Lopressor
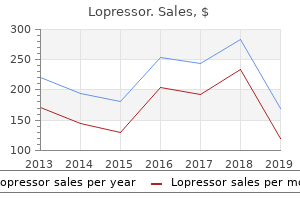
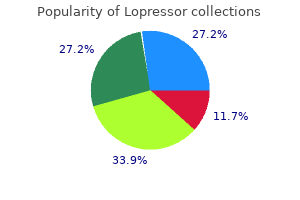
"Buy 12.5mg lopressor, hypertension drug".
By: A. Fasim, M.S., Ph.D.
Associate Professor, University of California, Merced School of Medicine
If a respondent has a disability arrhythmia flutter cheap lopressor 100mg visa, you must determine its severity and if it will prevent the respondent from completing in the interview hypertension vs preeclampsia discount lopressor 50mg. If the respondent has a person who can act as a proxy heart attack lyrics demi cheap 50 mg lopressor, you will need to secure their agreement to participate with the study respondent hypertension 2008 generic lopressor 25mg visa. Code the result appropriately and provide notes so that your supervisor can evaluate the case. Some of your calls will be with persons who have difficulty understanding your questions. Read questions slowly and distinctly and allow the respondent adequate time to answer. Repeat questions, if necessary, but be careful not to insult the respondent by suggesting that he/she does not understand. Some respondents will welcome the opportunity to talk to a neutral person about their health and family problems. You must know when to allow a respondent time to elaborate and when to re-focus him/her on the question. Some respondents will give answers that they believe you and/or the government expect; and they may expect you to help them with answers rather than give their own opinions or information. Some respondents may hesitate or decline to answer questions they consider intrusive or sensitive. Your professional handling of a sensitive issue can help to alleviate their fears. The more secure you feel about the confidentiality of the study, the more apt you will be to give a sense of security to the study respondent. However, if all else fails, you may simply offer them the option to decline answering a specific question. Encourage both family members and respondent to raise questions or concerns about the study. Encouraging them to ask questions, and your thorough and thoughtful responses to those questions, will help to alleviate their concerns. The interviewer should confirm the appointment with the respondent to avoid confusion Find an area where both you and the respondent can talk and write comfortably with minimal distractions. Make sure that the respondent understands the questions and that you are interpreting the responses accurately. Do this by restating what you think the respondent is telling you or asking him/her to restate the question you are asking. When the respondent strays from a question, try to use what he/she is saying to redirect the conversation back to the interview questions. If necessary, set time limits at the outset of the interview to encourage the respondent to stay on track. If necessary, read the interview questions to respondents who have visual impairments or limited reading ability. Communicate with other interviewers and the project director to share ideas about how to deal with difficult situations and to agree on consistent the following procedures are recommended for a successful interview: 2. If persons other than the respondent are present during the visit, address the respondent directly and do not encourage conversation with other parties. If necessary, ask that you and the respondent be left alone for a brief time to complete the questionnaire. Let the respondent know that you are willing to continue the interview after the interruptions are completed. Suggest that s/he call the number on the brochure for information and verification. Also point out that local health officials are aware of the survey, and offer to mail to the respondent a reproduction of newspaper clippings and/or endorsements. National Institutes of Health and local area health professionals to better understand the factors associated with heart and blood vessel diseases. We are doing an important research study and all the tests will be done free of charge. If applicable, remind that respondent that he/she was sent a letter about this selection process. Also explain that all information is held in strict confidence and that public reporting of the findings of this study will contain only statistical information.
Etiology the causes of hypophosphatemia include: decreased intestinal absorption (vitamin D deficiency prehypertension remedies buy lopressor 12.5mg without prescription, phosphorus-binding antacids heart attack or anxiety buy 25 mg lopressor overnight delivery, malabsorption); urinary losses (hyperparathyroidism 01 heart attack mp3 lopressor 50 mg free shipping, hyperglycemic states hypertension drugs lopressor 100 mg low price, X-linked hypophosphatemic rickets, oncogenic osteomalacia, alcoholism, or certain toxins); and shifts of phosphorus from extracellular to intracellular compartments (administration of insulin in diabetic ketoacidosis or by hyperalimentation or refeeding in a malnourished pt). The total body phosphate depletion cannot be predicted from the serum phosphate level; careful monitoring of therapy is therefore required. The clinical consequences of severe hyperphosphatemia are hypocalcemia and calcium phosphate deposition in tissues. Depending on the location of tissue calcifications, serious chronic or acute complications may ensue. Therapy consists of treating the underlying disorder and limiting dietary phosphorus intake and absorption. Oral aluminum phosphate binders or sevelamer may be used, and hemodialysis should be considered in severe cases. Hereditary causes include both disorders of absorption (rare) and those of renal loss. The most readily detectable clinical sign of hypermagnesemia is the disappearance of deep tendon reflexes, but hypocalcemia, hypotension, paralysis of respiratory muscles, complete heart block, and cardiac arrest can occur. Osteoporosis is a common condition in the elderly; women are at particularly high risk. In the United States, 8 million women and 2 million men have osteoporosis; an additional 18 million have osteopenia. Risk factors for an osteoporotic fracture are listed in Table 188-1, and diseases associated with osteoporosis are listed in Table 188-2. Preventive Health Services Task Force recommends that women age 65 and older be screened routinely for osteoporosis, and screening should begin at age 60 for women with increased risk. Criteria approved for Medicare reimbursement of bone mass measurement are summarized in Table 188-3. Risk factor reduction is a key part of management; smoking cessation and reduced alcohol intake should be encouraged; offending drugs should be discontinued or doses minimized. Moderate sun exposure also generates vitamin D, although recommending outdoor exposure is controversial because of concerns about skin cancer. Food and Drug Administration inhibit bone resorption, augment bone density, and decrease fracture rates. Long-term bisphosphonate treatment may be associated with atypical femur fractures; a tentative recommendation is to limit therapy to 5 years. Estrogen decreases the rate of bone reabsorption, but therapy should be carefully weighed in the context of increased risks of cardiovascular disease and breast cancer. It is indicated for treatment of severe osteoporosis and is administered as a daily injection for a maximum of 2 years. Teriparatide therapy must be followed by antiresorptive agent therapy to prevent rapid loss of the newly formed bone. Osteomalacia can also be caused by long-standing hypophosphatemia, which can be due to renal phosphate wasting. Proximal muscle weakness is a feature of vitamin D deficiency and may mimic primary muscle disorders. A decrease in bone density is usually associated with loss of trabeculae and thinning of the cortices. With advancing osteomalacia, hypocalcemia may develop due to impaired calcium mobilization from undermineralized bone. The lipoprotein phenotype is designated according to the Fredrickson classification. Cholesterol absorption inhibitors and bile acid sequestrants or nicotinic acid may also be required (Table 189-2). When chylomicrons are present, a creamy layer floats to the top of plasma after refrigeration for several hours. Tendon xanthomas and xanthelasmas do not occur with isolated hypertriglyceridemia, but eruptive xanthomas (small orange-red papules) can appear on the trunk and extremities and lipemia retinalis (orange-yellow retinal vessels) may be seen when the triglyceride levels are >11.
Lopressor 12.5 mg low cost. 5 Best Blood Pressure Monitor | Best Blood Pressure Monitors Reviews | Top 5 Blood Pressure Monitors.
As with more traditional approaches arrhythmia treatment buy cheap lopressor 100mg online, the results of these types of strategies are inconclusive arteria opinie 2012 effective 50mg lopressor. More research is needed to specify the conditions under which such interventions are effective hypertension workup purchase 50mg lopressor with amex. Several more biological approaches to rehabilitation have shown promise when implemented in animal models pulse pressure emt cheap lopressor 25 mg fast delivery, including methods to stimulate regeneration or reorganization of brain structure. In humans, pharmacological agents have been used to mitigate the effects of brain trauma. Can we learn more from word fluency measures with aphasic, right brain-injured, and closed head trauma patients? A developmental deficit in short-term phonological memory: implications for language and reading. Auditory and visual word-stem completion: separating data-driven and conceptually driven processes. Factors affecting excitatory amino acid release following severe human head injury. Contribution of surface and conceptual information to performance on implicit and explicit memory tasks. An individualized memory retraining program after closed head injury: a single-case study. Knowing the meaning, getting the point, bridging the gap, and carrying the message: aspects of discourse following closed head injury in childhood and adolescence. Spatiotemporal maps of brain activity underlying word generation and their modification during repetition priming. Volume of focal brain lesions and hippocampal formation in relation to memory function after closed head injury in children. Posttraumatic amnesia as a predictor of outcome after severe closed head injury: prospective assessment. A comparison of "errorless" and "trial-and-error" learning methods for teaching individuals with acquired memory deficits. Procedural memory during posttraumatic amnesia in survivors of closed head injury: implications for rehabilitation. Functional anatomy of neuropsychological deficits after sever traumatic brain injury. Which California Verbal Learning Test factors discriminate moderate and severe head injury from normals? Evidence for cellular damage in normalappearing white matter correlates with injury severity in patients following traumatic brain injury. Computer-assisted instructions for patients with traumatic brain injury: teaching of domain-specific knowledge. Facilitation of memory performance through induced semantic processing in survivors of closed head injury. Priming across modalities and priming across category levels: extending the domain of preserved function in amnesia. Word fluency generation skills of head-injured patients in an acute trauma center. Effects of brain injury and age on prospective memory self-rating and performance. Contributions of phonological and semantic short-term memory to sentence processing: evidence from two cases of closed head injury in children. A brief survey of the management of memory disorders in rehabilitation units in Britain. Cognitive and psychosocial outcome following moderate or severe traumatic brain injury. Categorization in aphasia: access and organization of goal-derived and common categories. Short-term memory impairments in Alzheimer-type dementia: evidence for separable impairments of articulatory rehearsal and long-term memory.
Many such individuals will indeed be found to have simple schizophrenia (so-called "pseudoneurotic" form) iglesias heart attack order 100mg lopressor amex. Here errors in diagnosis usually result from a failure to assess mental status carefully and to ascertain the life profile of the disorder heart attack telugu movie online effective lopressor 100 mg. A chronic delusional-hallucinatory state in a chronic alcoholic patient (chronic alcoholic hallucinosis) arteria femoralis communis purchase lopressor 50 mg on line. Only later do a few of these patients drift into a quiet hallucinatory ulterior motive quotes discount lopressor 12.5 mg line, mildly paranoid state, with rather bland affect. Evidence of the prepsychotic schizoid personality cannot be detected, and there is usually no family history of schizophrenia. Cases of this type with which we are familiar had their onset between 45 and 50 years of age, i. This alcoholic, schizophrenia-like illness should be differentiated from the paranoid type of schizophrenia. A patient who is confused or stuporous and seemingly catatonic-negativistic, refusing or unable to speak, to execute commands, or to be activated in any way. If signs of focal cerebral or brainstem disease are absent, one is tempted to make a diagnosis of catatonic schizophrenia, not appreciating that catatonia as a phenomenon may be indistinguishable from akinetic mutism (page 306); it may also appear with widespread disease of the associational cortices and as mentioned earlier, with severe depression, certain confusional states, and hysteria. The error can be avoided if one makes diagnoses on the basis of positive findings, not on the absence of specific data. The authors have seen cases of hypoxic and other metabolic encephalopathies, Schilder disease, certain storage diseases, and Creutzfeldt-Jakob disease mistaken for schizophrenia because of failure to adhere to this principle. A patient with temporal lobe epilepsy who, apart from intermittent psychomotor seizures, has long periods (weeks or months) of hallucinations, delusions, bizarre behavior, and disorganization of thinking. Such a mental disturbance often reflects the presence of a persistent state of temporal lobe seizures (temporal lobe status), which in some cases have been demonstrated by depth electrodes to originate in the amygdaloid or other medial temporal areas. The nature of the disturbances of emotionality and mentation in such patients, a somewhat controversial subject, is discussed in Chaps. Schizophrenic patients with prominent depressive symptoms who have made repeated suicide attempts pose an exceptionally difficult problem in diagnosis. They were referred to in the past as schizothymic, and to this day it is not certain whether they have schizophrenia, a relatively mild chronic depressive illness (dysthymia), depressive disease, or both schizophrenia and depression ("schizoaffective"). One should always be hesitant to make the diagnosis of schizophrenia during childhood, although such a diagnosis has been entertained in children who have a variety of developmental and adjustment problems and who at some time become psychotic, i. There is no evidence that such children go on to have schizophrenia later in life. And although what are thought to be "schizoid" traits may be recognized in childhood, a frank psychosis is hardly ever recorded at this age. Of particular importance in such children is to exclude the presence of metabolic errors, mental retardation, or an early-onset depressive illness. Similarly, childhood autism and particularly its milder forms (Asperger syndrome, page 889) should not be confused with schizophrenia. That the incidence of schizophrenia is not increased in the families of autistic children supports the idea that the two are separate diseases. Treatment the aims of treatment are to suppress psychotic symptoms, ameliorate the disorder of thinking and the apathetic state, prevent relapse, and optimize social adjustment. It is often possible, once the diagnosis of schizophrenia is established and the optimal regimen of medication decided upon, for a general physician to share the responsibility for following the patient with a psychiatric social worker or nurse. Relapse with psychotic decompensation demands drug therapy, and if there is a hazard of injury or suicide or difficulty in management at home, hospitalization becomes necessary. Many general hospitals and specialized psychiatric institutions have facilities for the management of such patients; state hospitals and other institutions are able to provide long-term treatment. The aim of hospitalization is to protect the patient, relieve the family of the need for constant vigilance and supervision, and assure the administration of drugs until the exacerbation spends itself. Later, instead of mere custodial care, the patient needs a supervised program of planned activities, vocational and milieu therapy, often in a "halfway house," which involves the patient as a contributing member during the more chronic phases of the disease. If medication is successful in preventing progressive decompensation, the patient can many times return to the family and community. It is invaluable to have a competent social worker or nurse maintain frequent contact with the patient and his family and assure continuity of medication.