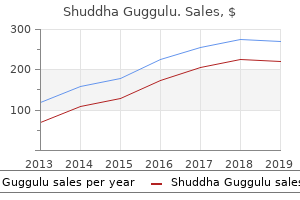
Shuddha Guggulu
"Discount shuddha guggulu 60 caps on-line, weight loss pills kill woman".
By: H. Vatras, M.B. B.CH. B.A.O., Ph.D.
Medical Instructor, Duke University School of Medicine
The major classifications of diabetes are: Approximately 5% to 10% of people with diabetes have type 1 diabetes weight loss apple cider vinegar buy cheap shuddha guggulu 60 caps on-line, in which the insulin-producing pancreatic beta cells are destroyed by an autoimmune process weight loss 2015 buy 60caps shuddha guggulu otc. As a result weight loss for kids purchase shuddha guggulu 60 caps online, they produce little or no insulin and require insulin injections to control their blood glucose levels weight loss pills do they work discount shuddha guggulu 60 caps online. If elevated glucose levels persist, diet and exercise are supplemented with oral hypoglycemic agents. In some individuals with type 2 diabetes, oral agents do not control hyperglycemia, and insulin injections are required. In addition, some individuals whose type 2 diabetes can usually be controlled with diet, exercise, and oral agents may require insulin injections during periods of acute physiologic stress (eg, illness or surgery). Type 2 diabetes occurs more among people who are older than 30 years and obese (Diabetes Information Clearing House, 2001). Diabetes complications may develop in any person with type 1 or type 2 diabetes, not only in patients who take insulin. Some patients with type 2 diabetes who are treated with oral medications may have the impression that they do not really have diabetes or that they simply have "borderline" diabetes. They may believe that, compared with diabetic patients who require insulin injections, their diabetes is not a serious problem. It is important for the nurse to emphasize to these individuals that they do have diabetes and not a borderline problem with sugar (glucose). Table 41-1 summarizes the major classifications of diabetes, current terminology, old labels, and major clinical characteristics. First, research findings suggest many differences among individuals within each category. Second, except for those with type 1 diabetes, patients may move from one category to another. For example, a woman with gestational diabetes may, after delivery, move into the type 2 category. When a person eats a meal, insulin secretion increases and moves glucose from the blood into muscle, liver, and fat cells. Often have islet cell antibodies Often have antibodies to insulin even before insulin treatment Little or no endogenous insulin Need insulin to preserve life Ketosis-prone when insulin absent Acute complication of hyperglycemia: diabetic ketoacidosis Onset any age, usually over 30 years Usually obese at diagnosis Causes include obesity, heredity, or environmental factors. No islet cell antibodies Decrease in endogenous insulin, or increased with insulin resistance Most patients can control blood glucose through weight loss if obese. Oral antidiabetic agents may improve blood glucose levels if dietary modification and exercise are unsuccessful. May need insulin on a short- or long-term basis to prevent hyperglycemia Ketosis rare, except in stress or infection Acute complication: hyperglycemic hyperosmolar nonketotic syndrome Accompanied by conditions known or suspected to cause the disease: pancreatic diseases, hormonal abnormalities, medications such as corticosteroids and estrogen-containing preparations. Depending on the ability of the pancreas to produce insulin, the patient may require treatment with oral antidiabetic agents or insulin. Onset during pregnancy, usually in the second or third trimester Due to hormones secreted by the placenta, which inhibit the action of insulin Above-normal risk for perinatal complications, especially macrosomia (abnormally large babies) Treated with diet and, if needed, insulin to strictly maintain normal blood glucose levels Occurs in about 2%5% of all pregnancies Glucose intolerance transitory but may recur: · In subsequent pregnancies · 30%40% will develop overt diabetes (usually type 2) within 10 years (especially if obese) Risk factors include obesity, age older than 30 years, family history of diabetes, previous large babies (over 9 lb). Above-normal susceptibility to atherosclerotic disease Renal and retinal complications usually not significant May be obese or nonobese; obese should reduce weight Should be screened for diabetes periodically Current normal glucose metabolism Previous history of hyperglycemia (eg, during pregnancy or illness) Periodic blood glucose screening after age 40 if there is a family history of diabetes or if symptomatic Encourage ideal body weight, because loss of 1015 lbs may improve glycemic control. The insulin and the glucagon together maintain a constant level of glucose in the blood by stimulating the release of glucose from the liver. Initially, the liver produces glucose through the breakdown of glycogen (glycogenolysis). After 8 to 12 hours without food, the liver forms glucose from the breakdown of noncarbohydrate substances, including amino acids (gluconeogenesis). It is thought that combined genetic, immunologic, and possibly environmental (eg, viral) factors contribute to beta cell destruction. Although the events that lead to beta cell destruction are not fully understood, it is generally accepted that a genetic susceptibility is a common underlying factor in the development of type 1 diabetes. People do not inherit type 1 diabetes itself; rather, they inherit a genetic predisposition, or tendency, toward developing type 1 diabetes. This is an abnormal response in which antibodies are directed against normal tissues of the body, responding to these tissues as if they are foreign.
Diseases
- Juberg Marsidi syndrome
- Short stature valvular heart disease
- Dissecting cellulitis of the scalp
- Cockayne syndrome type 2
- Halal Setton Wang syndrome
- Pseudoxanthoma elasticum, dominant form
- Cone rod dystrophy amelogenesis imperfecta
- Neural tube defect, folate-sensitive
Transport of Molecules into the Brain As an extension of the systemic circulation weight loss pills top 5 buy generic shuddha guggulu 60caps, the cerebral vasculature delivers oxygen and nutrients into the brain and removes carbon dioxide and other metabolic wastes weight loss pills for breastfeeding mothers cheap 60 caps shuddha guggulu with mastercard. Endothelial cells interact with neurons weight loss pills risks discount shuddha guggulu 60 caps with mastercard, astrocytes weight loss hypnosis app buy cheap shuddha guggulu 60caps on line, and microglia, as well as other perivascular cells, including smooth muscle cells and pericytes, to form a neurovascular unit (Lecrux and Hamel, 2011). An endothelial cell (E) surrounding the lumen, a pericyte (P) and an astrocytic endfoot process (A) are indicated. These junctions seal the paracellular space, although they remain capable of rapid modulation and regulation. Consequently, the only solutes that can passively enter the brain are lipid soluble and able to freely diffuse across endothelial cell membranes. However, in addition to clathrin-mediated transport, the plasma membranes of brain endothelia are enriched in membrane lipid rafts, called caveolae, that participate in potocytosis, a type of endocytosis by which small molecules are transported across the plasma membrane by caveolae rather than clathrin-coated vesicles. Select plasma proteins are, for example, taken up and transported across endothelial cell membranes by both receptor-mediated and receptor-independent transcytosis (transport across the interior of the cell from blood to interstitial fluid or vice versa) involving caveolae. Caveolae are also enriched in -D-galactosyl and -N-acetylglucosaminyl residues, cholesterol, sphingolipids (sphingomyelin and glycosphingolipids), as well as palmitoleic and stearic acids. The high metabolic rate within the brain is dependent on a continuous supply of glucose from the circulation, because under normal conditions, glucose is the main source of metabolic energy (see Chapter 3). These insulin-insensitive glucose transporters are constitutively expressed on the cell surface. Moreover, the pericytes, which are contractile cells that wrap around the endothelial cells, regulate the distribution of the capillary blood flow to match the local cerebral metabolic need (Dalkara et al. Aromatic amino acids in particular serve as precursors for the synthesis of the neurotransmitters serotonin, dopamine, and histamine, and the synthesis of these neurotransmitters is substrate limited. Na1-independent amino acid transport systems that have been identified in brain capillary endothelium are system L (or a high affinity isoform L1) for large neutral amino acids (including L-leucine, L-phenylalanine, L-isoleucine, 1 L-methionine, L-valine); system y for the transport of cationic amino acids (L-arginine, L-lysine, L-ornithine), 2 and system xc for anionic amino acids (cystine/glutamate exchange transporter system). The anionic amino acid transport systems are important in the inactivation of glutamatergic neurotransmission in the brain and for the synthesis of glutathione. The high affinity Na1-dependent transporters are located principally in the abluminal membrane of the cerebral endothelium (Broer and Palacin, 2011; Mann et al. The Cerebral Vasculature in Disease States Many disease states affect the cerebral vasculature. By contrast, more chronic cerebral ischemia can result in slow, progressive cognitive impairment and vascular dementia. The vasogenic edema that results is often associated with neurological impairment beyond the effects of the tumor itself. Molecular basis for endothelial lumen formation and tubulogenesis during vasculogenesis and angiogenic sprouting. The evolution of the brain, the human nature of cortical circuits, and intellectual creativity. Axonal swellings and degeneration in mice lacking the major proteolipid of myelin. Lake-front property: a unique germinal niche by the lateral ventricles of the adult brain. Varieties and distribution of non-pyramidal cells in the somatic sensory cortex of the squirrel monkey. Neuronal diversity and temporal dynamics: the unity of hippocampal circuit operations. Regulation of amino acid and glucose transporters in endothelial and smooth muscle cells. An organizing principle for cerebral function: the unit module and the distributed system. Review: molecular pathogenesis of blood-brain barrier breakdown in acute brain injury. Uber einige Beziehungen zwischen Nervenzellenerkrankungen und glio Ё Ёsen Erscheinungen bei verschiedenen Psychosen.
Shuddha guggulu 60caps low cost. patla hone ke tarike | हेल्थ टिप्स हिंदी | Sanyasi Ayurveda weight loss tips.
The tag should be securely placed on the patient and remain with the patient at all times weight loss 78209 discount shuddha guggulu 60caps visa. The log is used by the command center to track patients weight loss pills heart palpitations discount shuddha guggulu 60caps with visa, assign beds weight loss 911 buy generic shuddha guggulu 60 caps, and provide families with information weight loss before and after pictures discount 60 caps shuddha guggulu amex. Managing Internal Problems Each facility must determine its supply lists based on its own needs assessment. For example, the hospital might plan to have available a stockpile of cyanide kits or antibiotics used in treating biological agents. Information should be available about local resources for stocking or restocking any of the basic and special supplies, how those supplies are requested, and the time required to receive those supplies. Triage of Disaster Victims Triage is the sorting of casualties to determine priority of health care needs and the proper site for treatment. In nondisaster situations, health care workers assign a high priority and allocate the most resources to those who are the most critically ill. For example, a young man who has a chest injury and is in full cardiac arrest would receive advanced cardiopulmonary resuscitation, including medications, chest tubes, intravenous fluids, blood, possibly even emergency surgery in an effort to restore life. In a disaster, however, when health care providers are faced with a large number of casualties, the fundamental principle guiding resource allocation is to do the greatest good for the greatest number of people. Decisions are based on the likelihood of survival and consumption of available resources. Therefore, this same patient, and others with conditions associated with a high mortality rate, would be assigned a low triage priority in a disaster situation, even if the person is conscious. Although this may sound uncaring, from an ethical standpoint the expenditure of limited resources Communicating With the Media and Family Communication is a key component of disaster management. Communication within the vast team of disaster responders is paramount; however, effective, informative communication with the media and worried family members is also crucial. A clearly defined process for managing the media, which includes a designated spokesperson, a site for the dissemination of information (away from patient care areas), and a regular schedule for providing updates should be part of the disaster plan. Such a plan helps to prevent the release of contradictory or inaccurate information. Individuals in this group can progress rapidly to expectant if treatment is delayed. Delayed: Injuries are significant and require medical care, but can wait hours without threat to life or limb. Individuals in this group receive treatment only after immediate casualties are treated. Expectant: Injuries are extensive and chances of survival are unlikely even with definitive care. Persons in this group should be separated from other casualties, but not abandoned. Comfort measures should be provided when possible 1 Red 2 Yellow 3 Green Sucking chest wound, airway obstruction secondary to mechanical cause, shock, hemothorax, tension pneumothorax, asphyxia, unstable chest and abdominal wounds, incomplete amputations, open fractures of long bones, and 2nd/3rd degree burns of 1540% total body surface area. Upper extremity fractures, minor burns, sprains, small lacerations without significant bleeding, behavioral disorders or psychological disturbances. They may be feeling intense anxiety, shock, or grief and should be provided with information and updates about their loved ones as soon as possible and regularly thereafter. They should not be in the triage or treatment areas, but in a designated area staffed by available social service workers, counselors, therapists, or clergy. Access to this area should be controlled to prevent families from being disturbed. See Chart 72-2 for a discussion of cultural variables to consider when coping with disaster-related injuries and death. The Role of Nursing in Disaster Response Plans the role of the nurse during a disaster varies. The nurse may be asked to perform outside his or her area of expertise and may take on responsibilities normally held by physicians or advanced practice nurses.
Trifolium Pratense (Red Clover). Shuddha Guggulu.
- How does Red Clover work?
- High cholesterol in women
- Menopausal symptoms, hot flashes.
- Dosing considerations for Red Clover.
- Are there safety concerns?
- Are there any interactions with medications?
- Prevention of osteoporosis in women, prostate gland symptoms (such as increased nighttime urination) in men, cancer prevention, indigestion, lung problems (cough, bronchitis, asthma), cyclical breast pain, sexually transmitted diseases (STDs), premenstrual syndrome (PMS), skin problems (cancerous growths, burns, eczema, psoriasis), and other conditions.
- What is Red Clover?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96329