Sildenafil
"Cheap sildenafil 50 mg free shipping, erectile dysfunction at age of 20".
By: X. Shakyor, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Clinical Director, Northwestern University Feinberg School of Medicine
Abnormalities in esophageal transport may be due to disruption of peristalsis by a neuromuscular disorder or by an organic obstructing lesion erectile dysfunction injections cost 100 mg sildenafil. Disorders of peristaltic function erectile dysfunction protocol free copy buy 75mg sildenafil with amex, such as achalasia impotence organic origin definition order 75mg sildenafil amex, may occur together with abnormalities in sphincter relaxation are erectile dysfunction drugs tax deductible discount 75mg sildenafil free shipping. Gastroesophageal reflux leads to heartburn and postural regurgitation of food into the mouth. The esophagus and its sphincters function through complex neural, humoral, and myogenic mechanisms. The pharynx, upper esophageal sphincter, and upper third of the esophagus are composed of skeletal muscle. Disorders of skeletal muscle, such as polymyositis, affect the upper portions of the swallowing mechanism. The initiation of peristalsis by swallowing involves both cholinergic and noncholinergic neural pathways as well as myogenic mechanisms. The role of excitatory peptides and hormones, such as cholecystokinin, gastrin, substance P, and motilin, in the physiologic control of the sphincter is not clear, but they may cause the fluctuations in sphincter pressure that follow a meal. The patient usually uses the term "sticks," "pauses," or "hangs up," and often points to the subjective site of arrest with a finger. The sensation of a substernal lump (globus), present one-half hour after eating, is not dysphagia. Dysphagia is never an expression of a purely psychiatric disorder nor a manifestation of hysteria. However, some patients with well-established esophageal disease, such as achalasia, may report that their dysphagia is worse during severe emotional tension. This type of dysphagia is most commonly related to neurologic disease or to pharyngeal muscle weakness. The sensation of dysphagia is localized to the suprasternal notch or substernal region, but the location of the sensation is of little use in localizing the actual site of bolus arrest. Dysphagia for solids can occur either with an organic obstruction (stricture or cancer) or with esophageal motor disorders. If the bolus must be regurgitated, and if an attempt to force the bolus down with water is met by a sudden return of the fluid, then an organic obstruction should be suspected. If the patient is able to force the bolus down by changing their posture, by performing a Valsalva maneuver, by repeated swallowing, or by ingesting fluid, then a motor disorder is more likely. Progressive worsening of dysphagia over weeks to months usually signals the presence of organic narrowing, caused by either a lumen-obliterating carcinoma or a stricture from ongoing reflux esophagitis. Bolus arrest producing dysphagia can sometimes progress to a sensation of pain as esophageal obstruction continues. However, odynophagia usually occurs during the transit of the bolus and disappears once the swallowed material has left the esophagus. It can be of such intensity that the patient refuses to swallow any solids or liquids and expectorates saliva, or it may be mild in intensity, so that the patient is merely aware of the location of the swallowed bolus, as often occurs in patients with reflux disease. Odynophagia can be seen after involvement of the mucosa by reflux, radiation, or viral or fungal infections. Odynophagia can be an uncommon manifestation of carcinoma or of a localized ulcer caused by a lodged tablet. The term "burning" rather than "pain" is usually used, although heartburn can increase in intensity until it is perceived as chest pain. Patients often illustrate heartburn with a movement of the open hand up and down the sternum, as compared with the stationary, tightly clenched fist of angina pectoris. A constant burning unrelieved by antacids may well be of esophageal origin, but it does not represent heartburn. Heartburn is often worse after recumbency or lifting and may follow overeating or alcoholic indiscretion. Sometimes regurgitation is associated with eructation; often it accompanies bending over, lifting, or lying down at night. Regurgitation at night may lead to stridor or to wheezing, a hoarse voice, and other respiratory symptoms from unrecognized reflux. Less commonly, regurgitated fluid is not from the stomach or duodenum but from fluid retained in an achalasic esophagus or in a large pharyngeal diverticulum. In this condition, recently eaten food is propelled back into the mouth from the stomach by a strong contraction of the abdominal wall musculature. The food commonly is rechewed, reswallowed, and again returned to the stomach (see Chapter 227).
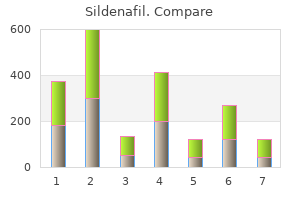
These patients have a survival rate and a response to therapy that are similar to those in Ph1 -positive patients erectile dysfunction news sildenafil 100mg with mastercard. Although 100% of the metaphases on cytogenetic analysis usually show the presence of the Ph1 chromosome how do erectile dysfunction pills work purchase sildenafil 50mg line, some normal stem cells must remain impotence caused by anxiety generic 50mg sildenafil visa. Normal diploid cells emerge on long-term bone marrow culture and after treatment with interferon impotence 27 years old sildenafil 50 mg, high-dose chemotherapy, and autologous bone marrow transplantation. Rarely, bleeding (associated with a low platelet count and/or platelet dysfunction) or thrombosis (associated with thrombocytosis and/or marked leukocytosis) occurs. The serum uric acid level is commonly elevated at diagnosis, and acute gouty arthritis may follow treatment. An elevated blood histamine level (related to the basophil cell mass) can cause upper gastrointestinal ulceration and bleeding. Neutrophil function is usually normal or only modestly impaired, and neutrophil numbers are markedly increased; infections are therefore uncommon at the time of diagnosis. Priapism is occasionally noted, usually in patients with marked leukocytosis or thrombocytosis. Hepatomegaly is less common and is usually minor (1 to 3 cm below the right costal margin). This satisfactory response is transient; all patients eventually develop a variety of changes in the behavior of the disease. Most frequently there is a "blast crisis," a clinical picture resembling that of acute leukemia. Blast crisis is diagnosed when 30% or more blast cells are present in the bone marrow and/or peripheral blood. It is important to be cautious in classifying patients as having blast crisis or accelerated phase because of the adverse prognostic implications. Criteria for accelerated phase are the following: an increase in blast cells (>15%) or basophils (>20%) in the blood or bone marrow, thrombocytopenia (<100,000/muL), serious anemia (hemoglobin [Hb] <7 g/dL); documented extramedullary leukemia, or development of clonal evolution (new chromosomal changes in addition to the Ph1 chromosome). The predominant cells are of the neutrophil series, with a left shift extending to blast cells. The bone marrow is hypercellular with marked myeloid hyperplasia and sometimes shows evidence of increased reticulin or collagen fibrosis. About 15% of patients have 5% or more blast cells in the peripheral blood or bone marrow at diagnosis. The red cells are usually normochromic and normocytic, but nucleated red cells are present in the blood of one fourth of the patients at diagnosis. Serum levels of lactate dehydrogenase, uric acid, and lysozyme are often increased. Kinetic studies show an increased neutrophil production rate related to a markedly expanded myeloid mass. Anderson Cancer Center patients with chronic myelogenous leukemia by phase of disease, 1970-1997. The standard diagnostic test remains the cytogenetic analysis; the presence of the Ph1 chromosome in this clinical setting establishes the diagnosis. The Ph1 chromosome is usually present in 100% of metaphases, ordinarily as the sole abnormality. Ten to 15 percent of patients at initial presentation have an additional chromosomal change, such as loss of the Y chromosome, trisomy 8, an additional loss of material from 22q, or an atypical translocation. Corticosteroids can rarely cause extreme neutrophilia together with the left shift, but this response is self-limited and short in duration and thus seldom a cause of diagnostic difficulty. Patients having agnogenic myeloid metaplasia with or without myelofibrosis have splenomegaly and often have neutrophilia and thrombocytosis. Polycythemia rubra vera with associated iron deficiency, which causes a normal hemoglobin level and hematocrit value, can manifest with an elevated neutrophil and platelet count. The greatest diagnostic difficulty lies with patients who have splenomegaly and leukocytosis but who do not have the Ph1 chromosome. Rarely, patients have myeloid hyperplasia, which involves almost exclusively the neutrophil, eosinophil, or basophilic cell lineage. Isolated megakaryocytic hyperplasia can give rise to a syndrome called idiopathic thrombocythemia with marked thrombocytosis and splenomegaly. This loss of control (accelerated phase) is often associated with an increased proportion of blasts, promyelocytes, and basophils in the peripheral blood and bone marrow and is often accompanied by anemia and thrombocytopenia. Some patients develop bone marrow failure in which anemia and thrombocytopenia are accompanied by increasing evidence of dysplastic changes in the marrow and myelofibrosis.
Purchase 50 mg sildenafil with amex. The Truth About Erectile Dysfunction And 3 Uncommon Cures.
Although the most common cause of hemoptysis is bronchitis erectile dysfunction 23 years old order sildenafil 50 mg on-line, this symptom in a high-risk individual should lead to prompt investigation impotence treatment reviews cheap 50 mg sildenafil with mastercard. Tumors that obstruct major airways can produce wheezing erectile dysfunction protocol real reviews buy sildenafil 25 mg online, and unilateral wheezing suggests a localized obstruction impotence after 40 order sildenafil 100mg with amex. Bronchogenic carcinomas are often associated with cavitation and lung abscess formation, due either to airway obstruction with postobstructive pneumonia or to necrosis of a large tumor mass. Clinical signs particularly indicative of malignancy-associated lung abscess include chronicity of symptoms, lack of high fever, and lack of leukocytosis. Local invasion can produce chest pain, dyspnea from pleural effusion, and symptoms referable to nerves, heart, and great vessels. Malignant pleural effusions occur in approximately 10 to 20% of patients at the time of diagnosis and are most frequently a sign that the tumor is not surgically resectable. Invasion of the pericardium can lead to cardiac tamponade as well as to arrhythmias. The superior vena cava syndrome is characterized by facial suffusion and swelling due to blockage of the superior vena cava by either tumor or associated thrombosis. Although this syndrome is no longer considered a medical emergency, it should be treated promptly. Hoarseness can occur from invasion of the recurrent laryngeal nerve, usually by either tumor directly extending into the mediastinum or by adjacent malignant lymph nodes. The symptom of hoarseness is important because vocal cord paralysis denotes that the tumor is not resectable. The Pancoast syndrome occurs in tumors involving the apex and superior sulcus of the lung and results from local invasion into the brachial plexus as well as the cervical sympathetic nerves. Common sites of metastases of bronchogenic carcinomas include brain, bone, adrenal, and liver. In smokers who present with space-occupying lesions in these sites, the possibility of bronchogenic carcinoma should be immediately considered. In addition, metastatic carcinoma is a frequent cause of cervical and supraclavicular lymphadenopathy. Metastases to skin are relatively rare but are important to recognize clinically because of the ease of making a diagnosis by biopsy. Paraneoplastic syndromes occur in approximately 10% of patients with bronchogenic carcinoma and occasionally are the presenting symptom. Paraneoplastic manifestations can be divided into systemic, endocrine, neurologic, cutaneous, hematologic, and renal categories. Systemic manifestations are often nonspecific and can include weight loss, anorexia, and fever. The endocrine and neurologic manifestations of bronchogenic carcinoma are more specific (see Chapter 194). Digital clubbing is seen in a variety of pulmonary conditions but occurs most commonly in association with bronchogenic carcinoma. Clubbing is caused by soft tissue subungual thickening that most commonly involves the fingernails, resulting in loss of the normal angle between the fingernail and nail bed. In addition, the fingernails are easily compressed against the nail bed and have a spongy feel. Hypertrophic pulmonary osteoarthropathy (see Chapter 194) is often associated with clubbing and commonly presents with exquisite tenderness over the long bones. Invasion of the bone marrow can produce anemia or leukocytosis with a leukoerythroblastic reaction. A significant number of lung cancers are initially detected as an asymptomatic radiographic abnormality, especially a solitary pulmonary nodule (see Chapter 72). Lack of symptoms should not delay evaluation, as these patients are the most likely to be cured by appropriate therapy. In other situations, such as when a relatively low-risk patient presents with an asymptomatic radiographic abnormality, the decision to initiate an evaluation is less clear. When the cell type is in doubt, additional tissue should be obtained for pathologic study. The chest radiograph is the most important radiologic study to diagnose lung cancer. When an abnormality is visualized on a chest radiograph, it is extremely helpful to obtain old chest radiographs if available. The stability of the lesion over time can be very helpful in suggesting either a benign or malignant diagnosis (see.
This may be a partial explanation as to why there is less osteoporosis in obese women can you get erectile dysfunction young age cheap 25mg sildenafil fast delivery. Whether impaired glucose tolerance or frank diabetes ensues depends on the degree of insulin resistance and the underlying genetic make-up of the individual erectile dysfunction utah purchase sildenafil 75mg otc, but both are common erectile dysfunction gene therapy treatment buy 100 mg sildenafil with amex. Slightly low blood cortisol levels may be present in obesity impotence pronunciation sildenafil 25 mg otc, probably because of enhanced turnover rates of cortisol. Urinary free cortisol levels are generally normal if related to the lean body mass or urinary creatinine. Also, obese patients usually suppress normally with dexamethasone (see Chapter 237). Leptin has been found to inhibit the hypothalamic-pituitary-adrenal axis in rodents. It is possible that, if obese humans have peptin resistance, subtle adrenal disinhibition may occur. Pseudotumor cerebri (benign intracranial hypertension) occurs most commonly in obese young women. No intracranial pathology has been found, although headache, blurred vision, and papilledema occur. Hypothalamic control of prolactin and growth hormone is often defective in obesity, with poor responses to insulin hypoglycemia. Whether these pituitary abnormalities reflect altered hypothalamic control due to obesity or abet the obesity in some way is unclear. The responsibility of the physician is to be as supportive and helpful as possible. A truly motivated individual must stay on a diet for a long time, initially for weight loss and then for weight maintenance. It is not possible to calculate a diet under 1100 calories that contains adequate amounts of vitamins and minerals. If the diet is lower in calories than this, vitamin and mineral supplements are necessary. The goal of weight loss is to lose as much fat while losing as little lean body mass as possible. The protein should be of high quality, so that essential amino acids can be utilized to maintain lean body mass. A useful strategy to induce and maintain weight reduction is to educate the obese patient with regard to the caloric content of foods. Particularly important is to emphasize the high caloric density of some foods, especially those high in fat and sugar. Foods high in fiber should be used liberally because of their low caloric density. Refined sugars should be reduced because these provide calories without any useful vitamins or minerals. The concept of protein-supplemented fasting arose because the regimen improves nitrogen balance over fasting programs. There is little evidence, however, that at equicaloric levels protein alone is better than protein with carbohydrate. The extra weight lost early in the diet when protein alone is given is that of water. These very severe diets have been given for extensive periods of time, but it is unwise to allow them to last longer than 16 weeks. These diets, especially those relying on liquid formulas have been popular because of their relative ease and because, since they are so hypocaloric, the weight loss is more rapid. Side effects of these severe diets include orthostatic hypotension (secondary to both sodium loss and impaired norepinephrine secretion), fatigue, cold intolerance, dry skin, hair loss, and menstrual irregularities. Unfortunately, most individuals rapidly regain weight after being on these crash programs, perhaps in large measure because the very low caloric content and the liquid form of the diet do not educate the patient to make the adjustments in lifestyle and eating behavior necessary to subsequently maintain the weight loss. Obese persons tend to be inactive; it is therefore important to increase activity and thus overall energy expenditure. Patients should be taught the approximate number of calories being expended over basal level in individual activities. Most are surprised at how much exercise it takes to expend just a few calories (Table 228-5) (Table Not Available).