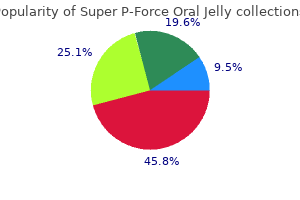
Super P-Force Oral Jelly
"Safe super p-force oral jelly 160 mg, erectile dysfunction 29".
By: I. Sigmor, M.B.A., M.D.
Clinical Director, Wake Forest School of Medicine
If you do not understand why using an acronym might be helpful blood pressure drugs erectile dysfunction super p-force oral jelly 160 mg with visa, or how to create an acronym erectile dysfunction statistics in canada 160mg super p-force oral jelly sale, the strategy is not likely to help you erectile dysfunction doctors in pittsburgh cheap super p-force oral jelly 160mg with visa. In a production deficiency the child does not spontaneously use a memory strategy and must be prompted to do so impotence marriage buy discount super p-force oral jelly 160 mg line. In this case, children know the strategy and are more than capable of using it, but they fail to "produce" the strategy on their own. For example, children might know how to make a list, but may fail to do this to help them remember what to bring on a family vacation. A utilization deficiency refers to children using an appropriate strategy, but it fails to aid their performance. Utilization deficiency is common in the early stages of learning a new memory strategy (Schneider & Pressley, 1997; Miller, 2000). Until the use of the strategy becomes automatic it may slow down the learning process, as space is taken up in memory by the strategy itself. Initially, children may get frustrated because their memory performance may seem worse when they try to use the new strategy. Once children become more adept at using the strategy, their memory performance will improve. In contrast, strategies acquired after this age often followed an "all-or-nothing" principle in which improvement was not gradual, but abrupt. Knowledge Base: During middle and late childhood, children are able to learn and remember due to an improvement in the ways they attend to and store information. As children enter school and learn more about the world, they develop more categories for concepts and learn more efficient strategies for storing and retrieving information. One significant reason is that they continue to have more experiences on which to tie new information. In other words, their knowledge base, knowledge in particular areas that makes learning new information easier, expands (Berger, 2014). Metacognition: Children in middle and late childhood also have a better understanding of how well they are performing a task, and the level of difficulty of a task. As they become more realistic about their abilities, they can adapt studying strategies to meet those needs. Young children spend as much time on an unimportant aspect of a problem as they do on the main point, while older children start to learn to prioritize and gauge what is significant and what is not. Metacognition refers to the knowledge we have about our own thinking and our ability to use this awareness to regulate our own cognitive processes (Bruning, Schraw, Norby, & Ronning, 2004). Schneider and colleagues found that there were considerable individual differences at each age in the use of strategies, and that children who utilized more strategies had better memory performance than their same aged peers. Critical thinking, or a detailed examination of beliefs, courses of action, and evidence, involves teaching children how to think. The purpose of critical thinking is to evaluate information in ways that help us make informed decisions. Critical thinking involves better understanding a problem through gathering, evaluating, and selecting information, and also by considering many possible solutions. These include: Analyzing arguments, clarifying information, judging the credibility of a source, making value judgements, and deciding on an action. Metacognition is essential to critical thinking because it allows us to reflect on the information as we make decisions. Language Development Vocabulary: One of the reasons that children can classify objects in so many ways is that they have acquired a vocabulary to do so. This language explosion, however, differs from that of younger children because it is facilitated by being able to associate new words with those already known, and because it is accompanied by a more sophisticated understanding of the meanings of a word. New Understanding: Those in middle and late childhood are also able to think of objects in less literal ways. For example, if asked for the first word that comes to mind when one hears the word "pizza", the younger child is likely to say "eat" or some word that describes what is done with a pizza. However, the older child is more likely to place pizza in the appropriate category and say "food". This sophistication of vocabulary is also evidenced by the fact that older children tell jokes and delight in doing do. They may use jokes that involve plays on words such as "knockknock" jokes or jokes with punch lines.
Children with bronchiectasis should be treated with antibiotics during symptom exacerbations based upon sputum culture results erectile dysfunction 40 year old man buy cheap super p-force oral jelly 160mg. There may also be a role for inhaled corticosteroids to modulate the host response and curb inflammatory damage to the lung (13) best erectile dysfunction pills review purchase super p-force oral jelly 160 mg amex. Lewiston recommended that surgery be delayed unless symptomatically necessary erectile dysfunction incidence age buy 160mg super p-force oral jelly visa, until the patient is 6-12 years erectile dysfunction related to prostate order super p-force oral jelly 160mg free shipping, because of the possibility of clinical improvement (10). Bronchiectasis has become an uncommon disease in the developed world, but it may often be unrecognized. Prophylaxis, treatment and progress with a follow-up study of 202 cases of established bronchiectasis. Mucociliary transport and ultrastructural abnormalities in Polynesian bronchiectasis. He has a normal physical exam except for an occasional low-pitched, monophonic expiratory wheeze heard best over the sternal notch. Since end exhalation films were unable to be obtained, decubitus films were performed. The right lateral decubitus film (right side down) shows air trapping on the right as evidenced by failure of the mediastinum to shift toward the dependent side. Some reasons for this are related to their developmental age such as: 1) exploration of their environment by putting objects into their mouths; 2) learning to walk and run; 3) inadequate dentition; 4) immature swallowing coordination; and 5) supervision by an older sibling. They also found that children, unlike adults, did not have a significant difference between the foreign body being found in the right or left bronchial tree (2). This may be explained by the fact that children have symmetric bronchial angles until about 15 years of age. At that time, the aortic knob has developed fully, causing the left mainstem bronchus to be displaced, which creates a more obtuse angle at the carina favoring the right mainstem for a foreign body (3). The patient will usually experience choking, gagging, coughing, wheezing, and/or stridor. The second phase is the asymptomatic period that can last from minutes to months following the incident. The duration of this period depends on the location of the foreign body, the degree of airway obstruction, and the type of material aspirated. The ease with which the foreign body can change its location is also a factor in the duration of this period. Airway inflammation or infection from the foreign body will cause symptoms of cough, wheezing, fever, sputum production, and occasionally, hemoptysis. Some of these illnesses are: asthma, croup, pneumonia, bronchitis, tracheomalacia, bronchomalacia, vocal cord dysfunction, or psychogenic cough (4). Although 75% of patients have one or more of these findings, only 40% have all three (5). If stridor (inspiratory and/or expiratory), aphonia, or hoarseness is present, the foreign body is most likely in the larynx or cervical trachea. Since most foreign bodies are not radiopaque, one must rely on indirect findings suggestive of the presence of a foreign body such as: mediastinal shift, atelectasis, and hyperinflation. It has been reported that imaging studies have a sensitivity of 73% and a specificity of 45%, however, up to 20% of patients will have both negative history and radiographic evaluation (6). If the patient presents in the first clinical phase, the family and/or health care professional should be advised to follow the recommendations of the American Academy of Pediatrics and American Heart Association (7). Unless there is a complete airway obstruction, spontaneous coughing and respiration should be the only treatment encouraged. In many such instances, a foreign body is not suspected and the foreign body remains untreated. Even if the patient has expectorated a foreign body, direct visualization is recommended to ensure there are no additional foreign bodies present and to determine if there is any compromise of the airway from inflammation. If there is airway edema and/or inflammation present on direct visualization, a short course of oral corticosteroids may be useful.
The relative risk is the proportion of patients who experienced the adverse outcome in the treatment group as compared to the control group and is expressed as "Y/X" doctor for erectile dysfunction philippines order 160mg super p-force oral jelly amex. A 50% reduction sounds better to most people than a reduction of 5 benadryl causes erectile dysfunction discount 160 mg super p-force oral jelly with mastercard, but in this scenario erectile dysfunction caused by heart medication discount 160mg super p-force oral jelly with amex, the two results represent the same information erectile dysfunction drugs and medicare cheap 160mg super p-force oral jelly visa. It is important to determine whether your patient is similar to the patients who were in the study you are investigating. You now determine that your patient is similar to those enrolled in the study, so the results can be applied to him. The study did not discuss any side effects or risks to the treatment, so the benefits of the treatment seem to outweigh the risks. The second set of guidelines entails the appraisal of articles on diagnostic tests. This includes evaluating whether there was a blind comparison of the test in question with a reference standard. This is important to determine how a new test measures up to the current "gold standard. If the patients in the study differ from the type of patient who would require the test, the study may not be useful. Did the results of the test being evaluated influence the decision to perform the reference standard? Are likelihood ratios for the test results presented or data necessary for their calculation provided? The next step is to ensure that all patients in the study underwent both the test in question and the reference standard. If only patients with abnormal results on the test being evaluated then underwent the reference standard, this would unfairly bias the results of the study, which is known as a "work-up bias. If the test cannot be duplicated, it may be difficult to use in clinical practice. The traditional method of defining the strength of a test is to determine its sensitivity and specificity. Specificity indicates the probability that a patient without a disease will have a negative test (think of this as the true negative rate). The "2x2 table" can also be used to calculate positive and negative predictive values. Although this concept is a very useful and clinically important concept for clinicians, it is mathematically (even with the nomogram) difficult to determine. If the clinical risk is low; however, such as in a fully ambulatory patient with minimal abdominal pain, appendicitis is very unlikely. In other words, if there is a high clinical probability and a positive test, then the patient most likely has that diagnosis. If there is a low clinical probability and a negative test, then the patient is not likely to have that diagnosis. If the clinical probability and the diagnostic test do not agree, then the diagnostic certainty is intermediate. In most situations, clinicians have an appreciation of these probabilities, but the numerical values can be difficult to measure. The last set of steps again involves determining whether the results of the study will help you care for your individual patient. It is important to determine whether the test in question is feasible to perform and interpret in your setting. If a test requires special expertise to perform or interpret, the test may be less useful to you and your patient. It is a tool, just like a stethoscope or history-taking skills, and can be immensely helpful in the day-to-day care of patients. What are the 7 basic steps outlining the evidence-based medicine approach to clinical problems? What are positive and negative likelihood ratios, and how do they differ from sensitivity and specificity? Randomization ensures that both known and unknown factors are evenly distributed between the treatment and control groups, making it more likely that any difference in outcome between the two groups is due to the treatment effect alone. His only physical exercise is at school during recess and physical education classes.
Syndromes
- CT scan or MRI scan of the affected area
- Pneumonia with impaired oxygen uptake (hypoxia)
- Kidney infection
- Nervousness
- The size, shape, or organization of mature cells becomes abnormal. This is also called atypical hyperplasia.
- Edwards syndrome (trisomy 18)
- Difficulty beginning to urinate
Protein-energy malnutrition unfortunately remains a significant problem impotence guilt discount 160mg super p-force oral jelly mastercard, both in developing countries erectile dysfunction hormonal causes safe 160 mg super p-force oral jelly, and in poverty-stricken areas of the industrialized world erectile dysfunction treatment portland oregon cheap 160 mg super p-force oral jelly mastercard. Protein-energy malnutrition may present as the classic syndromes of marasmus and kwashiorkor erectile dysfunction drugs in ayurveda buy cheap super p-force oral jelly 160mg on line, or more commonly, with overlap between the two. Kwashiorkor has been known to occur in toddlers weaned to a protein deficient diet (white rice, yams, cassava-a Latin American staple root otherwise known as manioc or yucca), or in chronically ill or hospitalized patients, in the industrialized world. Those who live in poverty are at increased risk, as are infants, adolescents, pregnant women, alcoholics, and patients with eating disorders. Children whose weights are less than 80% of expected (ideal body weight estimated by tracking growth over time, as well as weight-for-height for infants or body mass index measurements for older children) are considered malnourished. Treatment consists of the provision of adequate calories and protein to meet individual needs, and treatment of any underlying disease states. Vitamin A (2) (retinol, retinol ester, retinal, retinoic acid) is found in both plant and animal sources. Plant sources include green leafy vegetables and some of the yellow vegetables, such as carrots and squash, as well. These also provide provitamins such as betacarotene, which may be further metabolized to vitamin A. Vitamin A functions as an essential component of visual pigments, and has a role in the maintenance of mucus-secreting epithelia, which may contribute to its role in resisting infection. Deficiency syndromes are therefore notable for: impaired vision, particularly at night, xerophthalmia (in which normal epithelium is replaced by keratinized epithelium), squamous metaplasia of the airways leading to secondary pulmonary infections, renal or urinary bladder stones, and immunodeficiencies. This has led to a Red Book recommendation for vitamin A supplementation in some patients with measles (4,5). Vitamin D (2) is found in two precursor forms: 7-dehydrocholesterol (provitamin D3) in the skin, and ergosterol in plants. It is synthesized endogenously from its precursor in the skin, and found in dietary sources such as: deep-sea fish, plants, and grains. Deficiency states are referred to as rickets in children, or osteomalacia in adults. Populations at risk for deficiency states are usually marked by limited sun exposure, and therefore inadequate endogenous synthesis, as well as a diet limited in vitamin D. The classic syndrome of rickets is marked by: craniotabes, rachitic rosary, wrist thickening, pigeon breast deformity, Harrison groove, flaring epiphyses, and bowing of the legs. Deficiency syndromes of vitamin E are extremely uncommon, and are usually seen only in patients with fat malabsorption or other complicating chronic medical conditions. Deficiency syndromes are marked by posterior column/dorsal root ganglion-related signs, including: absent tendon reflexes, ataxia, loss of position and vibration sense, loss of pain sensations. Premature infants, for several reasons, may have persistent need for increased supplementation. Vitamin K supplementation (in addition to other fat-soluble vitamins) is therefore recommended for patients with fat malabsorption, cholestasis, and advanced liver disease (7). Vitamin B1 (2) (active coenzyme thiamine pyrophosphate) is found in a wide variety of dietary sources, with the notable exception of refined foods, such as polished rice, white flour, and white sugar. It also has a role in maintaining membranes and conduction pathways of the peripheral nerves. Several clinical deficiency states have been described, including: dry beriberi (polyneuropathy with toedrop/footdrop/wristdrop), wet beriberi (cardiovascular manifestations including peripheral vasodilation and high output cardiac failure), and Wernicke-Korsakoff syndrome (encephalopathy, with ataxia and psychosis, including retrograde amnesia, confabulation). It is involved in oxidation-reduction reactions, and is incorporated into mitochondrial enzymes. Vitamin B6 (2), or pyridoxine and the phosphorylated forms thereof, is found in almost all foods, though they may be lost after processing (such as dried milk preparations). It acts as a cofactor for a large number of enzymes, including the transaminases, carboxylases, deaminases, in lipid metabolism, amino acid metabolism, and immune responses. The clinical deficiency syndrome is similar to that seen in riboflavin or niacin deficiency: seborrheic dermatitis, cheilosis, glossitis, peripheral neuropathy, and sometimes seizures. Populations at particular risk for deficiency include: neonates (if the maternal diet is deficient), those with insufficient production of intrinsic factor (juvenile pernicious anemia), and those in whom the distal ileum has been surgically removed. The clinical deficiency state may include: Page - 73 megaloblastic anemia, leukopenia, thrombocytopenia, mild jaundice, and neurologic signs, such as posterior/lateral column demyelination, paresthesias, sensory deficits, loss of deep tendon reflexes, confusion, and memory deficits.
Generic super p-force oral jelly 160 mg with mastercard. Erectile Dysfunction is Reversible at Any Age.