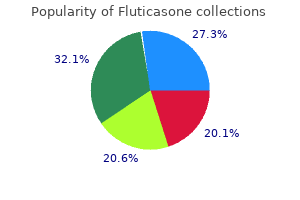
Fluticasone
"250mcg fluticasone overnight delivery, asthma treatment 1970".
B. Rendell, M.B. B.A.O., M.B.B.Ch., Ph.D.
Program Director, George Washington University Medical School
Seventy-seven percent of male and 61 percent of female American Indians/Alaska Natives are reported to be overweight and asthma treatment long acting beta agonist purchase fluticasone 250 mcg with mastercard, therefore asthma definition nz cheap fluticasone 250 mcg on line, at risk for diabetes and other illnesses asthma definition benign generic fluticasone 250mcg without a prescription. Age-adjusted death rates from diabetes mellitus among American Indians/Alaska Natives are nearly twice that for whites asthma symptoms rapid heart beat generic fluticasone 250 mcg. Exposure to local toxins is one source of health risks for American Indians/Alaska Natives. Of the more than 1,000 open dumps located on American Indian/Alaska Native lands identified in 1998, a third contained hazardous waste or waste that required special handling. The Alaska, Oklahoma and Phoenix service areas each had more than 100 open dump sites, while the Navajo service area had more than 200 open dump sites. Therefore, 20 percent of homes must use other means of waste disposal, including "honeybucket" methods in which waste is collected and disposed of in lagoons outside the bounds of villages or reservations. After heavy rainfalls, this waste and sewage can wash back into the community, causing contamination and infection. For example, in 2003, although the poverty income level, or threshold, for four-person families averaged $18,810, this average includes a threshold of $18,660 for a four-person family with two children and two adults along with a threshold of $19,289 for a four-person family with one child and three adults. Traditional gender roles (as hunters, horsemen, providers, and protectors) for many American Indian/Alaska Native males have been lost, as jobs have become scarce and opportunities to fish and hunt the land as their ancestors did are restricted on reservations. In addition, many American Indian/Alaska Native women are reluctant to report mistreatment by the men in their lives to non-Indian authorities because of the history of harsh treatment of American Indian/Alaska Native men by the U. American Indian/Alaska Native women often cope with prior victimization (from incest, rape, and other forms of sexual assault), often experienced in childhood or adolescence, by escaping into alcohol or drugs; doing so, though, contributes to higher mortality rates from alcohol- and drug-related causes. For the 19961998 period, mortality related to alcoholism among American Indian/ Alaska Native women ages 25 to 34 years was more than 23 per 100,000 population, in contrast to the 1 per 100,000 rate for women of all races. American Indian/Alaska Native women ages 45 to 54 had a mortality rate due to alcoholism of nearly 98 per 100,000 in 19961998, nearly 15 times the rate of their counterparts of all races. In the past, many addiction treatment programs were located outside of American Indian and Alaska Native communities and failed to incorporate healing elements from Native cultures. Though still true today, recently, more treatment programs have been developed close to or in American Indian and Alaska Native communities. These programs are tailored to the needs and cultural beliefs of American Indians and Alaska Natives and often incorporate elements of traditional medicine-such as talking circles, sweat lodges, and medicine wheels-into the services offered. Poverty, low self-esteem, alcoholism, and substance abuse often interfere with their ability to seek preventive health care. Some individuals with cancer are ostracized from their communities because of the belief that the person with cancer is contagious with the "cancer spirit. Screening facilities are often located far from communities, and the lack of culturally sensitive providers can discourage American Indians and Alaska Natives from returning for care. This distrust is due to a history of unethical medical research and health-related mistreatment by European colonizers in centuries past (whose use of smallpoxinfested blankets killed millions of American Indians) and by the Federal Government and its Indian Health Service in more recent times (that conducted experimental surgeries and performed unapproved sterilizations on American Indians as recently as the 20th century). More than 196,000 of the nearly 400,000 were women (both Hispanic and non-Hispanic). Additionally, Other Pacific Islanders were 19 percent of this population (71,978). In 2004, the Census Bureau estimated that more than 505,000 people in the United States identified themselves as Native Hawaiian or Other Pacific Islanders alone (both Hispanic and non-Hispanic). More than 248,000 (slightly less than half) of the 505,000 were women (both Hispanic and non-Hispanic). The United States maintains formal political associa tions with peoples from Polynesia and Micronesia, but not from Melanesia. An additional 6 percent lived in Washington, and 4 per cent each resided in Utah and Texas. Tongan Americans lived in Utah, many of them Mormon percent of Native Hawaiians or Other Pacific Islanders converts brought to the United States by missionaries. Guam, the most are more than one-third of the residents of Guam, developed of the islands in the western Pacific, has with Filipinos more than one-fourth, Chinese, Japanese, a relatively advanced system of health care. It has and Koreans together nearly 6 percent, and whites two hospitals-one that serves civilians and one that nearly 7 percent. Fourteen percent of the residents serves members of the military and their dependents. Due to the boost the tourism industry has recently the second largest Micronesian subpopulation is given its economy, Palau also has one of the best Marshallese (from the Republic of the Marshall Islands), health care systems, with a universal health care syswho numbered nearly 5,500 in 2000. A few satellite health clinics both natives and descendants of the Asian Indians who and private clinics also exist.
The rejection is provisional since the subject matter and the prior art are pending applications asthmatic bronchitis yogurt buy fluticasone 250 mcg visa. X is elected definition of asthma attack best 500 mcg fluticasone, a patent issues on X asthma symptoms 4dp3dt buy generic fluticasone 250 mcg, and a divisional No rejection of divisional application under 35 U asthma definition yahoo generic fluticasone 500 mcg on line. This form paragraph must be used in all Office Actions when a prior art rejection is made in an application with an actual filing date on or after March 16, 2013, that claims priority to , or the benefit of, an application filed before March 16, 2013. Patentability shall not be negatived by the manner in which the invention was made. Examiner Note: this paragraph must be used in all applications with joint inventors (unless the claims are clearly restricted to only one claimed invention. In bracket 2, identify the reason(s) why the disqualification attempt is ineffective. This paragraph is used to provisionally reject claims not patentably distinct from the disclosure in a copending application having an earlier U. If the claimed invention is fully disclosed in the copending application, use paragraph 7. If the claimed invention is not patentably distinct from the invention claimed in the copending application, a provisional obviousness double patenting rejection should additionally be made using form paragraphs 8. In bracket 2, insert the prior art reference(s) relied upon for the obviousness rejection. Considering objective evidence present in the application indicating obviousness or nonobviousness. Examiner Note: this form paragraph may be used, if appropriate, in response to an argument regarding the applicability of the factors for determining obviousness. When the reference teaches a product that appears to be the same as, or an obvious variant of, the product set forth in a product-by-process claim although produced by a different process. When the reference teaches all claim limitations except a means plus function limitation and the examiner is not certain whether the element disclosed in the reference is an equivalent of the claimed element and therefore anticipatory, or whether the prior art element is an obvious variant of the claimed element. If the interpretation of the claim(s) renders the claim(s) indefinite, a rejection under 35 U. For applications with an actual filing date on or after March 16, 2013, that claim priority to , or the benefit of, an application filed before March 16, 2013, this form paragraph must be preceded by form paragraph 7. Note that neither the filing of a request for continued examination, nor entry into the national stage under 35 U. Thus, a prior art disclosure could not be disqualified or antedated by showing that the inventor invented the claimed invention prior to the effective date of the prior art disclosure of the subject matter. This exception is not effective to except prior art that is also available under 35 U. These new provisions apply to any patent application that contains or contained at any time: (1) a claim to a claimed invention that has an effective filing date as defined in 35 U. If an application (1) contains or contained at any time a claimed invention having an effective filing date that is before March 16, 2013, or ever claimed 2100-355 Rev. These documents and activities are used to determine whether a claimed invention is novel or nonobvious. Evidence that the claimed invention was in public use, on sale, or otherwise available to the public may also be used as the basis for a prior art rejection under 35 U. Finally, a catch-all "otherwise available to the public" category of prior art is added. Note that the actual filing date of an application that entered the national stage under 35 U. Such documents and activities include prior patenting of the claimed invention, descriptions of the claimed invention in a printed publication, public use of the claimed invention, placing the claimed invention on sale, and otherwise making the claimed invention available to the public. There is an exception to this rule if the patent is secret as of the date the rights are awarded. In such situations, the patent is available as prior art as of the date the patent was made available to the public by being laid open for public inspection or disseminated in printed form. Although an invention may be described in a patent and not claimed therein, the grant date would also be the applicable prior art date for purposes of relying on the subject matter disclosed therein as "described in a printed publication," provided that the patent was made available to the public on its grant date.
Schick et al3 described a prospective comparative study assessing clinical differences between sequestrectomy and microdiscectomy asthma symptoms pregnancy purchase fluticasone 250mcg with amex. Use of an operative microscope is suggested to obtain comparable outcomes to open discectomy for patients with lumbar disc herniation with radiculopathy whose symptoms warrant surgery asthma treatment management cheap fluticasone 250mcg online. Grade of Recommendation: B Henrikson et al4 conducted a prospective randomized controlled trial evaluating whether microdiscectomy compared with standard discectomy would reduce the length of stay or postoperative morbidity in patients with lumbar disc herniation asthmatic bronchitis 8 weeks cheap fluticasone 500 mcg otc. Of the 79 patients included in the study asthma treatment cost cheap fluticasone 250mcg with mastercard, 40 were assigned to receive microdiscectomy and 39 to standard discectomy. Operative time was longer in the microdiscectomy patients (48 minutes versus 35 minutes, p<. The authors concluded that microdiscectomy does not shorten length of stay or influence postoperative morbidity. This study provides Level I therapeutic evidence that outcomes are similar between microdiscectomy and standard discectomy in patients with lumbar disc herniation. Tureyen et al5 described a prospective randomized controlled trial assessing outcomes of microdiscectomy versus macrodiscectomy. Microdiscectomy was defined as a small incision with flavum excision, use of scope and minimal bony removal. Of the 114 patients included in the study, 63 were treated with microdiscectomies and 51 received macrodiscectomies. Patients treated with microdiscectomy had smaller incisions and showed a statistically significantly greater improvement in muscle power, lower nar- There is insufficient evidence to make a recommendation for or against the performance of aggressive discectomy or sequestrectomy for the avoidance of chronic low back pain in patients with lumbar disc herniation with radiculopathy whose symptoms warrant surgery. Grade of Recommendation: I (Insufficient Evidence) Barth et al1,2 reported results of a prospective study comparing microdiscectomy with sequestrectomy in patients with lumbar disc herniation and radiculopathy. Self-rated assessment deteriorated over two years in discectomy patients but improved in sequestrectomy patients. The authors concluded that reherniation rates were similar two years after microdiscectomy or sequestrectomy. However, sequestrectomy was associated with a better functional outcome over time. The authors concluded that microdiscectomy allows more return to work and function with less narcotic use than open surgery. There is insufficient evidence to make a recommendation for or against the use of medial facetectomy to improve the outcomes for patients with lumbar disc herniation with radiculopathy whose symptoms warrant surgery. Grade of Recommendation: I (Insufficient Evidence) Abramovitz et al6 performed a prospective comparative study evaluating the indications for and efficacy of lumbar discectomy with or without facetectomy, stratified by preoperative risk factors. Outcomes were assessed at 12 months for the 740 patients included in the study, with three-month data available and presented for 533 patients. Use of the operating microscope improved outcome in patients with one to two predictors of favorable outcome but worsened outcome in patients with five to six predictors. The authors concluded that risk factors based on clinical examination and history can predict outcomes following lumbar discectomy. The meaning of these findings relative to the use of the operating microscope is speculative. Epstein et al7 performed a retrospective comparative study to determine and compare indications and benefits of varying surgical approaches to far lateral lumbar disc herniation. Of the 174 patients included in the study, 73 were treated with complete facetectomy, 39 with laminotomy with medial facetectomy and 58 with intertransverse discectomy. No difference in outcomes, defined as the percentage of patients with good or excellent results, was seen between the surgical treatment subgroups. The authors concluded that the three surgical procedures yielded near comparable outcomes in patients with far lateral disc herniations. Ryang et al8 described a retrospective comparative study comparing the efficacy of lateral transmuscular and combined interlaminar/paraisthmic approach to treat lateral lumbar disc herniation. Of the 48 patients included in the study, 28 were treated with a combined interlaminar/paraisthmic approach and 20 with a lateral transmuscular approach. Outcomes were assessed between 18 and 37 months using Ebling criteria and assessing pain in the lower back, along with consideration of radicular, sensory or motor deficits. There was a statistically significant improvement in overall excellent outcomes in the lateral transmuscular group. Even though 100% of back pain resolved in both groups, the patients treated with the combined approach had a 21% incidence of new back pain.
Diseases
- Illyngophobia
- Hypertrichosis retinopathy dysmorphism
- Brachymetapody anodontia hypotrichosis albinoidism
- Lymphedema hereditary type 2
- Oculodentoosseous dysplasia dominant
- Craniosynostosis contractures cleft
