Asendin
"Cheap asendin 50mg with amex, hyperinflationary depression definition".
By: N. Dawson, M.B. B.A.O., M.B.B.Ch., Ph.D.
Clinical Director, Cooper Medical School of Rowan University
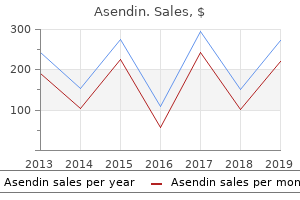
In choosing a type of treatment for a given patient anxiety keeping me from working generic asendin 50 mg without a prescription, clinicians often rely on their own experiences with similar patients (Pilkonis & Krause mood disorder young children discount asendin 50mg with mastercard, 1999) depression quest steam cheap asendin 50 mg amex. Effectiveness is assessed in nonresearch settings depression self evaluation test buy discount asendin 50 mg on-line, the place where most clinicians treat patients, without excluding them because of multiple diagnoses. By 40 40 definition, correlational studies of 30 30 treatment do not include random 20 20 assignment, nor do they have in10 10 dependent or dependent variables. Rather, a correlational research 0 5 10 15 20 25 30 35 40 45 0 5 10 15 20 25 30 35 40 45 study determines whether changes Therapy session Therapy session in one variable are associated with Among 10,000 patients with various psychological Examining data using a lower standard of changes in another variable. Another 25% attained clinically significant out able to function reasonably well despite their improvement by the 40th session. This association between dose and response is referred d 5 7 Th Dose-Response R l ti 5. More sessions are associated with a better outcome (Hansen, Lambert, & Forman, 2002; Shadish et al. In general, patients improve the most during the early phase of treatment (see Figure 5. However, people with more severe or entrenched problems, such as schizophrenia or personality disorders, may not show as much benefit in the early stages of outpatient treatment but rather tend to improve over a longer period of time. Because the dose-response relationship is correlational, it does not indicate whether the increased number of sessions causes the increased response. It is possible that people who are feeling better during the course of treatment are more eager or more willing to attend additional sessions than those who are not responding as well. If this were the case, the response would be "causing" the increased dose Percentage of patients Percentage of patients A curious finding invites speculation: People in the eastern part of the United States remain in treatment longer than those in the western part ("Fee, Practice, and Managed Care Survey," 2000). One possible explanation is that people in the eastern part have a different definition of "improvement"; that is, they continue in treatment until their symptoms have improved more than those of their counterparts in the western part of the country. For example, perhaps people who fare better as a result of treatment have more social support available in their lives, and these supportive individuals encourage them to continue treatment. Matching Patient and Therapist by Gender and Ethnicity All types of psychotherapy involve a relationship between two (or more) people. Therapists and patients may be similar with regard to racial or ethnic background and gender, or they may be different. However, with regard to gender, one study found that women and men are both less likely to drop out of treatment if they have a female therapist, although the study did not address the reason for this gender preference (Flaherty & Adams, 1998). Nevertheless, some people prefer a therapist with a similar ethnic or racial background to their own. For those with a strong preference, such as some Asian Americans, matching the ethnicity of the patient and therapist may lead to better outcomes (Sue, Zane, & Young, 1994), and it can result in lower dropout rates among non-Whites (Flaherty & Adams, 1998; Flaskerud & Liu, 1991; Fiorentine & Hillhouse, 1999; Sue, Kuraski, & Srinivasan, 1999). However, not all studies have reported this result (Arcia, Sanchez-LaCay, & Fernandez, 2002). Research on psychotherapy across different ethnic groups is complex, in part because of possible confounding factors. For instance, ethnicity is often associated with other demographic variables, such as socioeconomic status. In addition, research suggests that the more culturally assimilated a patient from a nonmajority ethnic group is, the less patient-therapist matching matters (Alvidrez, Azocar, & Miranda, 1996; Lamb & Jones, 1998). Finally, research on matching by ethnicity usually involves broad categories, such as patient and therapist who are both Asian American. However, when patients prefer a therapist from their own ethnic group, matching them with a therapist from a broadly similar group may not suffice. A Korean American patient, for instance, may prefer a Korean American therapist, but if such a therapist is not available, that patient may not prefer a Chinese American therapist over a therapist of any other background (Karlsson, 2005). Spencer Grant/Photo Edit Some patients prefer a therapist who shares their ethnic background, and this common background may make a patient less likely to drop out of treatment. However, such matching does not appear to produce better treatment outcomes (Beutler, Machado, & Neufeldt, 1994; Garfield, 1994; Lam & Sue, 2001).
As we discuss below depression symptoms hypothyroidism buy generic asendin 50mg line, this approach emphasizes the brain rather than the body (hence the neuro- in its name) and maintains that no factor can be considered in isolation depression exercise routine buy asendin 50 mg on-line. As psychologists and other scientists have learned more about the biological factors that contribute to psychological disorders bipolar depression symptoms test cheap asendin 50mg visa, the primacy of the role of the brain-and even particular brain structures and functions-in contributing to psychological disorders has become evident mood disorder odd buy asendin 50mg overnight delivery. Ultimately, even such disparate biological factors as genes and bodily responses. In addition, neurological, psychological, and social factors are usually involved simultaneously and are constantly interacting (see Figure 1. Hence, no one factor can be understood in isolation, without conneurological, psychological, and social factors sidering the other factors. For example, problems in relationships (social factor) interact with one another via feedback loops to contribute to the development of psychopathology. As you will see throughout this book, interactions among neurological, psychological, and social factors are common. Any of the types of factors can spark us to behave in a certain way or can help us control ourselves so that we do not behave in a certain way. In short, the neuropsychosocial approach can allow us to understand how neurological, psychological, and social factors-which affect and are affected by one another through feedback loops-underlie psychological disorders. In the next chapter, we will discuss the neuropsychosocial approach to psychological disorders in more detail, examining neurological, psychological, and social factors as well as the feedback loops among them. In that chapter, we will also continue our evaluation of the Beales and the specific factors that might contribute to their unusual behavior. Chapters 2 though 5 will provide you with knowledge to understand psychopathology in general: neurological, psychological, and social factors that contribute to psychological disorders (Chapter 2); issues related to diagnosing and assessing psychopathology (Chapter 3); treating psychological disorders (Chapter 4); and researching psychological disorders (Chapter 5). Chapters 6 through 15 address specific categories of psychological disorders (such as anxiety disorders). The final chapter (Chapter 16) discusses ethical and legal issues related to psychological disorders. As you will see in these subsequent chapters, the definition of a psychological disorder provided earlier in this chapter-a pattern of thoughts, feelings, or behaviors that causes significant distress, impaired functioning in daily life, and/or risk of harm-forms the basis for the definitions of specific disorders. However, we note in Chapter 3 and other chapters that the extent of distress, impaired functioning, and/or risk of harm that is required for a diagnosis of a psychological disorder is not always clear. Two individuals with psychological disorders are likely to have symptoms that reflect different locations on each continuum. Neuropsychosocial approach the view that a psychological disorder arises from the combined influences of neurological, psychological, and social factors-which affect and are affected by one another through feedback loops. Skinner spearheaded behaviorism, focusing on directly observable behaviors rather than unobservable mental processes and mental contents. They investigated the association between a behavior and its consequence, and proposed scientifically testable mechanisms to explain how maladaptive behavior arises. Behaviorism helps explain how maladaptive behavior can arise from previous associations with an object, situation, or event. Ivan Pavlov discovered and investigated what is sometimes referred to as Pavlovian conditioning-the process whereby a reflexive behavior comes to be associated with a stimulus that precedes it. Pavlovian conditioning helps explain the severe fears and anxieties that are part of some psychological disorders: Neutral stimuli that have in the past been paired with fear-inducing objects or events can subsequently, by themselves, induce fear or anxiety. The discovery of the biological cause of one type of mental illness-general paresis-led to investigations into possible biological causes of other types of mental illness. Although researchers investigate various biological and neurological abnormalities to understand psychopathology, exclusively biological explanations ultimately strip mental disorders of the context in which they occur and provide a false impression that mental disorders arise from biological (primarily neurological) factors alone. Psychological disorders cannot be fully explained by any single type of factor or theory. The biopsychosocial approach rests on the idea that both diathesis and stress can be grouped into three types of factors: biological, psychological, and social. As research on biological factors associated with psychological disorders has advanced, the important effects of the brain on other biological functions have become clear. The distress involved in a psychological disorder is out of proportion to the situation.
What determines the possession of assistive devices among patients with rheumatic diseases? The practice of physical and rehabilitation medicine in sub-Saharan Africa and Antarctica: a white paper or a black mark? In patient stroke rehabilitation efficiency: influence of organization of service delivery and staff numbers mood disorder in kids buy discount asendin 50mg online. Strengthening care for the injured: Success stories and lessons learned from around the world bipolar depression 24 trusted asendin 50 mg. Affordability bipolar depression 4 months order 50mg asendin otc, availability and acceptability barriers to health care for the chronically ill: longitudinal case studies from South Africa depression symptoms how long purchase asendin 50 mg on-line. The rehabilitation of hearing loss: challenges and opportunities in developing countries. Crossing professional and organizational boundaries: the implementation of generic rehabilitation assistants within three organizations in the northwest of England. The Journal of Rural Health: official journal of the American Rural Health Association and the National Rural Health Care Association, 2009,25:26-32. Retention policies for allied health professionals in rural areas: a survey of private practitioners. The development of rehabilitation services and suggestions for public policy in developing nations. Physical therapy roles in community based rehabilitation: a case study in rural areas of north eastern Thailand. The education of mid-level rehabilitation workers: Recommendations from country experiences. Personnel resources in physical therapy: an analysis of supply, career patterns, and methods to enhance availability. Community-based rehabilitation and orthopaedic surgery for children with motor impairment in an African context. Increasing access to health workers in remote and rural areas through improved retention: Global policy recommendations. Multidisciplinary perceptions of the role of nurses and healthcare assistants in rehabilitation of older adults in acute health care. The effectiveness of a sexuality training program for the interdisciplinary spinal cord injury rehabilitation team. Use of telerehabilitation to address sustainability of international service learning in Mexico: pilot case study and lessons learned. The effectiveness of cultural-competence training for health professionals in community-based rehabilitation: a systematic review of literature. Worldviews on Evidence-Based Nursing/Sigma Theta Tau International, Honor Society of Nursing, 2008,5:85-94. Cultural competence in the multidisciplinary rehabilitation setting: are we falling short of meeting needs? Staffing remote rural areas in middle- and low-income countries: a literature review of attraction and retention. Identification of recruitment and retention strategies for rehabilitation professionals in Ontario, Canada: results from expert panels. Motivation and retention of health workers in developing countries: a systematic review. Prosthetist/orthotist educational experience & professional development in Pakistan. Financial incentives for return of service in underserved areas: a systematic review. Exploring the barriers and enablers to attendance at rural cardiac rehabilitation programs. Factors shaping attitudes towards physical disability and availability of rehabilitative support systems for disabled persons in rural Kenya. The United Nations Standard Rules on the equalization of opportunities for persons with disabilities: government responses to the implementation of the rules on medical care, rehabilitation, support services and personnel training [Part 1. Barriers experienced by parents/caregivers of children with clubfoot deformity attending specific clinics in Uganda. Cape Town, Department of Physiotherapy in the Faculty of Community and Health Science, University of the Western Cape, 2006.
In addition severe depression gambling buy asendin 50mg on line, the results of a randomized anxiety scale 0-5 buy 50mg asendin mastercard, double-blind anxiety exercises buy asendin 50 mg without prescription, placebo-controlled trial (445) suggest that desipramine or amantadine treatment for depressed cocaine-abusing definition of depression in history generic asendin 50 mg amex, methadone-maintained patients may reduce cocaine use. Given the evidence to date, however, these treatments alone cannot be expected to reduce cocaine use in these patients and must therefore be accompanied by appropriate psychosocial treatment for a cocaine use disorder (1309, 1310). Comorbid general medical disorders A range of general medical conditions are associated with cocaine use, depending on the route of administration of cocaine. Intranasal use may cause sinusitis, irritation and bleeding of the nasal mucosa, and nasal septum perforation. Smoking cocaine is associated with respiratory problems, such as coughing, bronchitis, bronchospasm, and pneumonitis, resulting from irritation and inflammation of the tissues lining the respiratory tract (1320, 1321). Barotrauma such as pneumothorax, pneumomediastinum, and pneumopericardium may occur as a result of coughing or a Valsalva-like maneuver that is performed to better absorb the drug (1322, 1323). Treatment of Patients With Substance Use Disorders 109 Copyright 2010, American Psychiatric Association. Puncture marks and "tracks," most commonly in the forearms, occur in individuals who inject cocaine. General medical conditions independent of the administration route of cocaine include weight loss and malnutrition from appetite suppression, myocardial infarction, and stroke (657, 1225, 1324). Seizures, palpitations, and arrhythmias have also been observed in cocaineusing individuals. Although earlier studies suggested that cocaine use during pregnancy results in adverse effects on fetal development. The cocaine-exposed infants were significantly more likely to be premature and have smaller birth weight, length, and head circumference but showed no other major or minor anomalies to a greater degree than non-cocaine-exposed infants. They found that although all of the complications they examined (prematurity, abruptio placentae, low birth weight, prevalence of major malformations, premature rupture of membrane, and mean birth weight, head circumference, and length) demonstrated worse outcomes in infants who had been exposed to cocaine in utero than those who had not, only the risk for abruptio placentae and premature rupture of membrane remained statistically associated with cocaine use. Thus, although children of women who used cocaine during pregnancy did appear to have worse perinatal outcomes, this may have been due to other factors associated with cocaine or other substance use during pregnancy. The possible effects on early childhood development that have been reported in cocaineexposed newborns include hypertonicity, spasticity, convulsions, hyperreflexia, irritability, and inattention. However, the role of exposure to cocaine or other substances, poor maternal nutrition, birth prematurity, low infant birth weight, and neonatal withdrawal in the development of these signs and symptoms remains unclear (1330, 1331). A recent review of early child development after prenatal cocaine exposure (1333) systematically examined 36 studies on this subject and documented no independent effects of cocaine exposure on most measures of child development, although it did find that some reduction in attentiveness and emotional expressivity may occur. In addition, as stated above, many children of women who used cocaine during pregnancy have other risk factors that may affect their development. A clinician who is developing a treatment plan for a pregnant patient who is withdrawing from cocaine should take into account the risks and benefits to the mother and fetus in deciding about the use and choice of pharmacotherapies. When present, the concurrent use of other substances will also need to be addressed. Of these lifetime users, 314,000 individuals had used heroin in the previous year and 169,000 reported heroin dependence at some point in the previous year. This suggests that a high proportion (54%) of individuals who used heroin in the previous year were dependent on this opiate. These numbers are likely to be significant underestimates because of the difficulty in ascertaining community rates of heroin dependence; the Office of National Drug Control Policy estimates that 750,000 to 1,000,000 individuals are heroin dependent (1333a). Heroin is not the only opiate that is abused; there has been a growing awareness of misuse or "nonmedical use" of prescription pain relievers. Although a considerably lower proportion of individuals with past-year use were dependent on prescription opioid pain relievers compared with heroin (8% vs. Given the number of individuals who are using and are dependent on opiates, it is not surprising that the most commonly studied substance-related conditions, and those for which treatments have been most extensively studied, are opioid dependence, opioid abuse, opioid intoxication, and opioid withdrawal. Interventions include pharmacological treatments with agents such as methadone, buprenorphine, and naltrexone and nonpharmacological services such as behavioral therapies and counseling. The treatment of opioid dependence, in particular, is one of the most extensively researched areas in the field of addictions, and the range of available treatments is more extensive than for most other substance use disorders. Despite the number of effective treatments for opioid dependence and the scientific basis for their efficacy and safety, the availability of treatment programs for this and other illicit drug use is limited.
Purchase 50mg asendin. Mood disorders (depression mania/bipolar everything in between).