent complication. Differential diagnosis: Chanchroid, lymphogranuloma venereum, herpes simplex, syphilis, and hidradenitis suppurativa. Therapy: Oral antibiotics (erythromycin, azithromycin, streptomycin, tetracycline, or doxycycline) for no less than three weeks or ampicillin for 12 weeks are standard therapies. Normally, the infection will start to subside within 1 week of treatment, but the full therapy period must be followed so as to minimize the possibility of relapse. Definition: Aphthosis is a benign, persistent, and relapsing inflammatory situation characterised by single or a number of painful, self-healing canker sores on the oral or genital mucosa. Oral and genital lesions might coexist, and this situation is named aphthosis main or bipolar aphthosis. Other medications which have been used for selected sufferers with refractory disease embody colchicine, pentoxifylline, levamisole, dapsone, thalidomide, immune suppressors, and biologics. Efficacy of tumour necrosis factor- antagonists in aphthous ulceration: Review of published individual patient data. Definition: It is a neutrophilic inflammatory dermatosis with distinctive medical manifestations. Etiology: the etiology is unknown, however most likely entails altered immunity, as advised by its frequent affiliation with systemic autoimmune ailments. Roles of defects in both humoral and cell-mediated immunological responses, as properly as neutrophil dysfunction (impaired phagocytosis), have been proposed. Epidemiology: It is found not often on the vulva and very few circumstances have been described in the literature, most of that are associated with an underlying disease. Biopsy is subsequently an essential step for the correct diagnosis and administration of pyoderma gangrenosum. Differential prognosis: Bacterial and mycobacterial infections, chronic ulcerative herpes, tertiary syphilis, gangrene, tropical ulcers, and deep mycoses. Therapy: the mainstay of treatment stays high-dose oral corticosteroids, though cyclosporine has additionally proven promising results. Other treatments which have been reported to show restricted outcomes include dapsone, sulfapyridine, sulfasalazine, clofazimine, azathioprine, cyclophosphamide, minocycline, intralesional steroids, chlorambucil, and hyperbaric oxygen. Topical tacrolimus and imiquimod symbolize interesting novel approaches to therapy. Surgical therapy within the form of debridement of the ulcer can exacerbate the situation and pores and skin grafts are frequently rejected. Effective administration of an underlying disorder usually seems to end in improvement. Friction and a heat and moist setting may favor maceration and the onset of pruritus, but most cases are asymptomatic. Predisposing factors embody obesity, diabetes, a scorching and humid climate, and profuse sweating. Differential diagnosis: Fungal infections, eczema, intertrigo, inverse psoriasis, seborrheic dermatitis, and acanthosis nigricans. Therapy: Topical therapy with antibiotics (erythromycin or fusidic acid) is normally efficient. Definition: Ecchymoses, contusions, and collections of partially clotted blood in the skin or mucosae. Straddle accidents are the most common unintentional feminine genital traumas, defined as a fall during which the subject straddles an object compressing the gentle tissue of the vulva between the item and the underlying bones of the pelvis. Differential diagnosis: Bruising can sometimes be a sign of physical abuse or reveal a bleeding dysfunction or pores and skin fragility. By contrast, in case of extreme trauma, instrumental investigations and surgery could also be essential.
100 mg viagra jelly trusted
Fixation is done by a retrograde nail or by two screws Indian tibia is smaller in diameter with a slender intramedullary canal erectile dysfunction gel treatment viagra jelly 100 mg discount mastercard. To go properly with the Indian tibiae erectile dysfunction kya hai purchase 100 mg viagra jelly otc, we have to have a nail with a smaller diameter within the midshaft of tibia, eight mm or 9 mm and a bigger diameter distally. The quick nail causes stress riser effect at the proximal end of the nail and may result in fracture. However, most preferred incision is over the lateral malleolus to the tip of fibula, curving distally across the sinus tarsi. The operation is carried out with the patient in supine place beneath tourniquet, often beneath epidural anesthesia. Guidewire placed in line; (B) Making the entry level; (C) Entry level of the neurovascular bundle in malleolus and turned anteriorly towards sinus tarsi Starting from some extent about 6 cm from the tip of the lateral malleolus and is curved anteriorly towards the sinus tarsi. A small medial incision is often required to put together the joint floor from the medial side to get hold of wonderful bone to bone contact. The fibula is osteotomized, fibulocalcaneal ligament reduce and the lateral malleolar fragment is reflected posteriorly. Posterior gentle tissue is preserved to preserve the vascularity of the fragment, which is used as a strut graft. For Indian sufferers 5� dorsiflexion is important for squatting for foiled objective. The osteotomies are modified to appropriate any deformities by calculating the closing wedges. Preparation of Joints Preparation of the joints for fusion is of paramount significance. Tibial plafond and talar dome are fastidiously resected to right the malalignment and different deformities such as varus, valgus, equinus and rotational malalignment by using a saw blade or osteotome. If the physique of the talus has been resected the calcaneus ought to be aligned with tibia. It is extraordinarily essential to place the guidewire in the actual position to prevent postoperative malposition. Sequentially reaming must be accomplished in order that the canal is about 1 mm bigger than nail diameter to prevent tibial fracture. The nail is assembled over the zig and gently hammered in, in order that the nail is a few millimetera inside the calcaneal surface to enable for compression. This is required as a outcome of when the fusion site is compressed, the nail protrudes out of the calcaneal floor. Some firms have arrangement for inner compression by internal fixation, by tightening the rod and in addition by exterior device. Lateral image should show the hole in the nail for anteroposterior calcaneal locking screw, above the inferior calcaneal floor. Finding Nail Insertion Point It is necessary to mark the start line for placement of the guidewire. To mark the place to begin for retrograde nail a line joining the information of between medial and lateral malleoli is drawn on the plantar floor of the foot. The guidewire ought to pass by way of the physique of the talus and thru the middle of the ankle. Nailing approach: A vertical incision is taken within the skin on the insertion point. An artery forceps is Calcaneal Screws Before inserting the calcaneal screw, place of the foot is checked for varus/valgus, flexion/extension of the foot. Calcaneal screw is inserted from the medial facet of tuberosity of calcaneus roughly parallel to the calcaneal weight-bearing floor, towards the calcaneocuboid joint. Compression is given manually or by internal/external compression device if out there. Second screw, the talar screw is passed from lateral side of the calcaneal tuberosity into the talar neck. This was treated with fusion of the ankle and subtalar joint by retrograde nailing. Note the distal fibular fragment is fixed to the tibia and talus with two screws Proximal Tibial Screws Proximally screw is inserted in the dynamic gap, to deal with any subsidence on the fusion website. The screw is implanted whereas holding the required rotational place of the ankle. Fibular Strut Graft the medial floor of osteotomized lateral malleolar fragment is decorticated and glued by two screws-one in the distal tibia and the other within the talus as a further stability. Retrograde nail is successful even in Charcot joints provided operation carried out meticulously observing the above-mentioned principles for successful end result. The strategy of realigning and stabilizing every joint was difficult because of lack of bone for fixation with plate or screws. For fusion of the ankle joint, subtalar joint actions should be fully absent. When the edema subsides, beneath knee plaster cast is given and no weight-bearing for 6 weeks. The main drawback is related deformities and joint instability which alter the load utilized to plantar floor of foot. The indications for surgery are deformities such as rocker backside foot, exostosis or bumps inflicting unequal loading of foot, ulceration and infection. For fusion every attempt should be made to achieve as inflexible an inside fixation as attainable. Study confirmed an excellent outcome and a high price of bony union with comparable complication rates. With new nail sorts and improvement in the surgical methods, the indications have expanded to include neuropathic circumstances, club foot and arthritis of ankle and subtalar joints. Dynamic proximal locking and longer nails are a couple of recommendations beneficial by authors in these studies. Note the swelling on both sides of the ankle; (B) Incision over the distal fibula extending toward the sinus; (C) Excised particles. Complication vary from hematoma, an infection, nonunion, malunion, arthrosis of adjacent joints and osteomyelitis. With fashionable prosthetic becoming techniques, a prosthesis can be fitted to any well-healed nontender stump. Determining the level of amputation requires an understanding of the trade-offs between elevated function with more distal stage of amputation and a decreased complication fee with a extra proximal level of amputation. Closed Amputation Where the flaps are customary and closed primarily at the time of amputation. Part of the limb removed Reamputation the limb is amputed at the next degree and flaps closed. Intermediate Amputation Where in an injured limb, the choice to amputate is taken after ineffective makes an attempt to get hold of a limb with cheap function. The final function of the limb thus salvaged, after numerous operations, extended hospitalization and large monetary prices, have to be weighed against the useful capabilities of contemporary prosthesis fitted after early amputation. The larger the level of amputation, the greater the vitality expenditure required for strolling, the walking speed of the person decreases and the oxygen consumption will increase (Table 3). Classification of closed and open wounds, peripheral pulsation and status skin are all evaluated.
100 mg viagra jelly generic free shipping
Proper place erectile dysfunction protocol book download viagra jelly 100 mg buy overnight delivery, gentle passive stretching and stump train prevent contracture erectile dysfunction treatment algorithm buy viagra jelly 100 mg cheap. Fixed contracture may have plaster solid and wedge resection of forged or surgical release of contractures. Postoperative Care After Treatment Postoperative care of amputations is essential. Surgeon might need assistance of a group which features a physical medicine-specialist, a physical therapist, an occupational therapist, a psychologist, and a social worker. All of the identical precautions are followed as for any main orthopedic surgical procedure, together with perioperative antibiotics, deep venous thrombosis prophylaxis, and pulmonary hygiene. Pain administration consists of the transient use of intravenous narcotics adopted by oral pain medication. Use of steady postoperative perineural infusional anesthesia for a quantity of days cut back analgesic dosage is replaces. Conventional soft concern dressing is replaced by inflexible dressing, consisting of plaster casts, which is applied on the end of the surgical procedure. Advantages of rigid dressing are: (1) Prevents edema, (2) protects the wound from bed trauma, 3) enhances early healing, (4) reduces postoperative pain and (5) permits early mobilization of the patient. Drains are removal after 2 days and the physiotherapy began with stump exercise to strengthen muscular tissues. Rigid dressing ought to be eliminated within a week but when the forged is free, patient has fever or extreme drainage inflexible dressing should be removed earlier and wound is inspected. If weight-bearing ambulation within the instant postoperative interval is anticipated, a true prosthetic solid ought to be utilized. A metallic pylon with a prosthetic foot is connected to the forged and correctly aligned for ambulation. For transtibial amputations, inflexible dressings prevent the formation of knee flexion contractures. The physiological advantages of upright posture and walking to the respiratory, cardiovascular, urinary, and gastrointestinal methods are essential. In most cases, the hospital keep could be decreased and the worth of care reduced accordingly. Finally, earlier definitive prosthetic becoming is feasible, and a higher percentage of patients are efficiently rehabilitated. The patient is instructed on tips on how to place the stump correctly while in mattress, whereas sitting, and while standing. The stump is elevated by raising the foot of the mattress, which helps to handle edema and postoperative ache. With transfemoral amputations, the affected person is cautioned against putting a pillow between the thighs or beneath the stump or otherwise preserving the stump flexed or kidnapped. These precautions are necessary to help stop flexion or abduction contractures. Complications Hematoma prevented by meticulous hemostasis at surgery, postoperative wound drainage and stump bandaging. Amputation ought to be at a degree of enough circulation; wants instant debridement and wound care. Painful Neuroma Prevented by permitting the nerve to retract, treated by ultrasonic therapy, surgical excision may be essential. Phantom limb: this is the feeling by the affected person of the presence of amputation limb. This is a standard phenomenon in almost each case and the phantom limb disappears sooner or later of time. This phenomenon may be prevented by correct therapy of nerves at surgery, myoplastic procedures and correct stump bandaging and stump workouts. It could disappear 3466 TexTbook of orThopedics and Trauma � Stump bandaging with maximal strain terminally and minimal pressure proximally prevents blood loss and terminal edema, reduces phantom sensation and produces good shape � Stump exercises started early � Stump hygiene and intermittent exposure to air to forestall skin diseases. A troublesome, painful phantom limb could be treated by analgesics, sedatives, stump exercises, native nerve blocks, differential spinal anesthesia or transcutaneous nerve stimulation. Back ache is common in amputees, which should be handled by routine backache management. Stump edema, skin ulceration and attainable an infection must be prevented and handled. Part 2: Amputations in Lower Extremity Amputations of decrease limbs are the commonest. Disarticulation Disarticulation offers length and good stump for end-weight bearing and is more suitable for prosthetic than transfemoral amputation. Amputation versus Limb Salvage or Reimplantation If the affected person has come early inside 6�8 hours, vascular reconstruction or reimplantation of separated part could be undertaken supplied vascular surgeon and good services are available. Stump A good stump is important for becoming a great prosthesis and higher rehabilitation (Table 4). The characteristics of an excellent stump are: (1) best size, (2) ideal form, (3) muscular and never flabby, (4) good muscle power, (5) no fixed deformity, (6) full and free actions at the joint above, (7) an infection free, (8) nonadherent incision scar, (9) absence of neuroma, and (10) bone end well lined by muscles. Type of stump Too quick stump Difficulty skilled Lack of leverage to move the bogus limb, in order that the stump slips out of the socket 1. Bonystump Give more padding (soft felt) inside the socket of the synthetic limb 6. This reduces the edema, prevents knee flexion contractures and protects the limb from external trauma and friction with mattress. The benefits are lowered ache, prevention of tibiofibular instability, the periosteal stay is covered over the distal end of the tibia and fibula. Although, newer socket designs and prosthetic knee mechanisms that present swing section management have lowered such complaints. Though conveniently a long anterior flap is used, in ischemic limbs lateral flaps are preferred to prevent flap necrosis. These amputees got prostheses with conventional aspect steels and joints, but the trendy approach is to use a "four-bar link knee unit". A B � In this degree, a long broad anterior flap is used, which is the same as the diameter of the knee. As the medial condyle is bigger, the medial flap can be suitably larger, by about 2�3 cm. The increased floor area of the distal metaphysic permits dissipation of loading pressures over the big floor space or the articular floor of the distal femur in disarticulation and distal tibia in Syme ankle disarticulation. Impact at heel strike is additional dampened by the mechanical characteristics of the metaphyseal bone and cushioned finish pad of gastrocnemius muscle (in knee disarticulation) orheelpad(inSymeankledisarticulation);(B)Indirectloadtransferused with transosseous amputation ranges through the femur or tibia. The femur is adducted in transfemoral ranges, and the tibia is flexed 7�10� to allow distribution of weight-bearing hundreds over the complete surface are of the bony platform, thus avoiding concentration of forces on the small surface area of the terminal bony stump which is composed of mechanically stiff cortical bone Source: Modified from In: Browner-Jupiter-Krettek-Anderson (Ed).