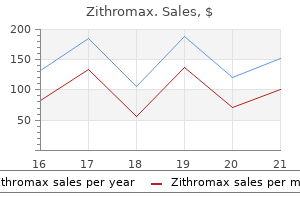
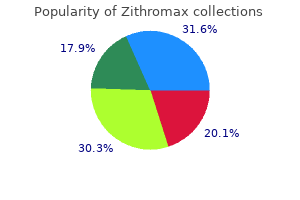
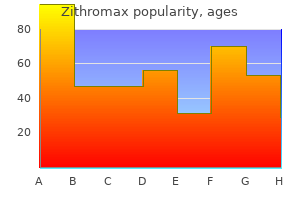
Zithromax
Zithromax dosages: 500 mg, 250 mg, 100 mg
Zithromax packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Discount zithromax 100 mg on-line
The two conditions may current with related signs including joint ache virus kills kid order 500 mg zithromax fast delivery, swelling sulfa antibiotics for sinus infection zithromax 100 mg generic, tenderness, and occasionally comparable laboratory findings similar to elevated white blood cell depend and sedimentation rate. Intraosseous tophi may have aggressive look and thus might simulate malignant bone tumor. On radiography, articular gouty erosions, notably affecting the proximal and distal interphalangeal joints, might sometimes mimic erosive osteoarthritis. Amyloid infiltrate of the articular structures may cause delicate tissue lots accompanied by cystic and erosive lesions indistinguishable from these of gout. Finally, it has to be identified that gout may coexist with other arthropathic situations corresponding to rheumatoid arthritis, osteoarthritis, and infectious arthritis. In addition, the drugs that block uric acid manufacturing, corresponding to xanthine oxidase inhibitors (allopurinol or febuxostat), and medications that enhance removal of uric acid from the physique (probenecid), are used to forestall problems of gout. Most lately, rheumatologists reported that urate-lowering therapy using pegloticase, a pegylated mammalian (porcine-like) recombinant uricase, resulted in reduction of the gouty tophus dimension both at subcutaneous websites and inside the joints. This consists of the risk of Stevens-Johnson syndrome in patients receiving allopurinol. A: Lateral radiograph of the knee of a 65-year-old man, who offered with proper knee ache, exhibits prepatellar delicate tissue mass eroding the anterior cortex of the patella. In addition, synovial, bursal, ligamentous, and tendinous calcifications are encountered. It rarely presents as a gentle tissue mass in extraarticular location, which is called tumoral or tophaceous pseudogout. The men and women are equally affected; mostly, patients are center aged and older. The disease may be asymptomatic, by which case the one imaging discovering may be chondrocalcinosis (see textual content below). Chondrocalcinosis, a situation in which calcification of the hyaline (articular) cartilage or fibrocartilage (menisci) occurs, may be seen in other problems as well, corresponding to gout, hyperparathyroidism, hemochromatosis, hepatolenticular degeneration (Wilson disease), and degenerative joint disease (Table 7. It shows distinctive imaging abnormalities similar to narrowing of the joint space, subchondral sclerosis, and osteophytosis, just like osteoarthritis. Calcium pyrophosphate crystals, the pathogens in pseudogout, range as a lot as 10 m in length. Pyrophosphate crystals are usually chunkier and sometimes show a line down the center. Pathologic findings encompass punctate or linear calcium deposits, often in the hyaline cartilage paralleling the subchondral bone end plate, additionally referred to as a "subchondral" or "articular" cortex. On microscopic examination, the chalky white deposits seem both crystalline or amorphous. The pyrophosphate crystals are distinguished from urate crystals by their rhomboid shape. A: Sagittal section of the femoral head shows chalky white deposits of calcium pyrophosphate dihydrate inside the articular cartilage. B: Radiograph of the specimen clearly demonstrates the calcific nature of the deposit. B: Histopathologic section of the specimen stained with von Kossa stain demonstrates the calcium deposits (black) (original magnification �1). Scanning electron photomicrograph of calcium pyrophosphate dihydrate deposits exhibits attribute rhomboidal crystals (original magnification �2400). The arthritic changes encountered on this condition are much like those seen in osteoarthritis. In the knee joint, typically, the femoropatellar joint compartment is affected to considerably larger degree then medial or lateral joint compartments. The differential prognosis ought to embody tumoral calcinosis, a disorder characterized by the presence of single or a number of lobulated cystic lots within the gentle tissues, usually close to the main joints, containing chalky material consisting of calcium phosphate, calcium carbonate, or hydroxyapatite. The calcified deposits fail to present a crystalline appearance when examined by polarization microscopy. In this situation, the plenty are painless and normally occur in youngsters and adolescents, a majority of whom are black. One of the hallmarks of this situation is chondrocalcinosis as proven on this Grashey view (A) of the proper shoulder of a 32-year-old throughout the hyaline cartilage of the humeral head (arrowheads), Merchant view (B) of the knees of a 40-year-old girl, within the hyaline cartilage of the patellae (arrows), and anteroposterior radiograph (C) of the left knee of a 51-year-old man inside the medial and lateral menisci. A 70-year-old lady offered with acute onset of pain in her right knee and was treated with colchicine for acute gouty arthritis with out aid of her ache. Anteroposterior (A) and lateral (B) radiographs of the knee show calcification of the hyaline and fibrocartilage. Capsular and tendinous calcifications are also apparent, in addition to narrowing of the femoropatellar joint compartment, a characteristic feature of this dysfunction. A: Dorsovolar radiograph of the right wrist of a 63-year-old man who presented with an acute onset of ache reveals chondrocalcinosis of the triangular fibrocartilage, cystic modifications within the scaphoid and lunate, and narrowing of the radiocarpal joint. B: Dorsovolar radiograph of the right hand of a 55-year-old lady reveals chondrocalcinosis within the triangular fibrocartilage advanced and radiocarpal joint (curved arrows), in addition to typical arthritic changes affecting second and third metacarpophalangeal and first carpometacarpal joints (arrowheads). Dorsovolar radiograph of each arms of a 60-year-old man exhibits typical for this situation arthropathy of the radiocarpal, metacarpophalangeal, and proximal interphalangeal joints. Anteroposterior (A) and radial head�capitellum (B) views of the best elbow of a 52year-old woman with pseudogout syndrome show chondrocalcinosis (open arrows) however no other alterations of the joint space. Anteroposterior (C) and external indirect (D) radiographs of the best elbow of a 57-year-old man, in addition to in depth chondrocalcinosis (arrows) show additionally early osteoarthritic-like changes of the radiocapitellar joint. A: Anteroposterior radiograph of the pelvis of a 61-year-old man shows chondrocalcinosis inside the hyaline cartilage of the femoral heads and within the fibrocartilaginous acetabular labra (arrows). Anteroposterior (A) and lateral (B) radiographs of the proper knee of a 58-year-old girl, whose knee joint aspiration revealed calcium pyrophosphate crystals, show chondrocalcinosis and marked narrowing of the femoropatellar joint. Anteroposterior (A) and lateral (B) radiographs of the best knee of a 67-year-old woman show intensive chondrocalcinosis of the fibrocartilaginous menisci (arrows) and superior arthrosis of the femoropatellar joint compartment. The arrows are pointing to chondrocalcinosis, and the curved arrow to calcification inside gastrocnemius tendon. Acute symptoms include ache, tenderness on palpation, and local swelling and edema. Imaging Features Radiographic options depend upon the location of involvement, but often cloudlike or dense homogeneous calcific deposits are seen around the joint and tendons. The most typical location is around the shoulder joint at the site of the supraspinatus tendon. Calcific deposits can migrate into the adjoining bone, into the adjacent bursa, or into the tendon extending along the myotendinous plane. Treatment Treatment of this situation includes software of shockwave remedy (using sound waves), acetic acid iontophoresis, and drugs such as corticosteroids and cimetidine. Occasionally, arthroscopic or open shoulder surgical procedure is required to remove the calcific deposits. However, it has to be confused that always the outcomes of the remedy are disappointing.
Buy cheap zithromax 100 mg on-line
Advance the tube alongside the right aspect of the oropharynx once the epiglottis is seen antimicrobial guide cheap zithromax 250 mg with mastercard. When the glottic opening (or even simply the arytenoid cartilages) is recognized infection vs virus generic 100 mg zithromax mastercard, move the tube through to a depth of about 5 cm past the cords. While the tube remains to be held firmly, take away the stylet, inflate the cuff, attach a bag-valve mask, and check the tube for placement utilizing the instant affirmation protocol given in the paragraphs that observe. Insert the bougie via the cords, and then slip the tube over the bougie and slide it down by way of the cords. If still having problem visualizing the vocal cords, the emergency care provider can take his proper hand and, using mild stress, manipulate the thyroid (laryngeal) cartilage to deliver the vocal cords into view. The disadvantages of this methodology are its relative problem, depending as it does on the appreciation of the intensity of the breath sounds of spontaneously breathing patients, the longer duration to obtain intubation, and the necessity for the patient to be respiration on his personal. It is a blind process and as such requires further ability and care to successfully perform correct intratracheal placement. Grasp the cally assisted intubation, this method is being used much less thyroid cartilage, and transfer the larynx round to better visualize incessantly. Guidance of the tube through the glottic opening is a question of you perceiving the intensity of the sound of the patient breathing out. You can, with some issue, guide the tube toward the purpose of maximum depth and slip it by way of the cords. You can hear and really feel the breath sounds higher with your ear positioned against the proximal opening of the tube. Emergency care providers must always be cautious and wear personal protective tools when performing this process. Preparing two tubes allows the immediate use of the second, extra rigid tube ought to the first plastic tube turn out to be heat with physique temperature, thus shedding its anterior curve. Displacing the tongue and jaw forward additionally might help in attaining placement as a end result of this maneuver lifts the epiglottis anteriorly out of the finest way of the advancing tube. With the bevel in opposition to the floor or septum of the nasal cavity, slip the tube distally by way of the most important naris. When the tube tip reaches the posterior pharyngeal wall, take nice care on "rounding the bend," and then direct the tube towards the glottic opening. Tenting of the skin on either facet of the prominence signifies that the tube is caught up in the pyriform fossa, an issue solved by slight withdrawal and rotation of the tube to the midline. Bulging and anterior displacement of the laryngeal prominence usually indicate that the tube has entered the glottic opening and has been appropriately positioned. At this point the patient, particularly if not deeply comatose, will cough, strain, or each. This could also be alarming to the novice emergency care supplier, who would possibly interpret this as laryngospasm or misplacement of the tube. The temptation could additionally be to pull the tube and ventilate because the patient might not breathe instantly. Holding your hand or ear over the opening of the tube to detect airflow may reassure you that the tube is correctly placed, and you might inflate the cuff and begin air flow. Confirm tube placement utilizing the immediate confirmation protocol listed within the following part. A face-to-face strategy (also referred to as the tomahawk method) has been described and used successfully. Using this technique, the emergency care supplier faces the affected person and normally utilizes the Macintosh (curved) laryngoscope blade. The emergency care supplier holds the laryngoscope in his hand with the blade end of the handle emerging from the thumb side of the fist, in order that the blade can "hook" the tongue. Preparation of kit is as previously talked about, including having mechanical suction instantly obtainable. This technique could be very effective with patients in a seated position, similar to one trapped in a motorcar. An unrecognized esophageal intubation is a lethal complication of this life-saving process. Every effort have to be made to avoid this disaster, and a strict protocol have to be adopted to cut back the chance. The emergency care provider should remain vigilant in noting the depth marking on the mouth or nostril and to continually reassess the tube to be positive that it has not moved or turn out to be dislodged. The emergency care supplier ought to perform ongoing confirmation of the tube placement and likewise document this on the suitable type. When you employ this protocol, you must acknowledge the unreliable nature of auscultation as the only methodology of confirming intratracheal placement. Correct intratracheal placement is indicated by the following preliminary indicators: � An anterior displacement of the laryngeal prominence is seen or felt because the tube is handed distally. Note: Phonation-any noise made with the vocal cords- is absolute proof that the tube is in the esophagus, and the tube should be eliminated instantly. The following process should then be carried out instantly to prove correct placement. Some studies have shown poor sensitivity with youngsters under one yr of age and with patients in cardiac arrest. Any time placement remains to be unsure despite the preceding protocol, visualize instantly or remove the tube. In cases of cardiac arrest, finest outcomes might be obtained if good compressions are being accomplished at the time the system is used. Capnography has many different uses in nonintubated patients, including perfusion monitor, airway monitor, and air flow monitor. In arrest conditions, good compressions must be carried out as the waveforms are being evaluated. A delay of 10 to 30 seconds for warm-up (depending on the monitor) will ensue should you wait to activate it after inserting the tube. For best results, have the capnography waveform default when the monitor is turned on. If the waveform is nonexistent or seems in gross and irregular waveform patterns, the tube is probably in the esophagus or hypopharynx. Listen for breath sounds midaxillary on each side to rule out right mainstem intubation. This permits continuous measurement and reduces threat of hypoventilation or hyperventilation. On arrival on the receiving facility, print out another waveform (if available) to prove right placement on the time of affected person switch. Hyperventilation (check the depth and price of ventilation) or hypoperfusion (shock, or loss of pulses). This may not be visible on the monitor, so it is necessary to print out the waveform. This represents the diaphragm beginning to get well from the results of a neuromuscular blockade. To lose a tube can be a disaster, particularly if the patient is quite inaccessible or the intubation was a difficult one to carry out.
Generic 250 mg zithromax
Vasoconstriction causes decreased blood flow to the probe website on the extremities virus 57 buy zithromax 250 mg line. If carbon monoxide poisoning is suspected antibiotic 5 day pack 500 mg zithromax cheap free shipping, you must use a particular monitor and sensor to measure ranges (see Chapter 16). Cyanide poisons at the mobile level stop the cells from utilizing oxygen to make energy. However, the affected person will nonetheless be dying from lack of oxygen (at the mobile level). Remember that although very helpful, the coronary heart beat oximeter is simply one other device to allow you to assess the affected person. Reasons to be used embody ease of placement as an preliminary superior airway intervention or as a backup system for failed endotracheal intubation makes an attempt. They are all designed to be inserted into the pharynx with out the necessity for a laryngoscope to visualize where the tube goes. It additionally was thought that by sealing the esophagus, extra air would enter the lungs, and ventilation could be improved. It is designed with an esophageal and pharyngeal cuff, which inflate concurrently. Unrecognized intratracheal placement of the tube is a rare but deadly complication that produces full airway obstruction. With the neck stabilized in a neutral place, hold the mouth open, and apply a chin lift with your nondominant hand. While bagging the affected person, gently withdraw the tube until ventilation turns into straightforward. Adjust cuff inflation if essential to acquire a seal of the airway at the peak ventilatory strain employed. Port #2 is barely shorter at the proximal finish and opens on the distal finish of the tube. With inflation of the distal and pharyngeal balloons, ventilation via port #1 leads to air exiting the aspect of the tube into the pharynx. When insertion of the tube ends in a tracheal place, port #2 is ventilated with air being directly delivered via the trachea to the lungs. Selection of the incorrect port for ventilating the patient will end in insufficient ventilation and oxygenation. Use of capnography to confirm airway placement and monitor position of the gadget is really helpful as a end result of auscultation and chest wall movement may be unreliable within the prehospital setting. Use the larger syringe to inflate the pharyngeal cuff with the suitable quantity of air for the size being utilized. Use the smaller syringe to fill the distal cuff with the suitable quantity of air for the dimensions being utilized. Extubation is prone to trigger vomiting, so be ready to suction the pharynx upon removing. There are varied other units obtainable that make the most of an identical method by putting a masks over the glottic opening. Cuff pressure should be checked periodically, especially if nitrous oxide is used. With the neck stabilized in a neutral position, ventilate with a mouth-to-mask or bag-valvemask approach. This may be achieved by urgent the masks with its hole aspect down on a sterile flat floor (Scan 5-1-1). Use the fingers to information the cuff into an oval shape and attempt to get rid of any wrinkles on the distal edge of the cuff. A utterly flat and easy forefront facilitates insertion, avoids contact with the epiglottis, and is necessary to guarantee success when positioning the gadget (Scan 5-1-2). Under direct vision, press the tip of the cuff upward against the hard palate and flatten the cuff against it (Scan 5-1-4). The black line on the airway tube ought to be oriented anteriorly toward the higher lip. Holding the tube will stop this movement and not allow a seal over the glottic opening. However, this affirmation methodology may be unreliable, so use of capnography to confirm and monitor tube place is beneficial. Extubation is prone to trigger vomiting, so be prepared to suction the pharynx and turn the backboard. Accumulating data from research suggests that intubation within the subject can in some populations worsen outcomes. The evaluation for a tough airway is the same as with intubation as is the preparation of the system, medications, rescue airway plan, and preoxygenation. Confirmation of the airway is finest achieved by use of capnography as described elsewhere in the text. Advanced Airway Management Preparation for Intubation Whatever the strategy of intubation used, both patients and emergency care providers ought to be prepared for the process. Protective gloves such as latex or nitrile inspecting gloves (not essentially sterile) ought to be worn for all intubation procedures. All sufferers ought to be ventilated by way of a bag-valve masks or should breathe high-flow oxygen (at least 12 liters per minute) for several minutes previous to the try, using both a face masks or by way of nasal cannula. This will "wash out" residual nitrogen in the lungs and reduce the danger of hypoxia during the intubation process. Completely take away the air, and go away the syringe filled with air connected to the pilot tube. The assistant might help maintain the pinnacle and neck in a impartial position or carry out exterior laryngeal manipulation to assist make the cords seen to the emergency care provider. Laryngoscopic Orotracheal Intubation For laryngoscopic orotracheal intubation, the higher airway and the glottic opening are visualized, and the tube is slipped gently by way of the cords. The advantages of this method include the power to see obstructions and to visualize the correct placement of the tube. It has the drawback of requiring a comparatively relaxed patient without anatomic distortion and with minimal bleeding or secretions. The tools wanted for a laryngoscopic orotracheal intubation contains the following: � Straight (Miller) or curved (Macintosh) blade and laryngoscope handle, all in good working order (checked daily), in multiple sizes including pediatric sizes. This does make it more difficult to visualize the vocal cords throughout laryngoscopy. An assistant stabilizes the top and neck, and counts slowly aloud to 30 (at your request). Push the tongue to the left, and "inch" the blade down alongside the tongue in an try to see the epiglottis.
Zithromax 100 mg buy generic on-line
The contralateral atypical mesothelial hyperplasia apparently adopted external beam irradiation what causes antibiotic resistance yahoo generic 100 mg zithromax free shipping. They proposed that tunica vaginalis mesotheliomas be categorized as "mesotheliomas of uncertain potential" antibiotic spacer zithromax 250 mg order fast delivery. There could also be "scattered foci of atypical mesothelial cells on the papillary surfaces" and "the minimal presence of mesothelial cells within the underlying stroma". Inflamed hydroceles additionally 1472 Chapter 36: Diseases of the pleura tend to present a definite zonation with cellular areas. These mobile areas lie near the luminal floor, having underlying fibrotic areas. The proliferating mesothelial cells in benign reactions typically kind parallel traces to the surface of the hydrocele. This may be mistaken for a yolk sac tumor, although the arborizing structure of the rete is retained and is diagnostic. Adenocarcinoma of the rete testis, epididymis and its appendix, papillary cystadenoma of the epididymis and metastatic cancer, especially from the testis, lung, prostate, biliary tract and pancreas, enter the differential diagnosis. Epithelioid mesothelioma has a hyalinized stroma, uncommon psammoma our bodies and no cilia, options that differ from serous papillary adenocarcinoma. There are small papillary epithelial lesions with psammoma our bodies and intraglandular papillary lesions. Ultrastructurally, the cells confirmed no well-developed microvilli or secretory granules. Cytology the diagnosis of malignant mesothelioma on cytological preparations can be each tough and difficult, because of the significant morphological overlap between benign and malignant mesothelial cells, and between mesothelioma and metastatic adenocarcinoma cells. Testicular mesothelioma Three main intra-testicular mesotheliomas are described,786 two presenting as intra-testicular masses. The tumors ranged from 5 to 15 mm and shaped intra-testicular lots with invasion of the tunica vaginalis. Mesothelioma cells in effusions are nearly at all times epithelioid, for the rationale that sarcomatoid/desmoplastic variant not often exfoliates into the serous cavities or causes effusions. Cytologists speak of low-power examination showing "more and larger mesothelial cells in more and larger clusters". Note the difference between the atypical morphology of the malignant mesothelial cells as compared to the conventional mesothelial cells (green arrowheads). The ancillary strategies mentioned above and correlation with radiology and clinical data improve sensitivity significantly. Mesothelioma coating the pleura, extending around the coronary heart, through the diaphragm and into the interlobar fissure. Macroscopic pathology Diffuse mesothelioma In a review of 4710 printed instances of pleural mesotheliomas, they have been commoner on the best side (right:left � 3:2). This research could have included some carcinomas or newly described pleural neoplasms, because it pre-dates the immunoperoxidase period. The distribution of both the nodules and pleural plaques follows the traces of the lymphatics, as would be expected from the work of Boutin et al. With development, nodules coalesce, fusing the 2 layers of pleura and obliterating the cavity. Tumor extends into and infrequently by way of the diaphragm, alongside the fissures and into underlying atelectatic lung. The underlying and/ or contralateral lungs now hardly ever present asbestosis in the West, due to more stringent health and safety measures. Pleural plaques could also be found either alongside the tumor or included into it but that is typically solely appreciated histologically. Chest wall invasion in addition to direct invasion of the pericardium, myocardium and mediastinum is common. Multicystic mesothelioma may have an result on the pleura in an identical approach to the peritoneal cavity, however is uncommon. This is best accomplished very carefully with a protracted, metal knife, which can bend around the rib cage. Mesothelioma involving the pericardium and epicardium, as properly as infiltrating the myocardium. Part of a myxoid mesothelioma containing gray mucoid material inside cystic spaces. Sarcomatoid mesotheliomas typically confirmed marked pleural thickening and lung encasement at post-mortem. Metastases are often via blood vessels, quite than lymphatics (see below), causing distant metastases more generally than their epithelioid counterpart. In addition in the mediastinum and lung hilum there are nodes, either surrounded by tumor or with white foci, that are more probably to be tumor, but histology must affirm this fact. Synchronous bilateral pleural tumors Synchronous bilateral pleural tumors are uncommon. In one other two, the tumors existed in contralateral hemithoraces and in two, pleural mesothelioma developed synchronously with an extrathoracic malignancy. In 6/9, the second tumor was a primary bronchial carcinoma (three adenocarcinomas, two squamous cell carcinomas and one small cell carcinoma). In the other three, the second tumor originated from the colon, pancreas and breast. Five cases had asbestosis (four bronchial carcinomas and one colorectal carcinoma). Two individuals with non-bronchial carcinomas had asbestos our bodies however no interstitial fibrosis. In two cases, the second neoplasms (primary pulmonary squamous and small cell carcinomas) had been related to diffuse interstitial fibrosis but no asbestos bodies had been seen on light microscopy. In every case, transmission electron microscopic mineral evaluation revealed an asbestos fiber burden within the background inhabitants range for controls. No mesothelioma was recognized preoperatively but was suspected, primarily based on the pleural sample of involvement. Mixed tumors have options of each, massive pleural effusions occurring as incessantly as with epithelial tumors, however survival is almost as poor as in sarcomatoid instances. Lymphangitic involvement of the lung parenchyma by diffuse pleural mesothelioma was present in 16% epithelioid, 5% biphasic and 32% sarcomatoid subtypes respectively. Epithelioid tumors gain access to the interlobar or intralobular septae and from there into lymphatics and hilar, mediastinal, supraclavicular or axillary nodes. Single and multistation nodal involvement was present in 20 and 24 instances, respectively. Epithelioid tumors behave as carcinomas, spreading by direct extension, large pleural effusions, contralateral pleural effusions, ascites and metastases in regional lymph nodes. There was no distinction in survival between skip N2 cases and either different N2 or N1 circumstances. The mechanism of unfold of the disease to hilar nodes may be through lung invasion and not as a outcome of direct spread from the pleura.
Discount zithromax 500 mg with mastercard
Anteroposterior (A) and lateral (B) trispiral tomograms of the cervical backbone in a 55-year-old woman with a 15-year historical past of rheumatoid arthritis present erosion of the odontoid process typical for this situation antibiotic for sinus infection discount zithromax 250 mg amex. Lateral radiograph of the cervical spine in a 34-year-old girl with juvenile idiopathic arthritis since age 20 reveals the everyday involvement of the apophyseal joints bacteria 2012 zithromax 250 mg cheap with visa. A: Lateral radiograph of the cervical spine of a 66-year-old man reveals narrowing of the several disk spaces of the decrease segment, osteophyte formation from the anterior and posterior elements of the vertebral our bodies, and narrowing and eburnation of the facet joints. B: Oblique radiograph of the lumbar spine in a 72-year-old woman exhibits narrowing and eburnation of the articular margins of the aspect joints, osteophytosis, and narrowing of the intervertebral disk spaces-a combination of the results of true side joint arthritis, spondylosis deformans, and degenerative disk disease. A: A lateral radiograph of the decrease lumbar backbone of a 33-year-old man exhibits early inflammatory changes manifesting by so-called shiny corners (Romanus lesion) (arrowheads) and squaring of the vertebral our bodies (arrows). Anteroposterior (A) and lateral (B) radiographs of the lumbar backbone in a 31-year-old man with advanced ankylosing spondylitis reveal the everyday appearance of "bamboo backbone" secondary to irritation, ossification, and fusion of the apophyseal joints associated with ossification of the anterior and posterior longitudinal ligaments, in addition to the supraspinous and interspinous ligaments. A: Lateral radiograph of the lumbar backbone in a 27-year-old man shows a single, coarse osteophyte/syndesmophyte bridging the our bodies of L1 and L2. B: Anteroposterior radiograph of the lumbosacral phase exhibits the consequences of the inflammatory course of on the sacroiliac joints (sacroiliitis). Distribution of the Articular Lesion Distribution of the lesions in the skeleton varies with the type of arthritis. Osteoarthritis tends to have a attribute distribution in the skeletal system. Typically, the big joints such because the hip and knee and the small joints of the hand and wrist are concerned, whereas the shoulder, elbow, and ankle are spared. Inflammatory arthritides, nevertheless, have completely different websites of predilection in the skeleton, relying on the precise variant of the illness. Rheumatoid arthritis, for instance, entails a lot of the large joints such because the hip, knee, elbows, and shoulders, and small joints of the hands and feet. In the cervical spine, the C1�C2 articulation and the apophyseal joints are regularly affected. Juvenile idiopathic arthritis, previously generally known as juvenile rheumatoid arthritis, has an identical pattern of distribution, except that the distal interphalangeal joints of the hand may also be affected. Psoriatic arthritis, in distinction to rheumatoid arthritis, has a predilection for the distal interphalangeal joints, in addition to the sacroiliac joints, resembling reactive arthritis in this respect. Erosive osteoarthritis, which some investigators consider a variant of osteoarthritis, others a variant of rheumatoid arthritis, and still others a definite form of arthritis, has a tendency to affect the proximal and distal interphalangeal joints of the hand. Use of a binary search sample and discriminator analysis in the radiologic prognosis of arthritis. A comparison of etanercept and methotrexate in sufferers with early rheumatoid arthritis. Effects of anakinra monotherapy on joint injury in sufferers with rheumatoid arthritis. Incidence and dimension of erosions within the wrist and hand of rheumatoid sufferers: a quantitative microfocal radiographic study. Reactive arthritis: outlined etiologies, emerging pathophysiology, and unresolved remedy. Combination antibiotics as a therapy for continual Chlamydia-induced reactive arthritis: a double-blind, placebo-controlled, prospective trial. A multicentre, double blind, randomized, placebo managed trial of anakinra (Kineret), a recombinant interleukin 1 receptor antagonist, in sufferers with rheumatoid arthritis handled with background methotrexate. Febuxostat: a selective xanthine-oxidase/xanthine dehydrogenase inhibitor for administration of hyperuricemia in grownup with gout. Abatacept for rheumatoid arthritis refractory to tumor necrosis factor alpha inhibition. Periarticular bone changes in rheumatoid arthritis: pathophysiological implications and scientific utility. Ustekinubab, a human interleukin 12/23 monoclonal antibody, for psoriatic arthritis: randomized, double-blind, placebo- controlled, cross-over trial. Clinical diagnostic standards for gout: comparability with the gold commonplace of synovial fluid crystal analysis. The pathogenesis of psoriatic arthritis and related nail illness: not autoimmune in spite of everything Cervical spine involvement in rheumatoid arthritis: correlation between neurological manifestations and magnetic resonance imaging findings. Sacroiliitis related to axial spondyloarthropathy: new ideas and newest tendencies. Treatment of rheumatoid arthritis with methotrexate alone, sulfasalazine, and hydroxychloroquine, or a mix of all three medications. Distribution of finger nodes and their affiliation with underlying radiographic options of osteoarthritis. Distinguishing erosive osteoarthritis and calcium pyrophosphate deposition illness. Anatomical location of erosions at the metatarsophalangeal joints in sufferers with rheumatoid arthritis. Role of metacarpophalangeal joint anatomic factors within the distribution of synovitis and bone erosion in early rheumatoid arthritis. Monosodium urate deposition arthropathy part I: review of the stages and diagnosis of gout. Discussion of those therapies is beyond the scope of this textbook, but you will want to note that the biologic medicine have a big potential to modify illness, reduce the systemic manifestations, and gradual the development of destructive changes within the joints. They do, nonetheless, carry vital unwanted side effects and have to be monitored on an everyday basis. For this purpose, we advocate that using such drugs be carried out by rheumatologist and not by household practitioners or internists, until a rheumatologist concurrently follows the affected person. In the past, remedy consisted of anti-inflammatory medicine and sometimes using allopurinol. However, a whole number of new medication have been introduced that modulate different ranges of uric acid metabolism, and here again, our advice is that such usage ought to be carried out by rheumatologists. Systemic glucocorticoids or intra-articular injections of steroids may additionally be beneficial. Because reactive arthritis is associated with an infection attributable to Shigella, Salmonella, Campylobacter, Yersinia, or Chlamydia trachomatis, acceptable antibiotic treatment ought to be administered if infection is energetic. Finally, we observe that despite intensive efforts at understanding cartilage repair and new bone formation, the remedy of osteoarthritis has remained unchanged. The major handicap is a late analysis of the disease, as a result of majority of the sufferers current to the medical amenities with the already advanced, nondiagnosed osteoarthritis lasted for years. There are already pathologic changes in cartilage water content and an age-related affect of normal tissue repair. These factors are superimposed, amongst others, on affect of weight problems, prior damage, and poor conditioning. Most patients with osteoarthritis can be managed by way of nonpharmacological and pharmacological remedy. The former contains education, weight administration, bracing, and applicable train with objective to delay the progression of the disease, alleviate symptoms, and improve perform.
Zithromax 100 mg visa
Osteonecrosis standard antibiotics for sinus infection zithromax 100 mg buy with visa, which is frequently seen antibiotic for uti 100 mg zithromax cheap with amex, has been attributed to problems of treatment with corticosteroids. However, current investigations counsel the vital role of the inflammatory course of (vasculitis) in the improvement of this complication. Note subluxations within the first carpometacarpal and metacarpophalangeal joints without articular erosions. B: In one other patient, a 32-year-old girl, the indirect radiograph of her left hand reveals dislocations on the first carpometacarpal joint and distal interphalangeal joint of the index finger (arrows) and subluxations in the metacarpophalangeal joints of the index and center fingers related to swan neck deformities (open arrows). B: On the dorsovolar projection, the flexion deformities have been corrected by the pressure of the palms towards the radiographic cassette. Dorsovolar radiograph of each arms shows severe deformities, subluxations, and articular erosions. Note the superior osteoporosis secondary to disuse of the extremities and therapy with corticosteroids. B: In another affected person, a 51-year-old girl, observe flexion contractions, subluxations, and dislocations in the a quantity of joints of the proper hand. Dorsovolar radiograph of the hand of a 29-year-old lady demonstrates sclerosis of the distal phalanges (acral sclerosis). Similar sclerotic changes are additionally often seen in rheumatoid arthritis and scleroderma. It is seen predominantly in young women, usually becoming apparent of their third and fourth a long time. Clinically, many patients develop joint involvement, which is manifesting as arthralgia and arthropathy resulting in flexion contractions of the fingers. Oblique radiograph (A) and lateral standard tomogram (B) of the ankle show osteonecrosis of the talus in a 26-year-old lady with lupus who was treated with large doses of steroids. Pathology shows symmetrical intimal thickening of affected arteries related to endothelial necrosis and telangiectasia of capillaries. Imaging Features Radiographically, scleroderma presents with attribute abnormalities of the bone and delicate tissues. Soft tissue calcifications throughout the higher and decrease limbs can sometimes be fairly prominent. Corroborative findings are seen within the gastrointestinal tract, where dilatation of the esophagus and small bowel, together with a pseudoobstruction sample, is attribute. A: A 24-year-old woman introduced with atrophy of the gentle tissues at the distal phalanges of the index, middle, and ring fingers (arrows). B: A radiograph of the fingers of the left hand of a 36-year-old lady reveals atrophy of the soft tissue at the tip of the index and center fingers (arrows) and early resorption of the terminal tufts (arrowheads). A: A 32-year-old woman with progressive systemic sclerosis reveals soft tissue calcifications within the distal phalanges of the best hand, a typical characteristic of this disorder. B: Dorsovolar radiograph of the arms of a 53-year-old lady reveals a quantity of foci of sentimental tissue calcifications. Oblique (A) and lateral (B) radiographs of the left foot of a 35-year-old man show calcifications of the delicate tissues of the distal leg and adjacent to the calcaneus. Patients with pulmonary hypertension, a complication of scleroderma, are treated with prostaglandin inhibitors to scale back wedge stress. They characterize issues of striated muscle and pores and skin and are characterised by diffuse, nonsuppurative inflammation, in addition to degeneration. Early analysis and subsequent management of sufferers with any sort of myopathy, together with polymyositis and dermatomyositis, could be facilitated by the use of appropriate laboratory tests. The four checks most helpful in evaluating muscle disorders embody (1) serum enzymes, (2) urinary creatine and creatinine excretion, (3) electromyogram, and (4) muscle biopsy. Further, the determination of serum enzyme levels and urinary creatine excretion is helpful for the medical administration of polymyositis and dermatomyositis, because the two tests present a broader perspective than either test alone. Antibodies directed against the chromatin-remodeling enzyme Mi-2 are found in about 20% of patients. Antinuclear antibodies have been present in about 50% of patients with polymyositis and dermatomyositis and were discovered to be associated with the presence of antibodies directed towards a nuclear protein Mi-2. A: Dorsovolar radiograph of the fingers of a 44-year-old lady reveals acroosteolysis (arrow), soft tissue calcifications, and damaging changes of the distal interphalangeal joint of the center finger. B: In another affected person, a 46-year-old woman, intensive gentle tissue calcifications are present around the elbow and the forearm. C: Calcifications are present in the soft tissues of the posterior facet of distal arm and proximal forearm on this 37-year-old lady. A positive biopsy could not solely show that the disease course of is myopathy, thus enabling the doctor to rule out a neurogenic decrease motor neuron lesion, but may determine these patients whose muscle illness is more severe pathologically than was suspected on clinical grounds. With assistance from histochemical and electron microscopic methods, muscle biopsy will sometimes enable the pathologist to diagnose one of many rare forms of myopathy that can clinically mimic polymyositis. Such ailments include sarcoid myopathy, central core illness, and muscle diseases associated with irregular mitochondria. A: Dorsovolar radiograph of the hands of a 50-year-old man shows harmful modifications within the distal interphalangeal joints, in addition to delicate tissue calcifications and resorption of the tip of the distal phalanx of the left middle finger. B: Dorsovolar radiograph of the palms of a 53-year-old girl with longstanding systemic sclerosis shows acroosteolysis of all distal phalanges. The pathologic adjustments discovered on muscle biopsy in polymyositis have been properly described. The degree of pathologic change may range widely; one affected person could present only negligible pathologic modifications in muscle fibers on biopsy outcomes, whereas one other affected person presenting related scientific options might show in depth necrosis and fiber alternative. This variability in histologic findings is probably liable for the frequent regular muscle biopsy outcomes from patients with in any other case classic polymyositis. The overall fee of positive findings from muscle biopsy in several research of polymyositis was in the vary of 55% to 80%. Clinical symptoms consist of symmetric muscle weakness, particularly within the proximal components of the extremities. Additional signs embrace arthralgias, myalgias, and severe fatigue; Raynaud phenomenon may also be encountered. Patients with dermatomyositis may present with cutaneous manifestations, including Gottron papules (raised violaceous lesions on the extensor surfaces of the elbows, knees, and the hands-particularly on the web site of metacarpophalangeal and interphalangeal joints) and heliotrope rash (red or purple discoloration of the eyelids). Less frequent, erythematous or poikilodermatous rash across the posterior neck and shoulders (the shawl sign) and on the anterior neck and chest (the V-sign) could also be noticed. Periungual telangiectasias and nail fold capillary changes similar to those seen in scleroderma also have been reported. Lateral radiographs of the left (A) and proper (B) elbow of a 50-year-old-woman show intensive calcifications of the muscles of the arm and forearm. Imaging Features Imaging abnormalities in polymyositis and dermatomyositis are divided into two types: these involving gentle tissues and those involving joints.
Buy 250 mg zithromax with amex
Guidelines of the European Respiratory Society and the European Society of Thoracic Surgeons for the management of malignant pleural mesothelioma antibiotics for acne minocycline 500 mg zithromax cheap with mastercard. Proposed adjustments to pathologic staging of epithelial malignant pleural mesothelioma based on analysis of 354 circumstances antibiotic resistance hospitals generic zithromax 100 mg mastercard. Pattern of spread to N2 lymph nodes predicts survival in sufferers with biphasic pleural malignant mesothelioma. Peritoneal most cancers and occupational exposure to 1551 Chapter 36: Diseases of the pleura asbestos: results from the applying of a job-exposure matrix. Lymph node dissection in major intrahepatic malignant mesothelioma: case report and implications for diagnosis and remedy. Primary pericardial mesothelioma presenting as pericardial constriction: a case report. National epidemiologic surveillance methods of asbestosrelated illness and the exposed workers register. Malignant pericardial mesothelioma following thoracal radiotherapy; dissemination from pericardium to pleura. Incidental localized (solitary) epithelial mesothelioma of the pericardium: case report and literature evaluation. Malignant lesions of the female genital tract and peritoneum that might be underdiagnosed. Metastatic neoplasms involving the ovary: a review with an emphasis on morphological and immunohistochemical options. The mortality of girls exposed environmentally and domestically to blue asbestos at Wittenoom, Western Australia. Mesothelioma of the tunica vaginalis: a sequence of eight cases with unsure malignant potential. Case report: malignant mesothelioma of the tunica vaginalis testis: an indolent course. Malignant mesothelioma of the tunica vaginalis testis: a case report and evaluate of the literature. A clinicopathologic analysis 1552 Chapter 36: Diseases of the pleura of eleven instances with review of the literature. Malignant mesothelioma of the tunica vaginalis testis: evaluation of the literature and evaluation of prognostic parameters. Immunohistochemical profile of paratesticular serous papillary adenocarcinoma and tunica vaginalis facilitates differentiation from malignant mesothelioma. The immunohistochemical profile of malignant mesotheliomas of the tunica vaginalis: a study of 20 instances. Well-differentiated papillary mesothelioma of the tunica vaginalis: a case report with aspirate cytologic, immunohistochemical, and ultrastructural studies. Well-differentiated papillary mesothelioma occurring within the tunica vaginalis of the testis with contralateral atypical mesothelial hyperplasia. Cysts and epithelial proliferations of the testicular amassing system (including rete testis). Selected different problematic testicular and paratesticular lesions: rete testis neoplasms and pseudotumors, mesothelial lesions and secondary tumors. Immunohistochemical proof for mesothelial origin of paratesticular adenomatoid tumour. Primary localized malignant biphasic mesothelioma of the liver in a affected person with asbestosis. Localized malignant mesothelioma of the epithelial kind occurring as a primary hepatic neoplasm: a case report with evaluation of the literature. Malignant mesothelioma of the pleura: relation between histological sort and clinical behaviour. Fine needle aspiration cytologic findings, clinical and radiologic features and review of the literature. Localized malignant peritoneal mesothelioma containing 1553 Chapter 36: Diseases of the pleura rhabdoid cells. Vacuolated cell mesothelioma of the pericardium resembling liposarcoma: a case report. Localised malignant pleural mesothelioma: a separate medical entity requiring aggressive native surgical procedure. Sarcomatoid localised mesothelioma mimicking intrapulmonary synovial sarcoma: a case report and evaluate of the literature. A clinicopathologic research of nineteen true mesothelial neoplasms, apart from adenomatoid tumors, multicystic mesotheliomas, and localized fibrous tumors. Synchronous diffuse malignant mesothelioma and carcinomas in asbestos-exposed individuals. The sample of lymph node involvement influences end result after extrapleural pneumonectomy for malignant mesothelioma. The case for routine cervical mediastinoscopy previous to radical surgery for malignant pleural mesothelioma. Prevalence and sample of lymph node metastasis in malignant pleural mesothelioma. Outcomes after extrapleural pneumonectomy and intensitymodulated radiation remedy for malignant pleural mesothelioma. Malignant peritoneal mesothelioma in girls: a examine of seventy five instances with emphasis on their morphologic spectrum and differential diagnosis. Malignant mesothelioma: a comparability of biopsy and postmortem material by gentle microscopy and immunohistochemistry. Diffuse malignant mesothelioma of pleura: diagnostic criteria based mostly on an post-mortem examine. Two malignant pleural mesotheliomas with uncommon 1554 Chapter 36: Diseases of the pleura histological options. Lipoblastic differentiation in a primary localized fibrous mesothelioma of the peritoneum. Mesothelioma with rhabdoid options: an ultrastructural and immunohistochemical examine of 10 cases. Malignant peripheral nerve sheath tumor of the pleura with epithelial and rhabdomyoblastic differentiation: report of a case clinically simulating mesothelioma. Primary epithelial malignant mesothelioma of the pericardium with deciduoid features: cytohistologic and immunohistochemical research. Loss of heterozygosity analysis defines a 3-cM region of 15q generally deleted in human malignant mesothelioma. Mucin-positive epithelial mesotheliomas: a histochemical, immunohistochemical, and ultrastructural comparison with mucin-producing pulmonary adenocarcinomas. Expression of calretinin, thrombomodulin, keratin 5, and mesothelin in lung carcinomas of different types: an immunohistochemical analysis of 596 tumors as compared with epithelioid mesotheliomas of the pleura. Immunohistochemical marker panels for distinguishing between epithelioid mesothelioma and lung 1555 Chapter 36: Diseases of the pleura adenocarcinoma. Expression of calretinin and other mesothelioma-related markers in thymic carcinoma and thymoma.
Purchase zithromax 100 mg with amex
Carpal alterations in adult-onset Still disease antibiotic prophylaxis zithromax 100 mg with visa, juvenile persistent arthritis antibiotics and probiotics zithromax 100 mg visa, and adult-onset rheumatoid arthritis: comparative examine. Comparison of scientific and ultrasonographic evaluation for peripheral synovitis in juvenile idiopathic arthritis. Magnetic resonance imaging is more sensitive than radiographs in detecting change in measurement of erosions in rheumatoid arthritis. Monotherapy with biologic disease-modifying anti-rheumatic drugs in rheumatoid arthritis. Sensitivity and specificity of the classification of psoriatic arthritis standards in early psoriatic arthritis. Interphalangeal osteoarthritis characterised by painful, inflammatory episodes, resulting in deformity of the proximal and distal articulations. A radiographic classification in juvenile rheumatoid arthritis applied to the knee. Magnetic resonance imaging of the craniocervical junction in rheumatoid arthritis: worth, limitations, indications. Diagnostic imaging of the occipito-cervical junction in sufferers with rheumatoid arthritis. Prognostic factors in juvenile rheumatoid arthritis: a case-controlled examine revealing early predictors and outcome after 14. Radiologic comparability of erosive polyarthritides with outstanding interphalangeal involvement. Radiographic development in rheumatoid arthritis: a long-term prospective study of 109 sufferers. The shared epitope hypothesis: an strategy to understanding the molecular genetics of susceptibility to rheumatoid arthritis. Reproducibility and sensitivity to change of 5 methods for scoring hand radiographic injury in sufferers with rheumatoid arthritis. Methotrexate monotherapy and methotrexate combination remedy with conventional and biologic disease modifying anti-rheumatic medicine for rheumatoid arthritis: a community meta-analysis. Sensitivity and specificity of plain radiographic features of peripheral enthesopathy at main sites in psoriatic arthritis. Magnetic resonance imaging of sacroiliitis in sufferers with spondyloarthritis: correlation with anatomy and histology. Monitoring anti-interleukin 6 receptor antibody treatment for rheumatoid arthritis by quantitative magnetic resonance imaging of the hand and power Doppler ultrasonography of the finger. Ultrasound detection of bone erosions in rheumatoid arthritis: a comparison to routine radiographs of the arms and feet. Comparison of clinical versus ultrasounddetermined synovitis in juvenile idiopathic arthritis. Systemic evaluation of irritation by magnetic resonance imaging in the posterior elements of the backbone in ankylosing spondylitis. Systematic evaluation of inflammation by magnetic resonance imaging within the posterior parts of the backbone in ankylosing spondylitis. Dynamic contrast-enhanced magnetic resonance imaging in the assessment of illness activity in patients with juvenile idiopathic arthritis. Magnetic resonance imaging, ultrasonography, and conventional radiography in evaluation of bone erosions in juvenile idiopathic arthritis. Erosive osteoarthritis and psoriatic arthritis: a radiologic comparability within the hand, wrist, and foot. It is time to rethink juvenile idiopathic arthritis classification and nomenclature. Comparison of medical, laboratory, radiographic, and scintigraphic findings in erosive and nonerosive hand osteoarthritis. Revision of the proposed classification criteria for juvenile idiopathic arthritis: Durban, 1997. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. Magnetic resonance imaging of bone destruction in rheumatoid arthritis: comparison with radiography. Common problems of synovium-lined joints: pathogenesis, imaging abnormalities, and complications. Use of the Sharp and Larsen scoring methods within the evaluation of radiographic progression in juvenile idiopathic arthritis. Classification standards for psoriatic arthritis and ankylosing spondylitis/axial spondyloarthritis. Macrophage activation syndrome: a potentially fatal complication of rheumatic problems. A reappraisal of intra-articular corticosteroid therapy in juvenile idiopathic arthritis. A radiographic comparability of erosive osteoarthritis and idiopathic nodal osteoarthritis. Rheumatoid arthritis: a practical information to state-of-the-art imaging, picture interpretation, and scientific implications. Reactive haemophagocytic syndrome in youngsters with inflammatory problems: a retrospective research of 24 patients. Magnetic resonance imaging of the wrist in rheumatoid arthritis: demonstration of development between 1 and 6 years. Rheumatoid arthritis of the hand and wrist: comparison of three imaging strategies. Extra-articular illness manifestations in rheumatoid arthritis: incidence, tendencies and risk factors over 46 years. Roentgenologic, immunologic and therapeutic examine of erosive (inflammatory) osteoarthritis. Epitope spreading of the anti-citrullinated protein antibody response happens before illness onset and is related to the disease course of early arthritis. Comparison of radiography, computed tomography and magnetic resonance imaging within the detection of sacroiliitis accompanying ankylosing spondylitis. Tophi, a pathognomonic characteristic of gout, usually type on strain points in and across the infected joints. Crystal deposits cause acute inflammation of the articular and paraarticular soft tissues, whereas recurrent acute intermittent flares can lead to continual gouty arthritis resulting in cartilage and bone destruction. Four levels of the illness have been recognized: asymptomatic hyperuricemia, acute gouty arthritis, intercritical gout, and continual tophaceous gout. The nice toe is the most common site of involvement in gouty arthritis; the condition known as podagra, which involves the primary metatarsophalangeal joint, occurs in ~75% of sufferers. Other regularly affected sites include the ankles, knees, hands, wrists, and elbows. Most patients are men, exhibiting the upper prevalence after the age of 65 years, but gouty arthritis is seen in postmenopausal girls as nicely (mento-women ratio being 20:1). In 25% to 30% of gouty patients, a main defect in the fee of purine synthesis causes extreme uric acid formation, as reflected in excessive urinary uric acid excretion (more than 600 mg/day) measured while the affected person is maintained on a regular purine-free food plan. Increased manufacturing can also be seen in gout secondary to myeloproliferative issues associated with elevated destruction of cells and end in increased breakdown of nucleic acids.