Capoten
"Discount 25mg capoten visa, medicine quest".
By: I. Curtis, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Assistant Professor, Indiana Wesleyan University
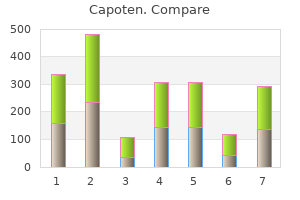
There are only a few possibilities: 1) the patient would have to take a drug which excretes chloride or retains bicarbonate symptoms lupus buy capoten 25mg free shipping. Looking at the three blood gas measurements: 1) the venous bicarb and the arterial bicarb are roughly the same treatment brown recluse bite buy 25 mg capoten free shipping. All that can be said about a venous pO2 is that it is lower than the arterial pO2 medicine 6mp medication purchase capoten 25mg with amex. All that can be said about a capillary pO2 is that it lies somewhere between the venous pO2 and the arterial pO2 treatment deep vein thrombosis 25mg capoten with amex. Therefore, a venous blood gas or capillary blood gas done in conjunction with a pulse oximeter measurement, should accurately reflect the arterial blood gas as long as the capillary source is well perfused. The arterial pO2 is frequently described as the paO2 to denote that this is an arterial sample, as opposed to a venous or capillary pO2. Blood gases and pulse oximeters can be occasionally fooled so it is important to know when these tests provide us with misleading information. This concept is difficult to visualize, but it can best be thought of as the force that the oxygen particles exert on the side of an enclosed container. Gases travel rapidly, so that the partial pressures of gases tend to be identical in samples that are next to each other for at least 5 seconds. Gas pressure or gas tension is measured in mmHg or Torr, which are exactly the same thing. The atmospheric pressure at sea level is 760 mmHg (or Torr) and the atmosphere contains 21% oxygen. As the coffee sits on the table, its gas content rapidly equilibrates with the environment so the pO2 in the liquid coffee is 160 mmHg. If one sends a sample of coffee to the blood gas lab, the blood gas machine should measure a pO2 of 160. If I replaced my blood with coffee, my brain and other tissues would not be happy since although the pO2 of the coffee may be 160, it does not contain much oxygen. One ml of coffee contains only a few oxygen molecules, while one ml of blood contains many, many more oxygen molecules. While many fluids may have reasonably good pO2s, only blood has a satisfactory oxygen content. The pO2 of a fluid sample is a measurement of its oxygen gas tension (or pressure), but it is not a measurement of oxygen content. This curve plots the oxygen saturation (in %) on the vertical axis and pO2 on the horizontal axis. The oxygen saturation % steadily increases as the pO2 increases up to about a pO2 of 100 mmHg at which point the oxygen saturation is 99% to 100%. If the patient breathes supplemental oxygen, the inspired pO2 increases to 200 mmHg, 400 mmHg or higher depending on how much oxygen is inhaled. So the typical appearance of an oxygen hemoglobin dissociation curve, has a steep rise at pO2s below 100 mmHg, at which point it becomes a plateau since the oxygen saturation cannot increase above 100%. Oxygen saturation (SaO2) is a measurement of the percentage of oxygen binding sites that contain oxygen. If all the oxygen binding sites contain oxygen, then the oxygen saturation is 100%. An oxygen saturation measurement can only be done on blood, as opposed to a pO2 which can be done on coffee or any fluid. The pO2 and the SaO2 are related to each other by the oxygen hemoglobin dissociation curve, which students learn in physiology. This curve plots the oxygen saturation (in %) on the vertical axis and pO2 on the Page - 294 horizontal access. The oxygen saturation % steadily increases as the pO2 increases up to about a pO2 nearing 90 to 100 mmHg at which point the oxygen saturation is 99% to 100%. Oxygen saturation can be measured continuously and non-invasively by pulse oximetry. Pulse oximetry uses light absorption through a pulsing capillary bed usually in a toe or finger, but it will also pick up in the nose, ear, palm, side of the foot, etc. The probe looks red, but it actually uses two light sources; one is red and the other is invisible infrared. Absorption using these two wave lengths measures oxygen saturation for hemoglobin A. Pulse oximetry will not measure the oxygen saturation correctly for other hemoglobins such as methemoglobin or carboxyhemoglobin.
Tympanic temperature measured with a probe against the tympanic membrane as commonly employed by anesthesiologists is very accurate compared with other core temperature measurements medicine interactions buy capoten 25mg without a prescription. Recently infrared ear thermometers have become popular because they give very rapid readings medicine ketoconazole cream discount 25mg capoten free shipping. However these commonly available infrared ear thermometers used in clinics treatment alternatives discount capoten 25mg mastercard, hospital wards treatment hepatitis c cheap 25 mg capoten, and homes are somewhat inaccurate and show significant variation between measurements. I have also encountered falsely elevated readings in multiple patients especially when the instrument is older or malfunctioning. Therefore, an unexpected elevated reading from an infrared ear thermometer should be confirmed with an oral or rectal measurement before embarking on an investigation of fever. Once it is proven that the patient has a fever, infrared ear readings may be used to measure trends in temperature associated with therapy of the basic process as long as one remembers that ear readings are variable and less accurate. Axillary temperature accuracy can be improved by keeping the thermometer in place for 5 to 12 minutes and holding the arm flexed against the body for the entire period. Therefore if tactile fever is reported, later confirmation of either elevated temperature or an abnormal clinical appearance is needed before embarking on an etiologic investigation (4). The first comprehensive study of temperature variation was published in 1868 by Carl Wunderlich (5,6). It is still the most comprehensive study and involved nearly one million observations in 25,000 subjects. He demonstrated that normal individuals have a range of temperature readings and that there is a diurnal variation with the lowest daily reading falling between 2 and 8 a. More recent studies using more modern instruments found normal oral temperature to vary between 35. Temperature was lowest at 0600 hours and peaked in late afternoon between 1600-1800. The mean difference between lowest and highest daily temperatures in these adult subjects was 0. For each individual, there existed a characteristic narrow range or normal set-point of body temperature showing diurnal variation of 0. Body temperature is affected very little by environmental conditions but to a greater degree by vigorous exercise. For a population of normal adults, the range of oral body temperature measurements is wider than the individual variation of 0. A systematic review of articles published from 1939-1990 showed the range for normal oral temperatures to be somewhat wider 33. Page - 170 There has been less systematic study of normal temperatures in children. It has been suggested that preschool children have a more exaggerated diurnal difference in than adults with higher temperatures late in the afternoon or after physical activity (8). A study of rectal temperatures taken once throughout the day in 671 well infants < 3 months old demonstrated (9): Age in days Birth - 30 days 31-60 days 61-91 days Mean temperature C 37. A third study found no evidence for temperature elevation with tooth eruption or the 5 days preceding (12). The idea that teething causes fever is a widespread folk belief shared by a majority of parents and pediatric dentists but by less than 10% of pediatricians (13). It remains somewhat uncertain exactly where the febrile range begins but oral temperatures greater than 37. Many lay people and health care professionals regard oral temperature readings between 37 and 38 degrees C (98. Certain individuals may have temperature elevations greater than this while being entirely well especially in late afternoon or after vigorous exercise. The presence of sustained fever of any degree indicates a problem which may need evaluation. Recognizing the presence of fever is of significance, but concern about the height of the fever is of less importance since the height of fever by itself is of limited diagnostic value. Physiology of Fever: Fever producing substances are divided into two categories: those produced outside the body (exogenous pyrogens) and those produced inside the body (endogenous pyrogens). Exogenous pyrogens are usually microorganisms, their components or their extracellular products. Endogenous pyrogens are host cell derived cytokines which are the principal central mediators of the febrile response. The secretion of endogenous pyrogens is induced by both exogenous pyrogens and many endogenous molecules such as antigen-antibody complexes, complement, steroid metabolites, certain bile acids, and many lymphocyte derived molecules.
Order capoten 25 mg with visa. Ketogenic Diet: Does it Work? | UCLA Center for Human Nutrition.
Studies have shown that as many as 25 percent of users who inject steroids have shared needles (5) treatment zone lasik buy cheap capoten 25mg online. Anabolic steroid users are also more likely to use other drugs and experience their attendant risks jnc 8 medications buy capoten 25 mg on line. However symptoms 38 weeks pregnant buy capoten 25mg visa, premature epiphyseal closure is irreversible and peliosis (purpura) medicine escitalopram purchase capoten 25 mg overnight delivery, hepatoma, baldness, clitoromegaly and voice changes will likely persist. Because anabolic steroid use can have multisystemic effects as described above, the differential diagnosis would at first appear to be a lengthy one. However, a history of athletic involvement in sports where muscle mass is important coupled with an unusual degree of muscle development should place anabolic steroid use at the top of the differential diagnosis list. Testosterone-producing tumors may have masculinizing effects on both males and females, but usually result in muscle-wasting and other signs of chronic illness. Once an adolescent who is using anabolic steroids has been identified, the pediatrician assumes the role of educator and counselor. Traditional drug treatment programs do not treat youths using anabolic steroids unless this use is part of a broader spectrum of substance use. Guidelines for the approach to the adolescent using anabolic steroids have been established by the American Academy of Pediatrics (2). In general, counseling should be provided in a confidential and non-judgmental manner. It is appropriate to acknowledge to the patient that anabolic steroids may, in fact, lead to increased muscle mass and strength. It is also appropriate to express an understanding of why athletes and others might want to increase muscle mass, strength and definition. This honest discussion of the "benefits" of steroid use must then be balanced with an honest review of the risks of use. There is no evidence that scare tactics work in diminishing steroid use since the drive to excel athletically is so strong. At the individual patient level, screening questions and anticipatory guidance regarding anabolic steroid use should be a part of each well-teen visit. Adolescents who present with signs or symptoms suggestive of steroid use, even if not related to the presenting complaint, should be asked specifically about the possibility of anabolic steroid use at acute care visits. Adolescents can be counseled about alternatives for improving their strength and appearance through healthier diets and appropriate physical training. At a community level, pediatricians can educate parents, schools and coaches about the prevalence and risks of anabolic steroid use among students. Musculoskeletal: premature epiphyseal closure, short stature, ligament and tendon injuries. Male reproductive: decreased testosterone production, decreased testicular size, impotence, enlarged prostate. Female reproductive: breast atrophy, clitoromegaly, menstrual changes, teratogenicity. Psychological: severe anger outbursts, hallucinations, paranoia, anxiety, addiction. True/False: Anabolic steroid use is usually effective in enhancing athletic performance. In which patients should pediatricians consider the possibility of anabolic steroid use One of the reasons it is difficult to dissuade competitive athletes from using anabolic steroids is that it can, in fact, result in increased lean body mass, muscle strength, and aggressiveness. An adolescent in early puberty who uses steroids risks premature epiphyseal closure with resultant shorter stature than otherwise would be predicted. Anabolic steroid use should be considered and addressed with all adolescent patients, male or female, athlete or non-athlete. Particular attention should be paid to those adolescents who have greater than expected muscle-mass development or in females with signs of masculinization.
Giving 262 ml means giving 1 unit (about 250 ml) medicine park lodging cheap capoten 25 mg free shipping, and about 10 ml from a second unit (discarding the rest) medications every 8 hours buy capoten 25 mg on line. For just a few hives treatment jokes capoten 25mg discount, it is not necessary to check the crossmatch of the blood treatment hyperthyroidism order 25 mg capoten visa, since this will detect antibodies causing hemolysis. Usually diphenhydramine alone can resolve the hives, and the same unit can be continued with the diphenhydramine in effect. Additionally, a child with such an extremely low hemoglobin needs to be transfused very slowly, at least initially, so as not to push his already compromised heart into further failure. With severe anemia, the patient is already in high output congestive heart failure. Thus, the transfusion must proceed very slowly under close hemodynamic monitoring. She was hospitalized three weeks ago for a pseudomonas external otitis media and neutropenia that was treated with two weeks of intravenous antibiotics. There is no family history of recurrent bacterial infection, neutropenia, immunodeficiency disease, autoimmune disease, or malignancy. Antineutrophil antibody testing is sent off to a specialized reference laboratory and it returns positive. A bone marrow examination is done (mostly because of parental concern) which shows a normal cellular marrow. Case 2 this is a 2 year old male who presents with a chief complaint of recurrent skin and soft tissue infections. Screening tests of humoral, cell mediated, and complement mediated immunity were normal. Referral is now being made to a hematologist during his current hospitalization for the treatment of cervical lymphadenitis and left lower lobe pneumonia with bilateral pleural effusions. Past Medical History: At 2 months of age, he developed a perianal furuncle that was incised and drained because of no response to oral antibiotics. At 5 months of age, he had surgical treatment for multiple perianal fistulas with abscesses. At 7 months of age, he had a left inguinal Klebsiella pneumoniae lymphadenitis that was treated with incision and drainage and oral amoxicillin/clavulanic acid. Two weeks later, a left subauricular lymph node abscess was incised and drained and a persistent perianal fistula received topical treatment with silver nitrate. Pseudomonas aeruginosa grew out of cultures of the neck abscess and the patient was hospitalized for intravenous antibiotic treatment and immunological evaluation. In addition to his subauricular lymphadenitis, he had a left calf cellulitis that grew Serratia marcescens and a left inguinal abscess that grew Staphylococcus epidermidis. However subsequently, he develops a slight limp at which time a large lytic bone lesion is found in the distal left tibia on plain x-rays. Culture of that lesion grows out Staphylococcus aureus after debridement and curettage. He is placed on subcutaneous injections of gamma interferon (three times a week) and twice daily doses of oral trimethoprim-sulfamethoxazole and has not required any further hospitalizations for bacterial infections for the last 3 years. Neutrophils (polymorphonuclear leukocytes) represent the first line of active defense against bacterial and fungal invasion for the innate immune system. Despite the relative rarity of primary neutrophil defects, clinical situations in which neutrophil function is decreased, such as prematurity, are commonly associated with increased rates of invasive bacterial infection. Primary deficiencies of neutrophil numbers or function are usually associated with an increased risk of serious, often life-threatening infections. Secondary deficiencies of neutrophil numbers or function are usually markers of systemic disease and tend to be clinically benign. The most common problem seen by primary care physicians is neutropenia (decreased neutrophil count). Acute inflammatory processes are commonly associated with normal or reactive increases in neutrophil counts. When low neutrophil counts are associated with infection it must be decided whether neutropenia is secondary to the infection, or if an underlying neutropenia contributed to the risk of infection. A key point to remember is that the risk of infection with neutropenia is high when bone marrow production of neutrophils is decreased from either primary or secondary causes. In general, common disorders are usually benign clinically and occur in children with no significant medical history of bacterial or fungal infections.