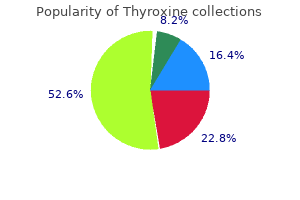
Thyroxine
"Buy thyroxine 150mcg, medications mothers milk thomas hale".
By: R. Moff, M.B. B.A.O., M.B.B.Ch., Ph.D.
Professor, University of Miami Leonard M. Miller School of Medicine
The accumulation compresses the heart and thereby impedes expansion of the ventricles and cardiac filling during diastole symptoms job disease skin infections cheap thyroxine 50 mcg line. As ventricular volume and cardiac output fall administering medications 7th edition answers buy thyroxine 125mcg line, the heart pump fails treatment dynamics order 50 mcg thyroxine with amex, and circulatory collapse develops symptoms graves disease buy 150mcg thyroxine amex. With gradual onset, fluid accumulates gradually, and the outer layer of the pericardial space stretches to compensate for rising pressure. With rapid onset, pressures rise too quickly for the pericardial space to compensate. Cancerous tumors, particularly from adjacent thoracic tumors (lung, esophagus, breast cancers), and cancer treatment are the most common causes of cardiac tamponade. Radiation therapy of 4,000 cGy or more to the mediastinal area has also been implicated in pericardial fibrosis, pericarditis, and resultant cardiac tamponade. Untreated pericardial effusion and cardiac tamponade lead to circulatory collapse and cardiac arrest. In malignant effusions, pericardiocentesis provides only temporary relief; fluid usually reaccumulates. Windows or openings in the pericardium can be created surgically as a palliative measure to drain fluid into the pleural space. Catheters may also be placed in the pericardial space and sclerosing agents (such as tetracycline, talc, bleomycin, 5-fluorouracil, or thiotepa) injected to prevent fluid from reaccumulating. Medical · Chemotherapy, biologic response modifier therapy, radiation therapy, or surgery is used to treat the underlying cancer. Clots are deposited in the microvasculature, placing the patient at great risk for impaired circulation, tissue hypoxia, and necrosis. In addition, fibrinolysis occurs, breaking down clots and increasing the circulating levels of anticoagulant substances, thereby placing the patient at risk for hemorrhage. The release of intracellular contents from the tumor cells, leads to electrolyte imbalances-hyperkalemia, Clinical Clinical manifestations depend on the extent of metabolic abnormalities. Medical Fluid intake range limited to 500 to 1,000 mL/day to increase the serum sodium level and decrease fluid overload. When neurologic symptoms are severe, parenteral sodium replacement and diuretic therapy are indicated. Electrolyte levels are monitored carefully to detect secondary magnesium, potassium, and calcium imbalances. If water excess continues despite treatment, pharmacologic intervention (urea and furosemide) may be indicated. Medical · To prevent renal failure and restore electrolyte balance, aggressive fluid hydration is initiated 48 hours before and after the initiation of cytotoxic therapy to increase urine volume and eliminate uric acid and electrolytes. Critical Thinking Exercises You are seeing a married couple in their 70s in the clinic for blood pressure checks. How would you respond if your suggestions for cancer screening are met with the answer that they are too old to worry about cancer? What special considerations are there if the woman has a physical disability that requires her to use a wheelchair? A 54-year-old woman with bone metastases secondary to breast cancer has been admitted to the hospital with a diagnosis of hypercalcemia. Describe the underlying cause of hypercalcemia and the medical and nursing management strategies that are anticipated. What patient monitoring would be essential before and after treatment of hypercalcemia? One of your home care patients, a 42-year-old executive of a major corporation, has a nonresectable malignant brain tumor for which she is receiving radiation therapy. She is being discharged from the hospital and will continue therapy as an outpatient. She is also concerned about her ability to carry out her executive responsibilities. What assessment by the nurse is indicated at this point, and what actions would be warranted by the nurse to help the patient and her husband deal with their concerns?
Simple tests using microscopy can detect certain vaginal infections medications like zovirax and valtrex buy 200mcg thyroxine free shipping, but laboratory tests to detect cervical infections caused by gonorrhoea and chlamydia are more expensive and complicated treatment for sciatica buy cheap thyroxine 100mcg on line. Moreover treatment vs cure 75mcg thyroxine mastercard, results are generally not available while the patient is still at the clinic treatment lymphoma order thyroxine 50mcg overnight delivery, which often means a missed opportunity for treatment if infection is found. And in resource-poor settings, laboratory methods of diagnosis are often neither affordable nor available. This approach uses standard flowcharts, adapted to the local epidemiological profile, to decide on a treatment that will be effective against all the organisms most commonly known to cause the particular syndrome in the particular setting. The method is simple and does not require extensive training for health personnel. An important advantage is that this approach helps to ensure that the patients get effectively treated at their first and probably only contact with the health system. However, this also means treating for several possible infections even if the patient has only one. Abnormal vaginal discharge is highly indicative of vaginal infections, but is a poor predictor of cervical infections, which are often asymptomatic. Strategies have been developed to improve syndromic management of vaginal discharge and to detect more cases of cervical infection (the cervix is the most common site of infection for gonorrhoea and chlamydia). Syndromic management may be improved in populations with high prevalence of gonorrhoea and chlamydia by introducing speculum examinations to detect cervical mucopus (although where this is not possible, it is better to treat presumptively when cervical infection is suspected). Given the low rate of return by clients for follow-up, diagnosis and treatment in one visit is generally preferable. Specific guidelines for diagnosis and treatment should be adapted to local conditions. However, several programme examples show that with sufficient resources it is possible to surmount social barriers within clinics. All reproductive health programmes should undertake prevention and counselling (with a special emphasis on the dual protection that male and female condoms provide), and symptomatic clients should be treated as appropriate. In areas where overall prevalence rates are low, targeting services to especially vulnerable groups such as sex workers, long-distance truck drivers, prisoners, street children, refugees and the internally displaced can be a cost-effective way to break the cycle of transmission and reduce rates of infection. Encourage screening and treatment for maternal syphilis as part of routine antenatal care. Millions of women access these clinics each year (surveys in several East African countries show that more than 90 per cent of women use these services). Family planning and antenatal care facilities serve primarily though not exclusively married women and those in stable relationships. Moreover, prevention messages need to be directed to men and to other higher risk groups. Thus, it may be useful to offer services for men where they work (occupational services) or through referrals. Another argument against integration is based on the need to reach higher risk populations. Various examples show that it is possible for an integrated programme to also reach out to vulnerable or at-risk groups. Early treatment can reduce the duration of infection, prevent the development of complications, protect their current or future sexual partners, and break the chain of transmission (secondary prevention). From a public health perspective, prevention measures aimed at high-frequency transmitters (those who have many partners or engage in high-risk sexual behaviours) can be more effective than measures targeting the general population. It is often especially hard for married women to refuse sex with their husbands or to insist on use of a condom, and efforts to empower them in partner negotiation may be helpful. The points below should be considered in designing or implementing programmes or advocating for policy. High-risk populations may include sex workers, long-distance truck drivers, prisoners, army personnel, street children, adolescents in penal institutions, refugees and the internally displaced. Such counselling should be a routine part of any reproductive health consultation. If so, the client should be referred to a higher level of service for screening, diagnosis and treatment.
These classifications complement the three delays model because they go beyond emergency obstetric care medications side effects discount 75mcg thyroxine with amex. All of these building blocks are determinants of the coverage and quality of care that women receive across the continuum of care symptoms 11dpo buy 25 mcg thyroxine. Country case studies describe the relative importance of these building blocks or equivalent groupings in understanding progress in maternal health (McPake and Koblinsky 2009) treatment without admission is known as cheap thyroxine 150mcg with mastercard. Progress has also been made for skilled birth attendance since 1990 (median coverage of 57 percent) medicine quotes doctor thyroxine 125mcg discount, emergency obstetric care (as measured, for example, by the cesarean section rate, and by the density of emergency obstetric care facilities per birth or population), and postnatal care for mothers (median coverage of 41 percent). For example, the welldocumented decline in maternal mortality in Bangladesh may be related to the availability of emergency obstetric care interventions and fertility decline, but it is also likely to be linked to the increased participation of women in the labor force. Several ecological studies of maternal mortality have shown the relationship between maternal mortality and skilled birth attendance, as well as to gross national product, health care expenditures, female literacy, population density, and access to clean water (Buor and Bream 2004; Montoya, Calvert, and Filippi 2014). Observational studies have shown inadequate levels of hygiene in many maternity facilities (Benova, Cumming, and Campbell 2014), with direct health impacts on mothers, newborns, and care providers (Mehta and others 2011). The reasons are multifactorial and include poor infrastructure; inadequate equipment and supplies; and poor practices by care providers and cleaners as a result of inadequate knowledge, attitudes, motivation, and supervision (Campbell and others 2015). Interventions to address these constraints go beyond the health sector, particularly for water and sanitation (Shordt, Smet, and Herschderfer 2012). Timely access to care and the difficulties in obtaining motorized transport, as well as challenging topography and inadequate and poorly maintained roads, are important barriers to care. Gabrysch and others (2011) demonstrate that in Zambia, the odds of women being able or choosing to deliver in a health facility decreased by 29 percent with every doubling of distance between their home and the closest facility. They conclude that if all Zambian women lived within 5 kilometers of health facilities, 16 percent of home deliveries could be averted. The proportion of hemorrhage and hypertension deaths found globally remains high despite established interventions to prevent and treat direct causes of maternal death (see chapter 7), such as active management of the third stage of labor. With the data available, it is not possible to determine if this high proportion is the result of a failure to implement policies and therefore quality of care, if there is a shift toward antepartum hemorrhage, or if misclassifications of abortion and obstructed labor are erroneously increasing the hemorrhage category. A Lifecycle Perspective Safe motherhood programs traditionally consider each pregnancy to be a separate event. Emerging evidence from cohort studies of near-miss patients suggests that women who have suffered severe obstetric complications have increased mortality risks for several years and have a higher risk of complications in subsequent pregnancies. It is important to be able to identify these women and offer them medical support for an extended postpartum period and in subsequent pregnancies (Assarag and others 2015; Storeng and others 2012). Role of Indirect Causes the data presented in this chapter also suggest that the proportion of maternal deaths due to indirect causes is increasing in most parts of the world. In addition, although the proportion of women who have a serious morbidity remains a hotly debated topic by epidemiologists, we estimate that approximately 30 percent of women may have a serious condition during pregnancy, childbirth, or the postpartum period. The main strategies used to date to reduce maternal mortality are based on the understanding that most complications are emergencies and that most deaths occur during a very short period around childbirth. Accordingly, the focus has been on reducing delays for emergency care, as well as on preventive measures, such as facilitating access to skilled birth attendance and reproductive rights. Complementary strategies are needed to address the indirect causes of death and the broader burden of maternal morbidity, in particular, given that the sequelae of maternal morbidity can last a long time. Health program managers and policy makers need to continue to encourage women to deliver in health facilities, where complications can be prevented by appropriate care and where women can receive lifesaving interventions. At the same time, the gaps in coverage of effective interventions for indirect causes of death according to their distribution in various settings have significant implications for the complexity of service delivery in light of the urgent need to accelerate the rate of decline in maternal mortality and, ultimately, Levels and Causes of Maternal Mortality and Morbidity 65 to stop all preventable deaths. Primary health care may have a greater role in the future in improving the health outcomes of pregnant and recently delivered women. Quality of Health Care Services In addition, if the post-2015 agenda is to emphasize universal access to essential interventions, the perceived and technical quality of the health care services provided becomes even more crucial in the fight against maternal mortality and morbidity, given their consequences for both demand for and supply of services. Thus, the international community emphasizes the development and implementation of a palette of quality-of-care interventions, including clinical audits, childbirth checklists, maternal deaths surveillance and response, and interventions to increase awareness around respectful care. Although the global attention to maternal mortality has engendered more studies and attempts to measure it, the quality, regularity, and ability of the results to robustly show differentials have not improved dramatically, especially routine sources of information such as vital registration. At the community level, data on direct obstetric complications are almost nonexistent; the burden of ill health associated with some conditions, such as sepsis and ectopic pregnancies, has not been reviewed for many years. Better population-based sources for local-level decision making are essential to achieving improved outcomes.
Syndromes
- Anticholinergics
- Rare causes, such as untreated syphilis or marfan syndrome
- Symptoms of the underlying problem (such as loss of sensation due to a nerve injury in vitamin B12 deficiency)
- Cannot empty the bladder
- Fibrocystic breast disease
- Alcohol or drug withdrawal state
Behavioral Interventions Many actions or decisions by caregivers medications vertigo 200mcg thyroxine fast delivery, health care providers medicine 666 colds 200mcg thyroxine with mastercard, and public health officials require behavior changes and the decision to act symptoms gluten intolerance thyroxine 50mcg discount. If improved practices became the norm treatment laryngitis buy 200 mcg thyroxine with mastercard, risk of diarrhea and morbidity and mortality rates would diminish. Each of these behaviors may be difficult to sustain, but each would have a major impact. Handwashing the transfer of infectious agents via the hands directly between individuals or indirectly through contamination of inanimate objects (fomites), such as dishes, utensils, and other objects (Abad and others 2001), is a common route for the transmission of low inoculum diarrhea pathogens (as well as respiratory infections). Contaminated hands readily inoculate food or water, allowing high inoculum pathogens to multiply. Simple handwashing procedures 174 Reproductive, Maternal, Newborn, and Child Health significantly reduce transmission rates in health care facilities (Bolon 2011); households (Bloomfield 2003); schools (Lee and Greig 2010); and even day care and preschool settings, which are notoriously difficult environments in which to enforce good hygiene (Churchill and Pickering 1997). Handwashing has an additional benefit in also reducing transmission of respiratory infections (Luby and others 2005). Provision of soap to an urban squatter community in Karachi, Pakistan, supported by weekly meetings with trained health care workers from the same communities to reinforce the behavior, reduced days with diarrhea by 39 percent (95 percent confidence interval -61 percent to -16 percent) among infants compared with controls over one year (Luby and others 2004). An additional benefit was a 50 percent reduction in the incidence of pneumonia (95 percent confidence interval -65 percent to -34 percent). In Bangladesh, the risk of diarrhea diminished when caregivers washed both hands with water before preparing food (odds ratio 0. Risk was also reduced when caregivers washed hands with soap after defecation, but not with water alone (odds ratio 0. Direct observations identified more than 20 opportunities per day for handwashing, a frequency considered impossible to achieve, especially when the added cost of soap is considered. Handwashing after contact with feces is poorly practiced globally (Freeman and others 2014), and Luby and others (2011) recommended prioritizing handwashing before food preparation because it was the single most effective opportunity to reduce diarrhea risk. A randomized intervention in Pakistan compared provision of soap for handwashing with a method to disinfect water or no intervention, including weekly visits over nine months to encourage either practice (Luby and others 2006). The study documented a 55 percent reduction in diarrhea (95 percent confidence interval 17 percent to 80 percent) compared with control neighborhoods, but no difference between the soap or water disinfection groups. When reenrolled in a follow-up surveillance 18 months later, handwashing intervention households were still 1. During weekly follow-up throughout the 14 months without active educational intervention there was no difference between the groups in the proportion of person-days with diarrhea (1. Three years later, however, the investigators reengaged 461 original households (69 percent) and found the original intervention households were 3. The critical question is not whether improving handwashing practices is effective, but rather how to best promote consistent behavior. The behavior requires availability of water and household handwashing stations designed and located to facilitate rather than inhibit the practice (Hulland and others 2013). Educational support from health care workers is useful, but how much is feasible and affordable remains in question. Health Care Seeking To ensure optimal care of infants and children with diarrheal disease, caregivers must recognize there is a problem, know what to do and do it, be alert to signs of clinical deterioration needing professional care, and know how to access such care without delay. Knowledge and experience are necessary but not sufficient; caregivers must also have the authority to act promptly. Initiatives to scale up prompt decision making and action generally focus on technical details and acquisition of practical skills, but frequently overlook social and cultural dimensions. These factors may influence whether a caregiver recognizes that fluid losses are beyond normal limits, are becoming dangerous, and require professional intervention (Larrea-Killinger and Muсoz 2013). Higher levels of education promote quicker careseeking action; however, cultural influences, for example, gender discrimination, can delay action for female infants (Malhotra and Upadhyay 2013). In rural Burkina Faso Diarrheal Diseases 175 caregivers failed to recognize mild diarrhea, especially among infants, and made intervention choices that were not clinically based and recommended (Wilson and others 2012). Cost of treatment is the major pragmatic impediment to care seeking outside of the home (Nasrin and others 2013).
Generic thyroxine 25 mcg visa. Measles: Causes and Symptoms.